Author: Timothy Hanaway, MD (Flight Surgeon, USAF) // Edited by: Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UT Southwestern Medical Center / Parkland Memorial Hospital) and Brit Long, MD (@long brit)
Case
It is an especially busy day in the ED, and a 54-year-old male is placed in a room. He informs you that approximately 1 week ago he noticed some slight pain and swelling in his left lower leg. The patient also reports that he thinks his leg is also slightly red, and over the past week the pain and swelling has significantly worsened. He also tells you he is a truck driver, and he heard of some other truck drivers having a similar problem. His vital signs are normal, and upon examination you see clear edema of the left lower leg compared to the right, and the leg appears mildly erythematous.
Background
Deep Vein Thrombosis (DVT) is not a stranger to the emergency physician and can be a significant diagnosis, with nearly half of patients diagnosed with DVT in the ED being admitted (1). A form of Venous Thromboembolism (VTE), a DVT is defined as the formation of one or more blood clots, or thrombi, in one of the body’s large veins, most commonly in the lower limbs (2). Symptoms include pain, swelling, tenderness, discoloration, redness, and skin that is warm to the touch (2).
Where do DVTs occur? Most commonly, the superficial femoral and popliteal veins of the thigh and the posterior tibial and peroneal veins of the lower leg. Patients often never realize a DVT is present, as the DVT may not extend and is usually broken up via fibrinolysis naturally. However, when this does not occur, the DVT can extend into the iliac veins and even up to the inferior vena cava. The veins in the upper extremities can also be affected, but this usually is due to a preceding event or presence of an intravenous catheter (29).
There are two main types of DVTs: provoked and unprovoked. A provoked DVT is defined as a DVT caused by a known event (prolonged immobility, recent surgery, instrumentation to the area, etc.). An unprovoked DVT is defined as a DVT arising from no identifiable environmental event. Approximately 25-50% of DVTs are unprovoked and approximately 50% provoked, most commonly relating to malignancy and surgery (8).
