
Author: Jamie Santistevan, MD (@jamie_rae_EMdoc – EM Physician, Presbyterian Hospital, Albuquerque, NM) // Edited by: Manpreet Singh, MD (@MPrizzleER – Assistant Professor of Emergency Medicine / Department of Emergency Medicine – Harbor-UCLA Medical Center) and Brit Long (@long_brit – EM Attending Physician, San Antonio, TX)
Welcome to this edition of ECG Pointers, an emDocs series designed to give you high yield tips about ECGs to keep your interpretation skills sharp. For a deeper dive on ECGs, we will include links to other great ECG FOAMed!
The Case:
A 65-year-old gentleman presents with stroke symptoms. His BP is 224/133. His initial ECG shows:

There is sinus rhythm with a rate of about 80. There is a right bundle branch block. There is a prolonged PR interval (280ms).
He receives IV labetalol for marked hypertension and his BP improves, but the nurse calls you to the bedside because his heart rate is now in the 40s. A second ECG shows:

There is bradycardia with QRS complexes clustered in groups of two. There is progressive lengthening of the PR interval followed by a prompt P-wave and an absent QRS. There are three P-waves for every two QRS complexes (3:2 conduction).
What are AV nodal blocks?
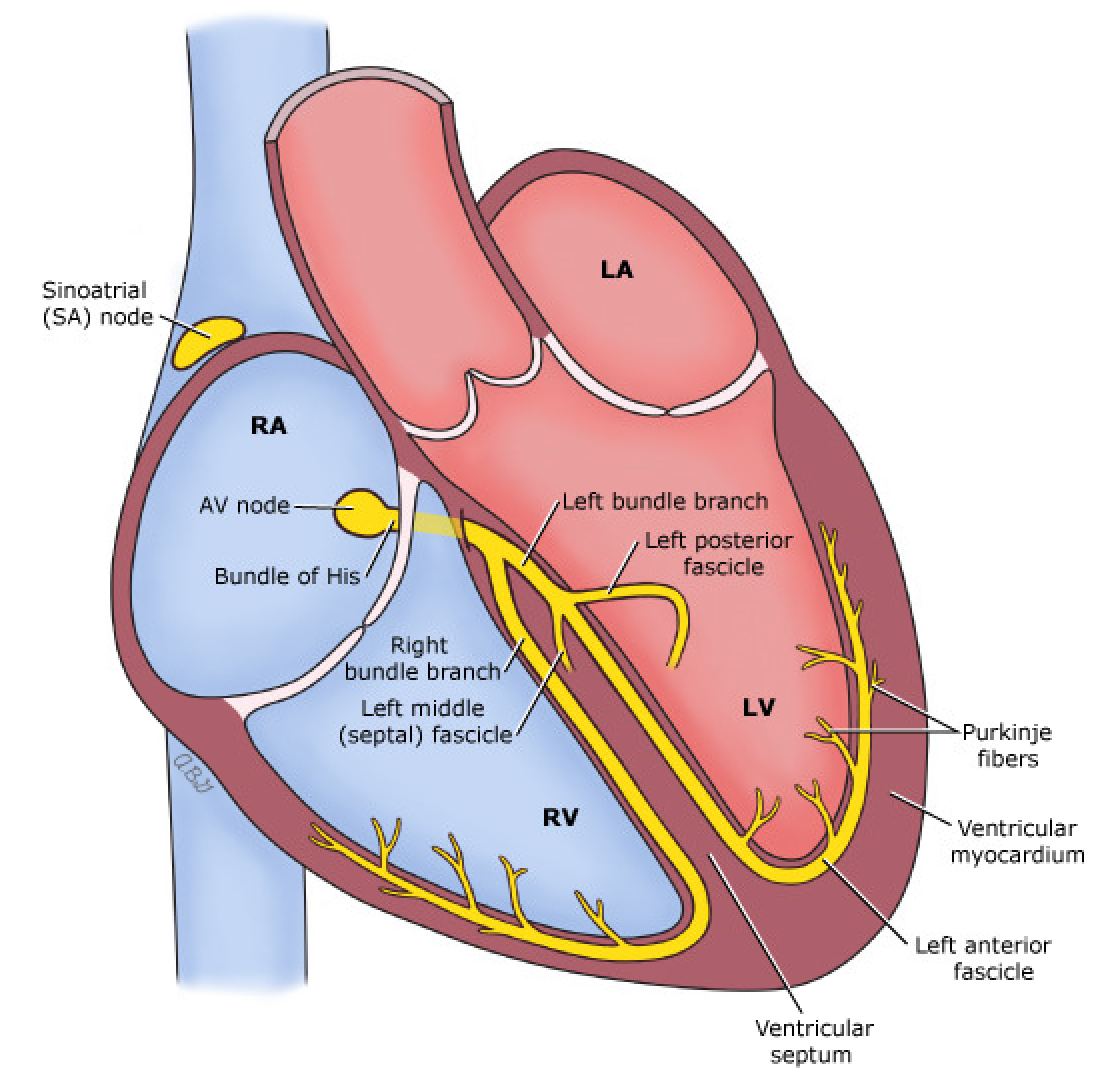
AV nodal blocks are defined as delay or interruption in transmission of the electrical impulse between the atria and ventricles. The conduction disturbance can be transient or permanent. They classified based on severity or degree of blockade —the more distal in the conduction system, the more severe block.
This post will focus on the so-called benign AV blocks. First-degree and second-degree Mobitz type I (Wenckebach) blocks are considered benign because they typically do not require external or permanent pacing [1].
First-degree AV block:
First-degree block is usually located within the AV node itself. The PR interval will be greater than 0.2 seconds (200 milliseconds) or one large box on the ECG paper. The PR interval is constant and there are no missed beats. A rare situation in which a pacemaker may be considered for first-degree AV block would include patients with neuromuscular disease (e.g. muscular dystrophy) due to the unpredictable risk of progression to higher degrees of AV blockade [2].
Severe first-degree AV block is a PR interval greater than 300ms. Check out this case from Life in the Fast Lane where the P-wave is buried within the preceding T-wave:

