
Authors: Joe Walter, MD (@joewalter9999, EM/Hyperbaric Attending Physician, Hennepin County Medical Center/ Healthpartners), R. Eric Minnihan, MD (EM Attending Physician, Hyperbaric Medicine fellow, Mayo Clinic Health System, Hennepin County Medical Center), Tom Masters, MD (EM/Hyperbaric Attending Physician, Hennepin County Medical Center), Chris Logue, MD (EM/Hyperbaric Attending Physician, Hennepin County Medical Center), Bjorn Westgard, MD (EM/Hyperbaric Attending Physician, Hennepin County Medical Center/ Healthpartners), Stephen Hendriksen, MD (EM/Hyperbaric Attending Physician, Hennepin County Medical Center) // Edited by: Alex Koyfman, MD (EM Attending Physician, UT Southwestern Medical Center / Parkland Memorial Hospital, @EMHighAK) & Justin Bright, MD (EM Attending, Henry Ford Hospital, @JBright2021)
Case:
An 82 year-old man with a history of dyslipidemia, hypertension, and CAD s/p stenting was driving home from the grocery store when he experienced sudden vision loss in his right eye around 2:30 pm. He has no previous history of vision problems and is puzzled but eventually concerned. By the time he presents to the ED he has light perception only in his right eye. He cannot not recognize motion. Central retinal artery occlusion (CRAO) is first in the differential.
Introduction:
Central Retinal Artery Occlusion is characterized by a sudden painless loss of vision in one eye. It occurs when there is a blockage of the central retinal artery causing ischemia and infarction to the retina. Incidence is 1-10/100,0001 with a mean age of 60-65 and over 90% of cases occurring in those over 40.2,3,4 Providers are increasingly recognizing this as a cerebral vascular accident that shares the same risk factors commonly associated with stroke: hypertension, hyperlipidemia, diabetes, and tobacco use1. Recent studies have shown that acute cerebral infarcts often accompany CRAO and a marked incidence in stroke and acute myocardial infarction occur in the month following a CRAO.5,6
Pathophysiology/Anatomy:

The first branch off of the internal carotid artery is the ophthalmic artery which splits into the posterior ciliary and central retinal arteries which supply the eye. In CRAO there is an occlusion of the central retinal artery causing a profound vision loss. In some cases the ciliary arteries are able to perfuse the periphery of the retina and maintain perfusion to the central portion of the retina. Research has shown that the retina can only survive 90-100 minutes of ischemia prior to permanent damage.7,8 However, cases with visual recovery beyond this timeframe have been reported, potentially due to incomplete occlusion, an intact cilioretinal artery, or collateral flow.
Etiology:
Although there are many etiologies for CRAO, carotid artery stenosis is thought to be the most common cause and is present in up to 70% of cases.2 Cardioembolic disease is another prevalent etiology and is more likely in those under 40 and in those with a history of atrial fibrillation or valvular disease. Giant cell arteritis, vasculitis, Sickle cell, carotid artery dissection, Moyamoya, hypercoagulable states (SLE, antiphospholipid, hematologic cancers), and iatrogenic causes (injections, cerebral angiogram, carotid endarterectomy) are less common causes of CRAO.
