
Authors: Brannon Inman, MD (EM resident, San Antonio, TX) and Lloyd Tannenbaum, MD (EM Attending Physician, San Antonio, TX) // Reviewed by: Alex Koyfman, MD (@EMHighAK) and Brit Long, MD (@long_brit)
Case:
During a bustling emergency medicine shift, a mom presents to the ER via her pediatrician’s request with Bubba, a 4-month-old previously “healthy”, ex-term, fully immunized baby boy. Baby boy Bubba was referred to the ED with a chief complaint of worsening poor feeding, irritability, and failure to thrive according to his pediatrician. Mom also notes Bubba has been having recurrent episodes of wheezing, and has been having a week of “viral-like symptoms.” He was also diagnosed with asthma 1 week ago. During your initial evaluation, he appears listless but arousable. He is much less active than expected for a child of this age. He is tachycardic, with a HR in the 190’s. On exam, you note a mildly dehydrated, thin child, smaller than expected for the stated age, with rhinorrhea, wheezing, and hepatomegaly. You also note a diastolic murmur best appreciated at the cardiac apex.
You see the following ECG:

Figure 1: Adapted from Electrocardiogram of Anomalous Left Coronary Artery From the Pulmonary Artery in Infants 1
Notice anything strange about this ECG?
Let’s zoom in on the various leads:

Figure 2: Adapted from The caveats in the diagnosis of anomalous origin of the left coronary artery from the pulmonary artery (ALCAPA)
Notice how there are very deep q waves in leads I, aVL, and V3-V6. You think to yourself: “Self, why does this baby have signs of anterolateral ischemia, poor feeding, wheezing, and failure to thrive? Could it be myocarditis?”. Maybe, but it could also an Alpaca!
Wait, ALCAPA!
Anomalous Left Coronary Artery from the Pulmonary Artery (ALCAPA)
Anomalous left coronary artery arising from the pulmonary artery (ALCAPA), AKA Bland-White-Garland syndrome is a relatively uncommon albeit life-threatening ideology that occurs in approximately one in 300,000 live births. Left untreated, the mortality rate of ALCAPA can approach 90%, with most children dying in the first year of life.2–4 Early in infancy, the patient continues to have elevated pulmonary vascular resistance thus often having a lesser degree of symptoms.3 However, later in life, as vascular pressure decreases, blood flow via the left corner artery is effectively stolen and transmitted back to the pulmonary artery. This steal phenomenon occurs because the pressure in the pulmonary artery is less than the pressure in the left coronary artery during systole.3 This results in chronic ischemia of the myocardium perfused by the left corner artery. Some children eventually develop collateral blood flow which can augment the degree of chronic ischemia and may lead to alterations in presentation, however to some degree chronic LCA distribution ischemia is a part of the natural history of ALCAPA. Ultimately this results in symptoms of congestive heart failure, left ventricular dysfunction, mitral regurgitation, arrhythmias, and death.3 Frequently the condition results in a dilated cardiomyopathy, which fortunately typically improves after surgical correction.5
The ECG findings of ALCAPA are those typical of anterolateral ischemia and often resemble old infarction. Deep q waves are often present in I, aVL, and V3-6 (Figure 2).4–6 Q waves are not typically present in the inferior leads, though they may be seen in lead II. Q waves in lead III are not suggestive of ALCAPA.7 ST-segment elevations are often accompanied by deep q waves in the anterolateral leads.6 Other common ECG findings include loss of R waves height in precordial leads and poor R wave progression, often with accompanying ST/T wave changes.7
Diagnostics typically involve an echocardiogram and CT angiogram (Figures 3 and 4). Management is surgical.2,3,5