Second-degree Mobitz type I (Wenckebach):
Mobitz I block is due to a reversible conduction block within or just below AV node (i.e. the Bundle of His). Nodal cells progressively fatigue and eventually fail to conduct the impulse. This leads to a “dropped beat”—an absent QRS complex after a normal P-wave. Mobitz I rarely progresses to higher degree AV blockade. If patients are asymptomatic they do not require any specific treatment [1]. If they are symptomatic and unstable, they may respond to atropine. If atropine fails, they require pacing [2].
What to look for on the ECG:
- QRS complexes appear to be clustered in groups of 3-5 beats
- There are P-waves at the beginning and end of each cluster of beats
- P-waves are regular and the PR interval progressively lengthens
- The PR interval is the longest right before the dropped beat and the shortest right after the dropped beat
- The conduction of atrial beats to ventricular beats is usually in a pattern of 3:2, 4:3 or 5:4
Some causes of the benign AV blocks include:
- High vagal tone (e.g. young athlete, carotid massage, sleep)
- Cardiac surgery (e.g. aortic valve replacement)
- Cardiomyopathy (e.g. ischemic, hypertrophic obstructive and restrictive)
- Fibrosis or sclerosis of the conduction system
- Endocarditis and myocarditis (e.g. Lyme disease, systemic lupus erythematous, syphilis)
- Drugs: Beta blockers, calcium channel blockers, digoxin, amiodarone and other drugs that affect the sodium channel (e.g. quinidine, procainamide, disopyramide).
- Acute myocardial infarction
- Hyperkalemia
Patients with acute MI can develop AV block, with the likelihood and severity depending on the area and extent of the infarct [3]. In 90% of people, the AV nodal artery is supplied from the right coronary artery (RCA). An inferior wall myocardial infarction may precipitate AV block [4]. The finding of Mobitz type I in a patient with an inferior MI is associated with increased mortality, presumably due to larger infarct size. When AV block is due to acute MI, restoring perfusion frequently improves the AV block [5].
While asymptomatic patients do not require any specific therapy, reversible causes of AV block should be identified and treated. Patients having an acute MI need revascularization. When drugs are suspected, offending medications should be withheld or an antidote given. Hyperkalemia should be treated as usual: C BIG K DROP (Calcium, Beta-agonists/Bicarb, Insulin + Glucose, Kayexalate, Diuretics, Renal replacement) [6].
Top ECG pointers for the “benign” AV blocks
- First-degree AV block has a PR interval greater than one large box (200ms)
- Progressive lengthening of the PR interval is characteristic of second-degree Mobitz type I AV block (Wenckebach)
- First-degree and second-degree Mobitz I rarely require pacing
- Inferior MI, hyperkalemia and medication toxicity are some dangerous causes of AV blocks – the block itself might not need specific treatment, but you should identify and treat the underlying cause
But wait, here’s some more ECG FOAMed:
- Here is a great case of Wenckebach in a patient with RCA occlusion from Dr. Steve Smith: http://hqmeded-ecg.blogspot.com/search/label/wenckebach
- For a complete overview of conduction abnormalities, visit the ECG Learning Center: https://ecg.utah.edu/lesson/6
- A primer on heart block can be found at Taming the SRU at http://www.tamingthesru.com/blog/diagnostics/ecg-heart-blocks-primer
References:
- Epstein AE, DiMarco JP, Ellenbogen KA, et al. ACC/AHA/HRS 2008 Guidelines for Device-Based Therapy of Cardiac Rhythm Abnormalities: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the ACC/AHA/NASPE 2002 Guideline Update for Implantation of Cardiac Pacemakers and Antiarrhythmia Devices): developed in collaboration with the American Association for Thoracic Surgery and Society of Thoracic Surgeons. Circulation. 2008;117(21):e350.
- Sauer WH. Etiology of atrioventricular block. Nov 2017. Uptodate.com
- Zoob M and Smith KS. The aetiology of complete heart-block. Br Med J. 1963;2(5366):1149.
- Van der Hauwaert LG, Stroobandt R, Verhaeghe L. Arterial blood supply of the atrioventricular node and main bundle. Br Heart J. 1972 Oct;34(10):1045–51.
- Mullins CB, Atkins JM. Prognoses and management of ventricular conduction blocks in acute myocardial infarction. Mod Concepts Cardiovasc Dis. 1976;45(10):129.
- Xiong PY. Tiny Tip: C BIG K DROP (Management of Hyperkalemia with ECG changes). Sep 2014. Canadiem.org. https://canadiem.org/tiny-tip-hyperkalemia-management/





1 thought on “ECG Pointers: AV Blocks – Part I”
Pingback: emDOCs.net – Emergency Medicine EducationECG Pointers: AV blocks - Part II - emDOCs.net - Emergency Medicine Education