Presentation:
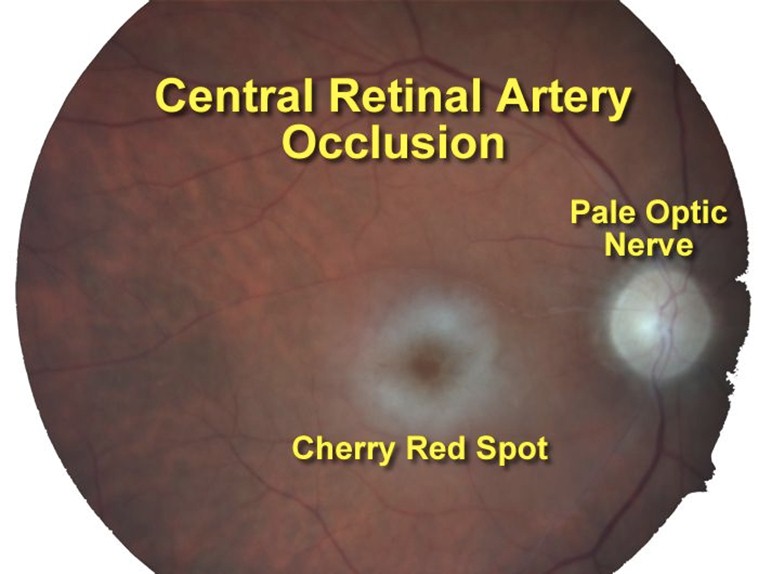
A patient typically presents with acute, profound, painless, monocular vision loss with potentially a small amount of temporal sparing. Approximately 20% of the population has a cilio-retinal artery which can lead to some central sparing in case of a CRAO.7 On exam, patients will demonstrate a complete or relative afferent pupillary defect, though this need not be present. Funduscopic exam will show retinal whitening (a “cherry red spot,” described in 90% of patients with acute CRAO) or “box-carring” (vascular attenuation with stacking of red cells within the vasculature, only seen in 15% of patients with acute CRAO).9
The particular history of past and present illness is important in each patient, as additional symptoms may lead to a specific etiology. Headache and/or temporal tenderness may suggest Giant Cell Arteritis while neck pain or recent cervical trauma may suggest dissection. It is also important to remember the differential diagnosis, which includes occipital stroke, retinal detachment, complex or atypical migraine, and other ischemic optic neuropathies.
Management:
Recent painless vision loss is an ocular emergency that should prompt immediate ophthalmology consultation. Concerns about vasculitis or Giant Cell Arteritis deserve the addition of an ESR/CRP to the workup. A complete stroke and cardiovascular work up is needed either in the ED or during inpatient admission, as there is a high correlation with additional stroke or myocardial infarction in the period immediately following onset of a CRAO (Incident Rate Ratio of 14.0 (95% confidence interval, 8.90-22.00)).5,6 Despite this only one-third of ophthalmologists transfer patients with incident CRAO to an emergency department for immediate evaluation.5
As this in an ophthalmologic emergency, management is usually in coordination with ophthalmology and early consultation is recommended. No clinical trials have demonstrated improvement with any treatment compared with observation10 and historically CRAO has an abysmal prognosis.10,11 Despite the unlikely chance of improvement, maneuvers are usually attempted if a patient presents within 24 hours including:10,12
-
- Ocular massage
- Ocular pressure lowering agents / maneuvers
- Topical agents such as timolol
- IV agents such as acetazolamide or mannitol
- Anterior chamber paracentesis
- Vasodilatory Agents
- Nitroglycerin
- Pentoxifylline
- Isosorbide
- Carbogen
- Breathing into a bag (to increase CO2 which causes vasodilatation)
Again, there is little data to show that any of these methods improve outcomes over control and there is some evidence to suggest that that these interventions may actually be associated with worsened visual outcomes and recovery rates.13
As CRAO is a vaso-occlusive phenomenon, there is a great deal of interest in the use of tPA in its treatment. While there are published reports of vision improvement after the administration of tPA,13 there is debate about whether or not this improvement is greater than the natural history of CRAO.11 Additionally, there is concern regarding hemorrhage associated with the administration of tPA and as such, the use of tPA in patients with CRAO is not currently considered standard of care. As a result of this, the traditional “treatment” of CRAO has been observation alone.11
Hyperbaric Oxygen Experience/Data:
Recently, the undersea and hyperbaric medicine society made a recommendation for the consideration of hyperbaric oxygen therapy (HBOT) in patients with a CRAO.14 While experiencing a CRAO, the inner retinal layers become ischemic due to poor perfusion / oxygenation. Animal models have shown that under hyperbaric conditions, the collateral circulation from the choroid is capable of supplying 100% of the retina’s oxygen needs.15,16 Additionally, as mentioned before, approximately 20% of the population has cilioretinal artery, which supplies blood to the area around the macula. This ability to hyperoxygenate and meet the retina’s oxygen demands while the central retinal artery re-cannulates is part of the rationale behind the use of hyperbaric oxygen. Additional proposed mechanisms are related to hyperbaric oxygen’s effect on edema reduction and its ability to blunt ischemia-reperfusion injury after re-canalization occurs.17
There are a number of clinical trials looking at the effect of hyperbaric oxygen on patients affected by a CRAO. In a literature summary of 476 patients treated with hyperbaric oxygen, 306 (65%) experienced vision improvement after their treatment.18 Overall, the American Heart Association classification of evidence was considered IIB with fair to good evidence with retrospective control case series, but no prospective randomized controlled trials.18 Additionally noteworthy is that therapy with hyperbaric oxygen is generally considered to be benign and safe with proper patient selection and medical control.