Laboratory testing with a D-Dimer can be helpful in some cases of DVT; however, the D-Dimer has limitations in DVT. With a high sensitivity and low specificity, it can be useful in ruling out a DVT, but a positive result is not diagnostic. D-Dimer can be elevated in a significant number of other disease states (sepsis, malignancy, infection, trauma, etc.) (30). But, we’re in luck, as there is an excellent scoring system for assessing DVT risk: the Wells score.
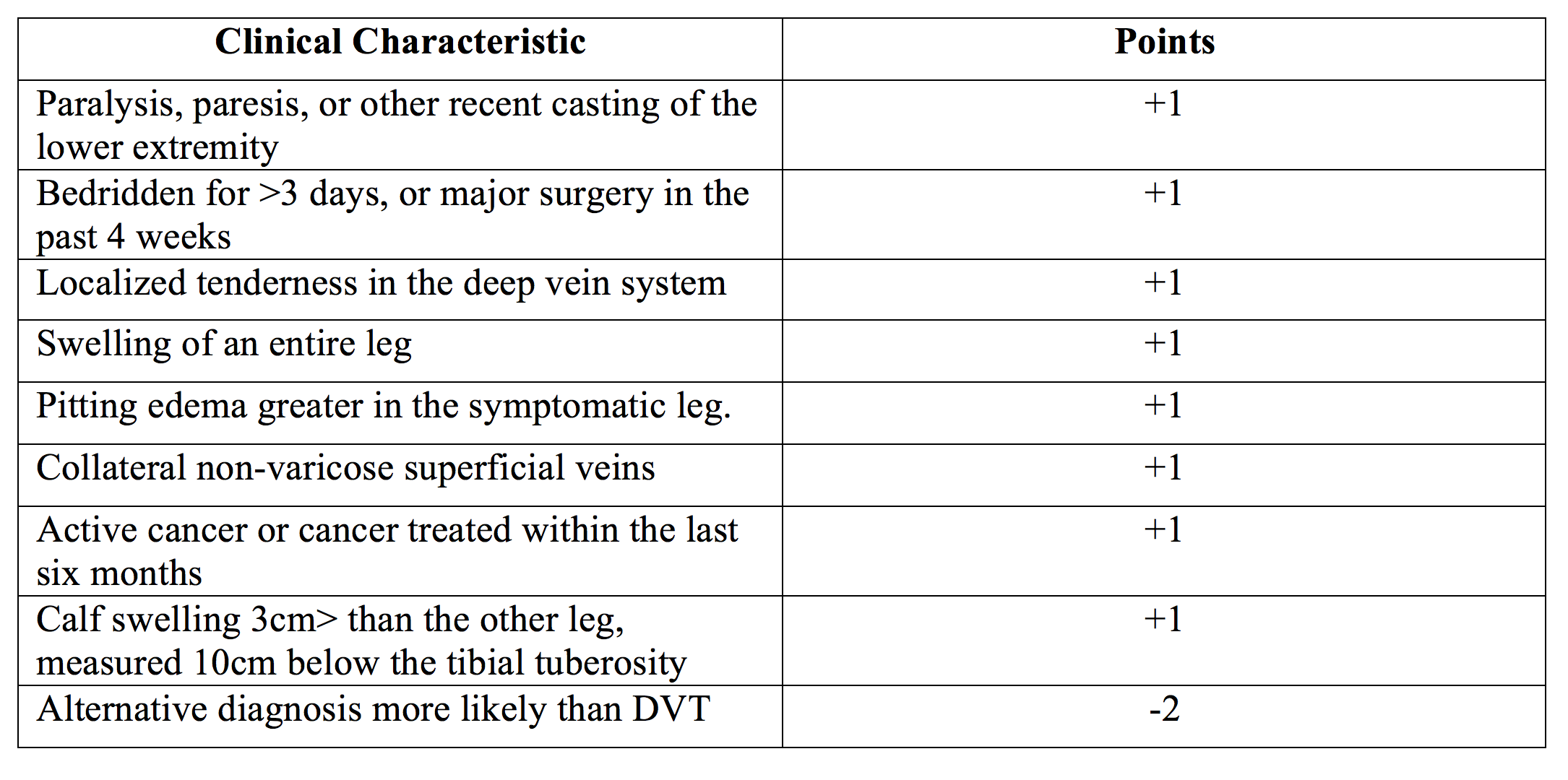
The Wells score includes a gambit of clinical characteristics, with each adding or subtracting to the clinician’s suspicion for a DVT. Patients can be classified into three categories based on the Wells Score; Low Risk (score of 0 or less), Moderate Risk (score of 1-2), and High Risk (score of 3 or more). This is an excellent tool, with some studies showing a 100% sensitivity in low risk patients and a 100% negative predictive value in patients with a moderate-high risk classification (3). The Modified Wells score adds one additional point onto the original for a history of DVT, and other than classifying patients into low, moderate, and high risk, only classifies by DVT likely (2 or more points), or DVT unlikely (3 or more points).
So you’ve classified your patient as low risk with a Wells score of 0 or less. Now what? The answer to this is highly dependent on the patient. For low risk patients, a D-Dimer should be performed. If the D-Dimer is negative, no further testing is indicated, and a DVT can be ruled out. However, if the D-Dimer is positive, or if the D-Dimer is suspected to be positive for another reason (concurrent recent surgery for example), then an ultrasound should be performed, as detailed below. Moderate risk patients follow the same algorithm; however there is some question whether these patients should proceed directly to ultrasound. High risk patients present the simplest medical decision making; if a patient has a high- risk Wells score, an ultrasound should be performed without a D-Dimer, as a negative D-Dimer in these patients cannot reliably rule out a DVT (31).
The Wells score is not the end of the line, however. The diagnostic choice for patients with a suspected DVT is compression ultrasonography (US). A meta-analysis in 2005 comparing venography to US, specifically compression US, revealed that compression US alone had a sensitivity of 93.8% for proximal DVT, and a 56.8% for distal DVT, with a specificity of 97.8% (7). Of note, the most sensitive aspect of compression US in diagnosing DVT is the lack of compressibility of the vein, and this criterion alone has been shown to be effective in DVT diagnosis (9).