Figure 3: from ALCAPA—A Reversible Cause of Dilated Cardiomyopathy in Infants: Echocardiogram showing LCA arising from the PA.
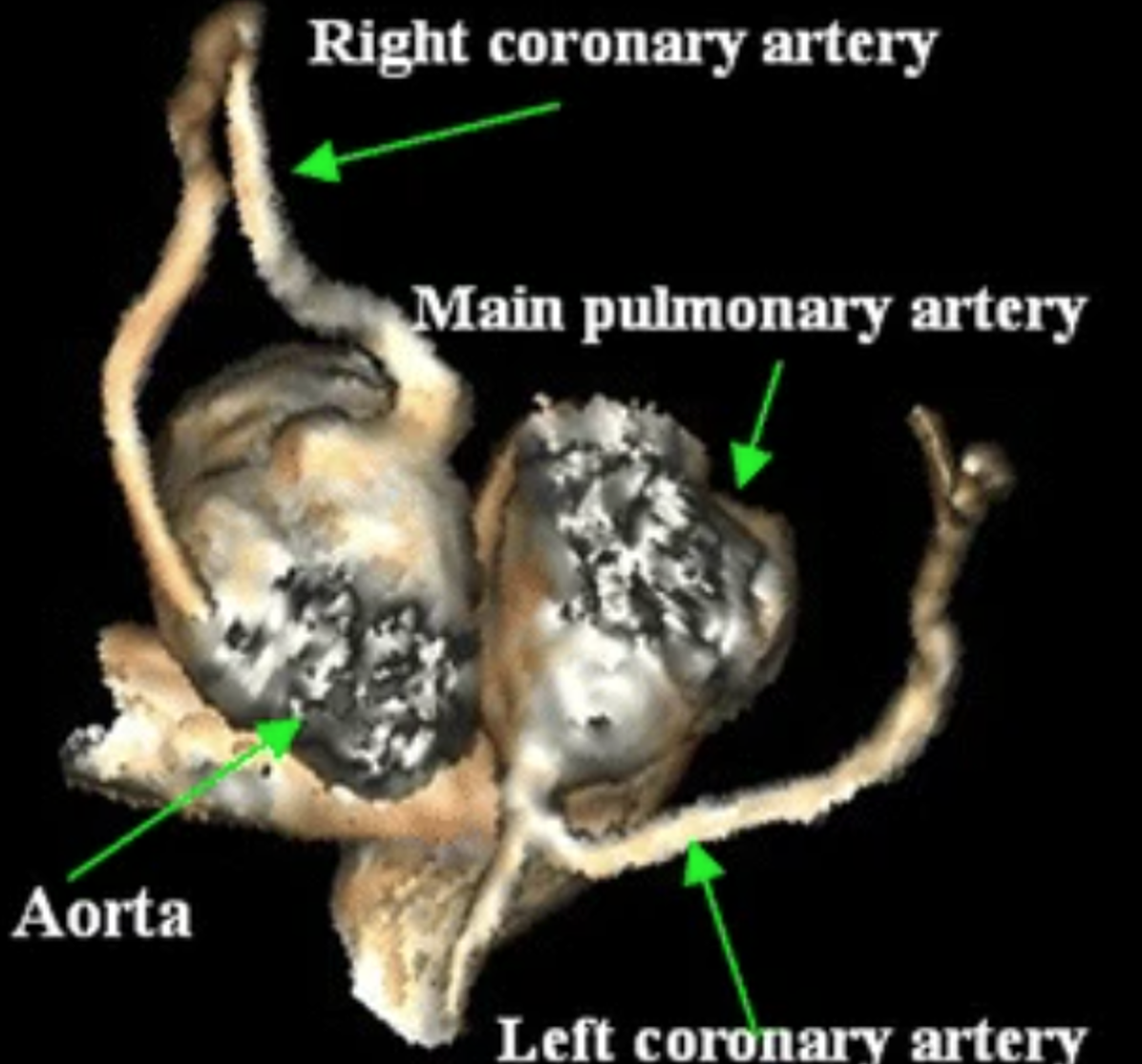
Figure 4: from Anomalous origin of the left coronary artery from the pulmonary artery (ALCAPA) in a newborn: CT angiogram reconstruction showing LCA arising from the PA
Key points:
- ALCAPA is an uncommon though life-threatening cardiac abnormality.
- ALCAPA is commonly misdiagnosed as myocarditis.3
- When a child presents with recurrent asthma/wheezing and failure to thrive consider ALCAPA.3
- Suspect ALCAPA if there are anterolateral Q waves, ST/T waves changes, loss of R wave height, or abnormal R wave progression in the precordial
- ED management is admission for further diagnostics (Echocardiogram and CT angiogram) and definitive management is surgical.
ALCAPA kills people:

Figure 5: Adapted from Paul the llama, from Llamas with Hats.
References/Further Reading:
- Hoffman JIE. Electrocardiogram of anomalous left coronary artery from the pulmonary artery in infants. Pediatric Cardiology. 2013;34(3):489-491. doi:10.1007/s00246-012-0599-7
- al Umairi RS, al Kindi F, al Busaidi F. Anomalous origin of the left coronary artery from the pulmonary artery: The role of Multislice computed tomography (MSCT). Oman Medical Journal. 2016;31(5):387-389. doi:10.5001/omj.2016.77
- Levitas A, Krymko H, Ioffe V, Zalzstein E, Broides A. Anomalous left coronary artery from the pulmonary artery in infants and toddlers misdiagnosed as myocarditis. Pediatric Emergency Care. 2016;32(4):232-234. doi:10.1097/PEC.0000000000000511
- Lapierre C, Hugues N. Anomalous origin of the left coronary artery from the pulmonary artery (ALCAPA) in a newborn. Pediatric Radiology. 2010;40(SUPPL.1):77-77. doi:10.1007/s00247-009-1529-6
- Krishna MR. ALCAPA—A Reversible Cause of Dilated Cardiomyopathy in Infants. Indian Journal of Pediatrics. Published online April 27, 2021:1-1. doi:10.1007/s12098-021-03754-0
- Hoffman JIE. Electrocardiogram of anomalous left coronary artery from the pulmonary artery in infants. Pediatric Cardiology. 2013;34(3):489-491. doi:10.1007/s00246-012-0599-7
- Varghese M, Kothari S. The caveats in the diagnosis of anomalous origin of left coronary artery from pulmonary artery (ALCAPA). Images in paediatric cardiology. 2010;12(3):3-8. Accessed May 23, 2021. http://www.ncbi.nlm.nih.gov/pubmed/22368564