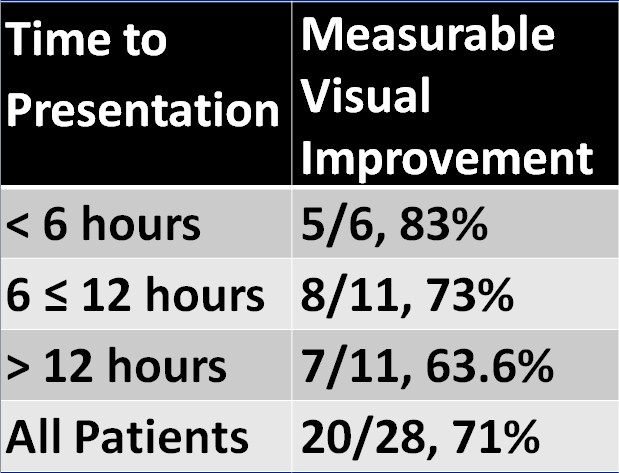
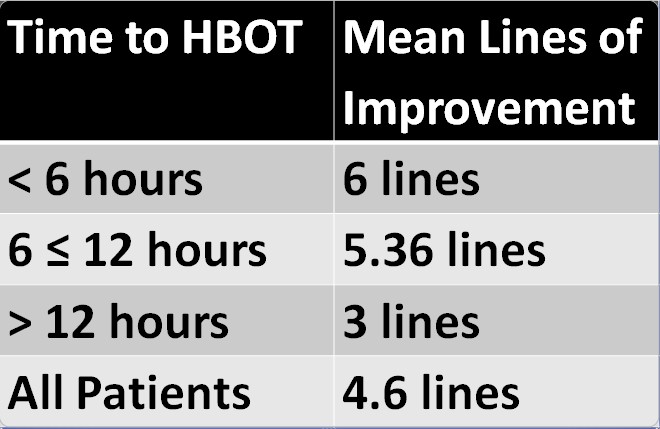
To add to the existing evidence, Hennepin County Medical Center has one of the largest single cohorts of CRAO patients treated with hyperbaric oxygen therapy. Patients found to have a CRAO are being treated with hyperbaric oxygen and seeing significant results. In patients who are treated in <6 hours from time of onset, 83% are seeing improvement in their vision, averaging 6 lines of improvement on a Snellen eye chart. Overall, patients had 4.6 lines of improvement when treated with HBOT.19 Though this is a small and promising study, further investigation is needed. As with all strokes, it appears that time is crucial.
Case Resolution:
Our patient is transferred to a hospital that has emergent hyperbaric capabilities and is evaluated by the Emergency Staff, Neurology and Ophthalmology. CRAO is confirmed and he is taken for hyperbaric oxygen therapy at 9:30 that evening (7 hours after onset of vision loss). During treatment, his vision improves to 20/200 (he can read the big E), and after treatment examination shows that he has improved to 20/100. On examination the following day, he is able to count fingers but is no longer able to read the eye chart. Immediately after his second treatment, he is again 20/100. Ophthalmology evaluation later that day shows a corrected vision of 20/20 -1. The patient reports some small gray spots, but otherwise marked improvement. He is then treated BID for a total of 10 treatments. During his hospitalization he had a stroke work up including an MRI, CTA of the neck and an echo. On reevaluation 6 weeks later, he continues to see 20/20 with correction.
Key Points:
- Presentation: Painless vision loss
- Early ophthalmology consultation (true eye emergency)
- Should be treated as a stroke
- Traditionally poor prognosis overall
- Promising HBO experience thus far. Consider early consultation with an emergent hyperbaric treatment center if available
References / Further Reading
- Leavitt JA, Larson TA, Hodge DO, Gullerud RE. The incidence of central retinal artery occlusion in Olmsted County, Minnesota. Am J Ophthalmol 2011; 152:820.