Does this mean that all patients with a warm, swollen extremity get a D-Dimer, Wells stratification, and a compression US? Of course not. There are a number of equally important pathologies that can mimic a DVT, and without careful thought and thorough medical decision making, the clinician could overlook a potentially life threatening diagnosis.
Emergent Mimics
ACUTE ARTERIAL OCCLUSION
Acute arterial occlusion, or acute limb ischemia, is defined as a sudden decrease in extremity perfusion leading to potential loss of the limb. This is usually due to a thrombus becoming dislodged from a more proximal vessel and leading to an embolic event in the limb, but it may also arise from an acute thrombus in the limb or from direct trauma to the artery. The most common artery involved is the femoral, with the arteries in the upper extremities a close second (10).
Differentiating a DVT from an acute arterial occlusion can usually be done with focused history and exam. An arterial occlusion will typically present dramatically, with a previously healthy limb immediately developing symptoms to ischemia. This acute presentation can be confounded in the patient with underlying chronic vascular disease, as collateral vessels previously formed allow for blood flow around the occluded artery. In these cases in particular, the Six P’s can be useful. These physical exam findings are paresthesia, pain, pallor, poikilothermia (inability to regulate temperature, i.e. a cold limb), and paralysis.
If an acute arterial embolism is diagnosed, anticoagulation and surgery are the mainstays of treatment, in conjunction with a vascular surgeon. The STILE trial showed a difference between the two therapies in relation to how long the limb had been ischemic. If the duration was 14 days, surgical revascularization was superior (11, 12). This information further supports a careful history, particularly to the onset and duration of symptoms, when thinking about acute limb ischemia.
PHLEGMASIA CERULEA DOLENS
Phlegmasia cerulean dolens (PCD) is a complication of a routine lower extremity DVT that should always be considered. PCD is defined as a massive iliofemoral DVT associated with limb threatening ischemia or symptomatic, serious edema and is part of a clinical spectrum ranging from phlegmasia alba dolens (“milk leg”) to frank venous gangrene. PCD when unrecognized and untreated can result in gangrene, amputation, circulatory collapse, and death (32).
All patients with a DVT have the potential to develop PCD; however, it is much more common in the fifth and sixth decades of life and in patients with an underlying malignancy. The majority of PCD occurs in the lower extremities, particularly the left leg, due to compression of the overlying artery (27). Patients can present with acute or gradual symptoms usually beginning with pain, edema, and blanching of the extremity (“milk leg”). Symptoms progress to severe, constant pain and cyanosis. Cyanosis beginning distally and progressing proximally is strongly suggestive for PCD.
Although the above presentation and symptoms are striking, exam and history alone should not be used to diagnose PCD. Ultrasonography should always be performed to confirm the diagnosis, as the treatment for PCD comes with serious considerations. PCD is the only DVT manifestation which indicates immediate thrombolysis via systemic or catheter-directed therapy, and possible surgical intervention (28). As such, vascular surgery and interventional radiology should be consulted as soon as PCD is confirmed. However, if these specialties are not readily available, intravenous unfractionated heparin should not be delayed.

