
Author: Lloyd Tannenbaum, MD (EM Attending Physician, APD, Geisinger Wyoming Valley, PA) and Jamie Kerestes, PharmD // Reviewer: Brit Long, MD (@long_brit)
Hello and welcome back to ECG Pointers, a series designed to make you more confident in your ECG interpretations. This week, we feature a post from Dr. Tannenbaum’s ECG Teaching Cases, a free ECG resource. Please check it out. Without further ado, let’s look at some ECGs!
“Hello residents! Welcome to your Cardiac Surgery ICU rotation. I’m Dr. Philippo, chief of cardiac anesthesia, and I’ll be your POC for this rotation. Before you start, we have a very important simulation to do. As you may have heard, we do things a little differently up here compared to the rest of the hospital.”
“What do you mean Dr. Philippo?” one of the residents asks.
“Great question. Let’s go over to the sim room and you’ll see. As we walk over, I’ll tell you the scenario,” he answers. “This is Becky, she’s 12 hours out from a coronary artery bypass grafting (CABG). There are drains and wires coming out of her chest. As the new resident on the floor, it’s your job to check on all the post op patients when you come on shift. I’ll step out and the sim will start. Good luck!”
“Wow, 4 residents all allowed to work together on a sim? That’s pretty great! This can’t be too hard, right?” One of the residents says out loud.
Dr. Philippo walks out and suddenly, the monitors that previously showed a blood pressure of 120/80 with a heart rate of 85 and a good pulse ox start alarming. Heart rate is very irregular and there’s a significant rhythm change. Blood pressure cuff starts to cycle but has not been able to find a pressure yet. This is what comes up on the monitor:
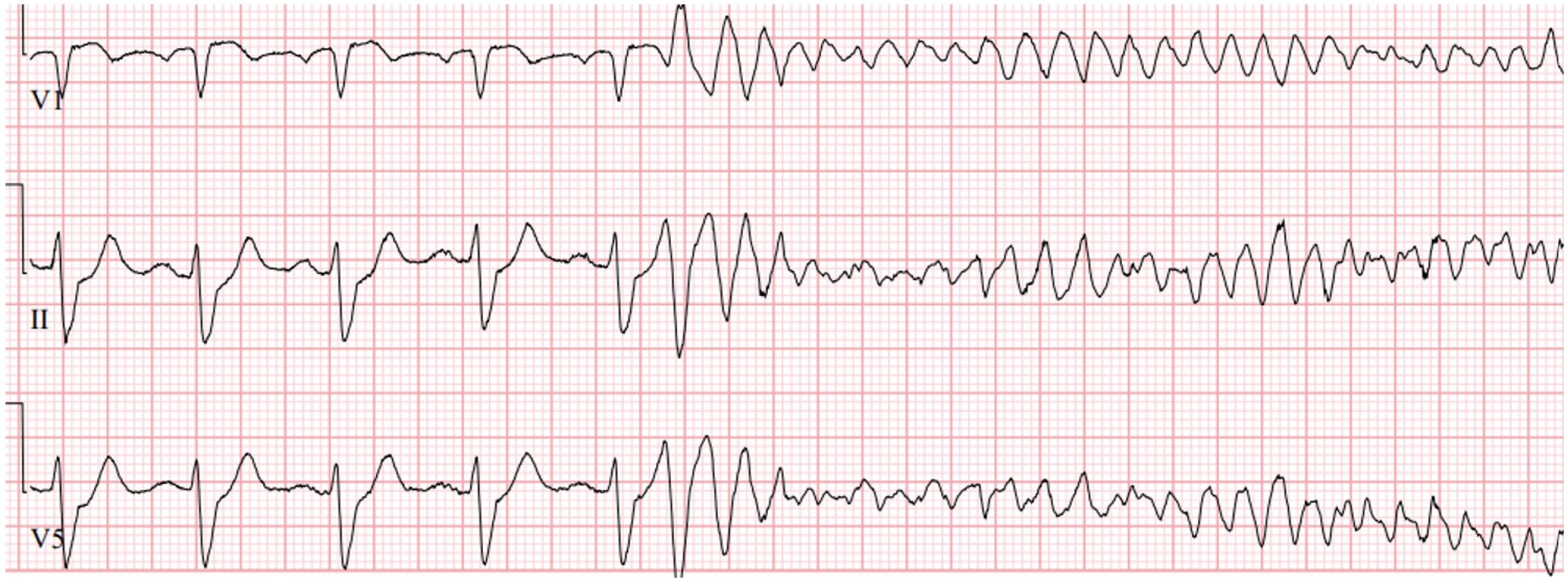
“She’s peri-arrest, about to code. Can anyone find a pulse?” The resident calls out.