- Yuzurihara D, Iijima H. Visual outcome in central retinal and branch retinal artery occlusion. Jpn J Ophthalmol 2004; 48:490.
- Park SJ, Choi NK, Seo KH, et al. Nationwide incidence of clinically diagnosed central retinal artery occlusion in Korea, 2008 to 2011. Ophthalmology 2014;121:1933–8.
- Smit RL, Baarsma GS, Koudstaal PJ. The source of embolism in amaurosis fugax and retinal artery occlusion. Int Ophthalmol 1994; 18:83.
- Park et al. Risk and Risk Periods for Stroke and Acute Myocardial Infarction in Patients with Central Retinal Artery Occlusion. Ophthalmology. 2015 Nov;122(11):2336-2343.e2. doi: 10.1016/j.ophtha.2015.07.018. Epub 2015 Aug 19.
- Lee et al. Co-occurrence of acute retinal artery occlusion and acute ischemic stroke: diffusion-weighted magnetic resonance imaging study. American Journal of Ophthalmology. June 2014;157(6):1231-1238.
- Brown GC, Shields JA. Cilioretinal arteries and retinal arterial occlusion. Arch Ophthalmol 1979; 97:84.
- Hayreh SS, Kolder HE, Weingeist TA. Central retinal artery occlusion and retinal tolerance time. Ophthalmology 1980; 87:75.
- Hayreh SS, Zimmerman MB. Fundus changes in central retinal artery occlusion. Retina. 2007;27(3): 276-289.
- Rudkin AK, Lee AW, Aldrich E, et al. Clinical characteristics and outcome of current standard management of central retinal artery occlusion. Clin Experiment Ophthalmol 2010; 38:496.
- Hayreh SS. Ocular vascular occlusive disorders: Natural history of visual outcomes. Progress in Retinal and Eye Research. 2014;41:1-25.
- Tintinalli, Judith, Gabor Kelen, and J. Stephan Stapczynski. Emergency Medicine: A Comprehensive Study Guide -6th Edition. New York: The McGraw-Hill Companies, Inc., 2004. Print.
- Schrag M, Youn T, Schindler J, Kirshner H, Greer D. Intravenous fibrinolytic therapy in central retinal artery occlusion. A patient-level meta-analysis. JAMA Neurology. 2015;72(10):1148-1154.
- Murphy-Lavoie H, Butler F, Hagan C. Arterial Insufficiencies: Central Retinal Artery Occlusion. In: Weaver LK, ed. Hyperbaric Oxygen Therapy Indications. 13th ed. North Palm Beach: Best Publishing Company; 2014.
- Patz A. Oxygen inhalation in retinal artery occlusion. American Journal of Ophthalmology. 1955;40:789-795.
- Li HK, Dejean BJ, Tang RA. Reversal of visual loss with hyperbaric oxygen treatment in a patient with Susac Syndrome. Ophthalmology. 1996;103(12):2091-2098.
- Buras JA, Garcia-Covarrubias L. Ischemia-reperfusion injury and hyperbaric oxygen therapy. Basic mechanisms and clinical studies. In: Neuman TS, Thom SR, eds. Physiology and Medicine of Hyperbaric Oxygen Therapy. 1st ed. Philadelphia, PA: Saunders Elsevier; 2008.
- Murphy-Lavoie H, Butler F, Hagan C. Central retinal artery occlusion treated with oxygen: a literature review and treatment algorithm. Undersea and Hyperbaric Medicine. September-October 2012;39(5):943-953.
- Masters T, Westgard B, Hendriksen S, Walter J, Logue C. Central retinal artery occlusion treated with hyperbaric oxygen. A retrospective review. Paper presented at: UHMS Annual Scientific Meeting, 2015; Montreal.






4 thoughts on “Central Retinal Artery Occlusion”
Thanks for this. We also treat crao with hbo at ummc and have seen mixed results. Early dx and off to the chamber within 6 to 12 hours is key. Do you know what Protocol Hennipin uses?
We do BID treatments at 2.5 ATA (first one at 2.8 ATA) for 5 days (10 treatments total).