COMPARTMENT SYNDROME
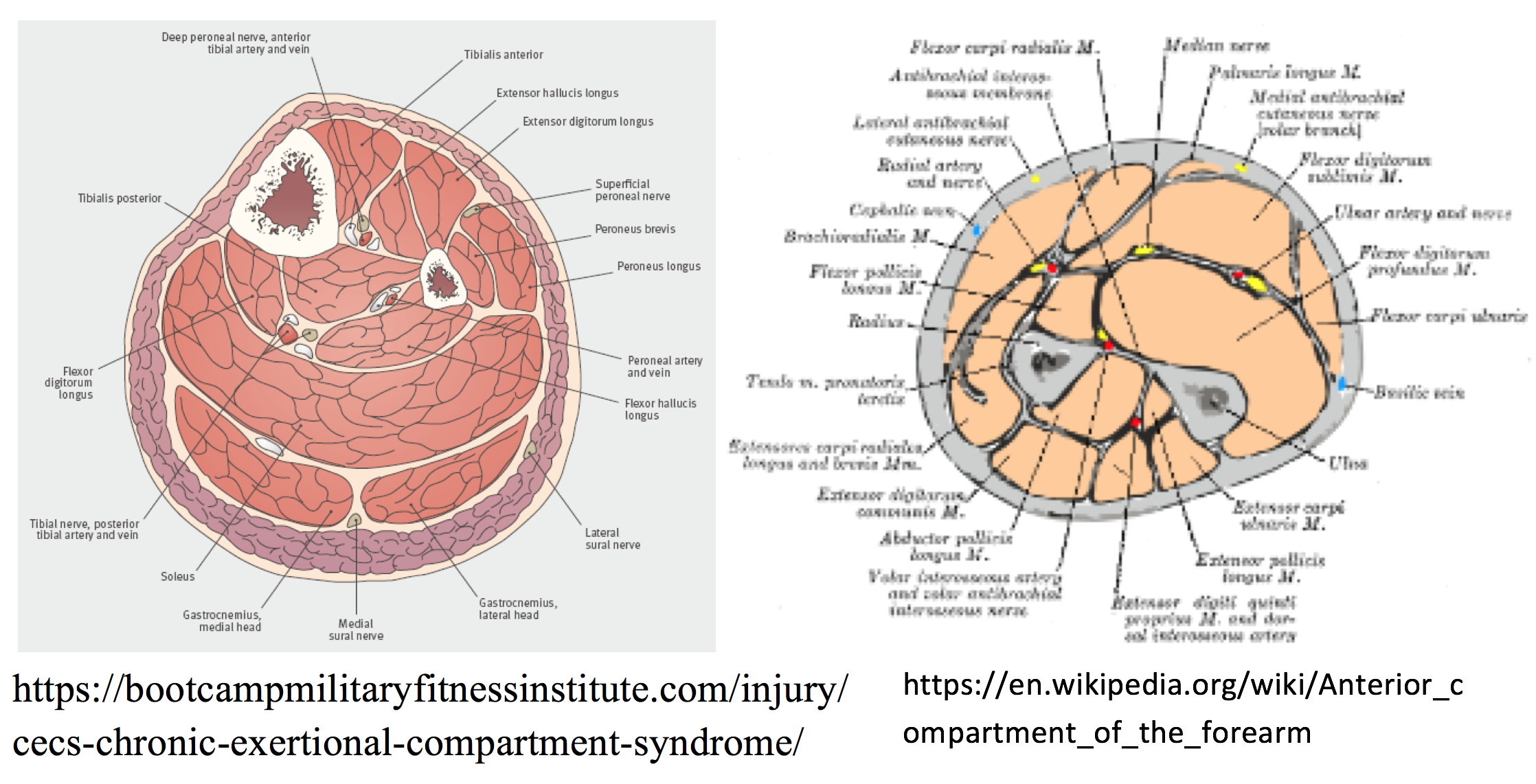
Acute Compartment Syndrome typically develops soon after a trauma, such as a long bone fracture (open or closed fracture) or a muscle rupture. After the injury, pressure in the compartment (typically forearm or leg) builds, and given the surrounding rigid fascia of the compartment, the pressure eventually rises to the extent that circulation and tissue function within the space is compromised (13).
The symptoms of compartment syndrome depend on which compartment is affected. The leg and the forearm both consist of 4 compartments, and each can develop compartment syndrome. In general, the symptoms include pain (particularly with stretching the muscles of the affect compartment), paresthesia, palpable tensity, and potentially pulselessness.
Compartment syndrome is a surgical emergency. Consulting with Orthopaedic Surgery or immediate transfer to a capable facility should be performed, as the definitive treatment for compartment syndrome is fasciotomy, with hyperbaric oxygen being a potential adjunct (14).
NECROTIZING FASCITIS
Necrotizing fasciitis describes forms of myositis, fasciitis, and cellulitis that lead to necrosis of tissue. There are two main types, I and II, with type I being a multi-organism infection, and type II (“streptococcal gangrene”) arising typically from Streptococcal species, most commonly Group A Streptococcus (15, 16). Type III is due to clostridial species.
The extent of necrotizing infection can be difficult to determine. Necrotizing cellulitis features dark, thin, pungent drainage, concurrent with crepitus of the skin caused by tissue gas formation (17). Deeper infection can be insidious, as the infection spreads along with deep, poorly vascularized fascia. Borderless erythema, warmth, edema, and pain out of proportion to exam should key the clinician in to possible necrotizing fasciitis (18).
Much like compartment syndrome, early surgical consultation is key. If necrotizing infection is suspected, no laboratory testing nor imaging should delay this early consultation. In addition, a triple antibiotic regimen should be administered once the diagnosis is confirmed, consisting of a carbapenem or beta-lactam-beta-lactamase inhibitor, clindamycin, and a MRSA active antibiotic (19).
URGENT MIMICS
CONGESTIVE HEART FAILURE
Congestive Heart Failure (CHF) is due to a functional of structural cardiac pathology that results in impaired ventricular output commonly leads to leg edema. This decreased ventricular output causes a backup in the venous system and decreased renal blood flow, resulting in third spacing of fluid, commonly into the lower extremities. Typically, almost universally, the resultant lower extremity edema in CHF is bilateral. More distinguishing features include pulmonary congestion, murmur (i.e. S3 gallop), and an elevated creatinine from baseline (33).
CELLULITIS
Cellulitis is the result of bacterial entrance into the superficial tissue as a result of defects in the skin barrier. Clinically, cellulitis can easily mimic a DVT, presenting with a similar onset duration, warmth, discoloration, tenderness to palpation, and edema. Cellulitis is typically also seen unilaterally. A key distinguishing factor in cellulitis is a more clearly demarcated erythematous area, whereas this will not be seen in a DVT. Ultrasonography may be considered with cellulitis as well if a deeper infection or an abscess is suspected, but remember, do not delay surgical consultation for imaging if a deep, necrotizing infection is on the differential (20).

VASCULITIS
Vasculitis is a very general term, referring to a large group of vascular diseases. Major categories in the group are large vessel vasculitis such as Giant cell arteritis, medium vessel such as polyarteritis nodosa, and small vessel such as Wegner’s Vasculitis. Patients with a vasculitis commonly have an insidious onset, with some systemic symptoms such as fever, malaise, athralgias, and weight loss, along signs of sensory or motor neuropathies, palpable purpura, and abnormalities in detectable pulses (bruits, tender pulses, or diminished pulses). Examination of pulses and palpation of arteries can be extremely helpful in identifying large-vessel vasculitis (21).
NEPHROTIC SYNDROME
Nephrotic Syndrome is defined as 24-hour urine protein excretion of more than 3.5 grams with peripheral edema and low serum albumin. It can be caused by multiple etiologies, including minimal change disease, focal segmental glomerulosclerosis, and amyloidosis. With reduced oncotic pressure, dependent areas accumulate fluid, leading to periorbital and pedal edema, worse in the morning. Skin changes are not common with nephrotic syndrome. Of note, nephrotic syndrome can lead to a hypercoagulable state (the cause of which is poorly understood), and this syndrome may lead to DVT (22, 23). Increased risk of infection is also present.
LYMPHEDEMA
Lymphedema results from pooling of interstitial fluid and fibro-adipose tissue secondary to a defect, primary or secondary, of the normal lymphatic system. Although lymphedema can be primary in nature (without an inciting factor), secondary lymphedema is much more common. Patients generally will present with unilateral, non-pitting, slowly developing edema of an extremity, and will have a history of some form of lymph node dissection at the proximal aspect of the limb (24).

VENOUS STASIS
Venous stasis is a common disease, affecting up to 50% of the population (25, 26). Caused by venous valve reflux, poor muscle pump function, and small venous thrombi, venous stasis is a progressive disease that eventually results in characteristic skin changes, dilated veins, and ulcerations. Leg heaviness, fatigue, and pain are hallmark features of venous stasis. Distinguishing from a DVT, venous stasis will present with symptoms progressing over an extended period, months to years. Patients with a history suggestive of DVT with pre-existing venous stasis present a difficult case, and therefore the possibility if DVT should not be ruled out by the presence of chronic venous stasis.
BAKER’S CYST
Baker’s cysts are popliteal synovial cysts and are very common. Caused by enlargement of the gastrocnemius-semimembranosus bursa, Baker’s cysts typically present with edema in the popliteal fossa. Baker’s cysts are usually the result of trauma or pre-existing knee pathology, such as osteoarthritis or rheumatoid arthritis. DVT and Baker’s cyst can usually be differentiated upon exam, but if the Baker’s cyst has ruptured, dissected, or massively enlarged into the lower leg, the symptoms of discoloration, pain, and edema in the lower leg closely resemble DVT. As such, the ever-important ultrasonography should be performed to distinguish between the two (34).
Summary
• Lower extremity unilateral edema is a hallmark of a deep vein thrombosis.
• Risk factors of DVT include malignancy, prolonged immobilization, and recent surgery.
• Emergent mimics of a DVT include acute arterial occlusion, phlegmasia cerulea dolens, compartment syndrome, and necrotizing fasciitis, with less emergent mimics including congestive heart failure, cellulitis, vasculitis, nephrotic syndrome, lymphedema, venous stasis, and Baker’s cyst.
• If DVT is suspected, compression ultrasonography must be performed for diagnosis.
References / Further Reading:
1. Singer AJ, Thode HC, Peacock WF. Admission rates for emergency department patients with venous thromboembolism and estimation of the proportion of low risk pulmonary embolism patients: a US perspective. Clinical and Experimental Emergency Medicine. 2016;3(3):126-131.
2. Office of the Surgeon General (US); National Heart, Lung, and Blood Institute (US). The Surgeon General’s Call to Action to Prevent Deep Vein Thrombosis and Pulmonary Embolism. Rockville (MD): Office of the Surgeon General (US); 2008. INTRODUCTION: Definitions of Deep Vein Thrombosis and Pulmonary Embolism.
3. Modi S, Deisler R, Gozel K, et al. Wells criteria for DVT is a reliable clinical tool to assess the risk of deep venous thrombosis in trauma patients. World Journal of Emergency Surgery : WJES. 2016;11:24. doi:10.1186/s13017-016-0078-1.
4. Johnson SA, Stevens SM, Woller SC, Lake E, Donadini M, Cheng J, Labarère J, Douketis JD. Risk of Deep Vein Thrombosis Following a Single Negative Whole-Leg Compression UltrasoundA Systematic Review and Meta-analysis. JAMA. 2010;303(5):438-445. doi:10.1001/jama.2010.43
5. Weber J. Venous Thromboembolic Disease. J Am Osteopath Coll Radiol. 2014;3(3):2-7.
6. Chu C-M, Chen K-C, Wang T-L. Ultrasound performed by emergency clinician improved the diagnostic efficacy in deep vein thrombosis. Critical Ultrasound Journal. 2015;7(Suppl 1):A28. doi:10.1186/2036-7902-7-S1-A28.
7. Goodacre et al. Systematic review and meta-analysis of the diagnostic accuracy of ultrasonography for deep vein thrombosis. BMC Medical Imaging 2005. 10.1186/1471-2342-5-6.
8. White R. The Epidemiology of Venous Thromboembolism. Circulation. 2003;107:I-4-I-8
9. Anthonie W.A. Lensing, M.D., Paolo Prandoni, M.D., Dees Brandjes, M.D., Peter M. Huisman, M.D., Mario Vigo, M.D., Giovanni Tomasella, M.D., Jelmer Krekt, M.D., Jan Wouter ten Cate, M.D., Ph.D., Menno V. Huisman, M.D., Ph.D., and Harry R. Büller, M.D., Ph.D. Detection of Deep-Vein Thrombosis by Real-Time B-Mode Ultrasonography. N Engl J Med 1989; 320:342-345
10. Abbott WM, Maloney RD, McCabe CC, et al. Arterial embolism: a 44 year perspective. Am J Surg 1982; 143:460.
11. Results of a prospective randomized trial evaluating surgery versus thrombolysis for ischemia of the lower extremity. The STILE trial. Ann Surg 1994; 220:251.
12. Weaver FA, Comerota AJ, Youngblood M, et al. Surgical revascularization versus thrombolysis for nonembolic lower extremity native artery occlusions: results of a prospective randomized trial. The STILE Investigators. Surgery versus Thrombolysis for Ischemia of the Lower Extremity. J Vasc Surg 1996; 24:513.
13. Matsen FA 3rd, Krugmire RB Jr. Compartmental syndromes. Surg Gynecol Obstet 1978; 147:943.
14. Wattel F, Mathieu D, Nevière R, Bocquillon N. Acute peripheral ischaemia and compartment syndromes: a role for hyperbaric oxygenation. Anaesthesia 1998; 53 Suppl 2:63.
15. Brook I, Frazier EH. Clinical and microbiological features of necrotizing fasciitis. J Clin Microbiol 1995; 33:2382.
16. Bisno AL, Stevens DL. Streptococcal infections of skin and soft tissues. N Engl J Med 1996; 334:240.
17. MACLENNAN JD. The histotoxic clostridial infections of man. Bacteriol Rev 1962; 26:177.
18. Stevens DL, Tanner MH, Winship J, et al. Severe group A streptococcal infections associated with a toxic shock-like syndrome and scarlet fever toxin A. N Engl J Med 1989; 321:1.
19. Stevens DL. Streptococcal toxic-shock syndrome: spectrum of disease, pathogenesis, and new concepts in treatment. Emerg Infect Dis 1995; 1:69.
20. Barbic D, Chenkin J, Cho DD, et al. In patients presenting to the emergency department with skin and soft tissue infections what is the diagnostic accuracy of point-of-care ultrasonography for the diagnosis of abscess compared to the current standard of care? A systematic review and meta-analysis. BMJ Open 2017; 7:e013688.
21. Grayson PC, Tomasson G, Cuthbertson D, et al. Association of vascular physical examination findings and arteriographic lesions in large vessel vasculitis. J Rheumatol 2012; 39:303.
22. Rabelink TJ, Zwaginga JJ, Koomans HA, Sixma JJ. Thrombosis and hemostasis in renal disease. Kidney Int 1994; 46:287.
23. Lionaki S, Derebail VK, Hogan SL, et al. Venous thromboembolism in patients with membranous nephropathy. Clin J Am Soc Nephrol 2012; 7:43.
24. Szuba A, Shin WS, Strauss HW, Rockson S. The third circulation: radionuclide lymphoscintigraphy in the evaluation of lymphedema. J Nucl Med 2003; 44:43.
25. Zahariev T, Anastassov V, Girov K, et al. Prevalence of primary chronic venous disease: the Bulgarian experience. Int Angiol 2009; 28:303.
26. Brand FN, Dannenberg AL, Abbott RD, Kannel WB. The epidemiology of varicose veins: the Framingham Study. Am J Prev Med 1988; 4:96.
27. Haimovici H. The ischemic forms of venous thrombosis. 1. Phlegmasia cerulea dolens. 2. Venous gangrene. J Cardiovasc Surg (Torino) 1965; 5:Suppl:164.
28. Casey ET, Murad MH, Zumaeta-Garcia M, et al. Treatment of acute iliofemoral deep vein thrombosis. J Vasc Surg 2012; 55:1463.
29. Palareti G, Cosmi B, Lessiani G, et al. Evolution of untreated calf deep-vein thrombosis in high risk symptomatic outpatients: the blind, prospective CALTHRO study. Thromb Haemost 2010; 104:1063.
30. Lee AY, Julian JA, Levine MN, et al. Clinical utility of a rapid whole-blood D-dimer assay in patients with cancer who present with suspected acute deep venous thrombosis. Ann Intern Med 1999; 131:417.
31. Constans J, Nelzy ML, Salmi LR, et al. Clinical prediction of lower limb deep vein thrombosis in symptomatic hospitalized patients. Thromb Haemost 2001; 86:985.
32. Sarwar S, Narra S, Munir A. Phlegmasia cerulea dolens. Tex Heart Inst J 2009; 36:76.
33. Marwick TH. The viable myocardium: epidemiology, detection, and clinical implications. Lancet 1998; 351:815.
34. Fritschy D, Fasel J, Imbert JC, et al. The popliteal cyst. Knee Surg Sports Traumatol Arthrosc 2006; 14:623.





1 thought on “DVT Mimics: What should the emergency physician consider?”
Pingback: Länkar v34-35 | Internmedicin