“No pulse… We start CPR right? This is a code? We start compressions?”
“Wait, can we with a recently opened sternum?”
“She has no pulse! She’s in VF! We need to shock NOW… Where is the defibrillator!?!?!” And one of the residents starts to do compressions on the mannequin as the others scramble to find the defibrillator.
“AND STOP!” The residents hear Dr. Philippo yell. This is exactly why we do this sim on day one before you’re allowed to see any of my post-op patients with a recently opened chest. Let’s talk about changes to the standard ACLS algorithm that we do on post op patients, called Cardiac Advanced Life Support, or CALS. (NOTE: in the USA, CALS is also known as Cardiac Surgical Unit Advanced Life Support or CSU-ALS. For simplicity, in this write up, we’ll just be referring to it at CALS).
*****
CALS was first introduced as a guideline by Drs. Dunning et al in their landmark paper, “Guidelines for resuscitation in cardiac arrest after cardiac surgery” on the proper way to resuscitate a patient in cardiac arrest up to 10 days after open heart surgery.
Taken directly from their paper, they state:
“This protocol differs from existing generic guidelines in a number of areas, the most import of which are the following:
- Successful treatment of cardiac arrest after cardiac surgery is a multi-practitioner activity with six key roles that should be allocated and rehearsed on a regular basis.
- In ventricular fibrillation, three sequential attempts at defibrillation (where immediately available) should precede external cardiac massage.
- In asystole or extreme bradycardia, pacing (where immediately available) should precede external cardiac massage.
- Where the above measures fail, and in pulseless electrical activity, early resternotomy is advocated.
- Adrenaline [epinephrine] should not be routinely given.
- Protocols for excluding reversible airway and breathing complications and for safe emergency resternotomy are given.”
There are a couple of nuanced points to mention here. One of the most interesting ones is actually point 5, not giving adrenalin (epinephrine) to these patients if they arrest, so I’ll start there. This is mostly based on the data for giving epi in a code not being particularly strong and a letter to the editor by Dr. Webb describing a situation where 1 mg of epi was given in accordance with ACLS protocol when a post-op CABG patient arrested from a tension pneumothorax. Once a chest tube was placed, ROSC was rapidly achieved; however, a large amount of blood started coming out of his chest drains. When the patient had an emergent re-sternotomy, they found that the graft had burst open, likely secondary to the epi causing a huge spike in blood pressure. He encouraged the European Resuscitation Counsil to post cardiac surgery patients a special population and recommend against giving epi if they arrest.
Points 2, 3, and 4 change the way we’re supposed to approach these patients if they arrest. Ideally, we should spend 1 minute prepping to either shock, pace, or determine if the patient is in true PEA. Then, if necessary, start external CPR, recognizing that you may cause harm to the heart while compressing a split sternum, while the rest of the team preps to open the chest.
The major point that this paper makes and that the guidelines are based on, is that most causes of cardiac arrest in these patients are reversable and related to their cardiac surgery. Getting back into the chest as quickly as possible (emergent re-sternotomy) leads to better outcomes.
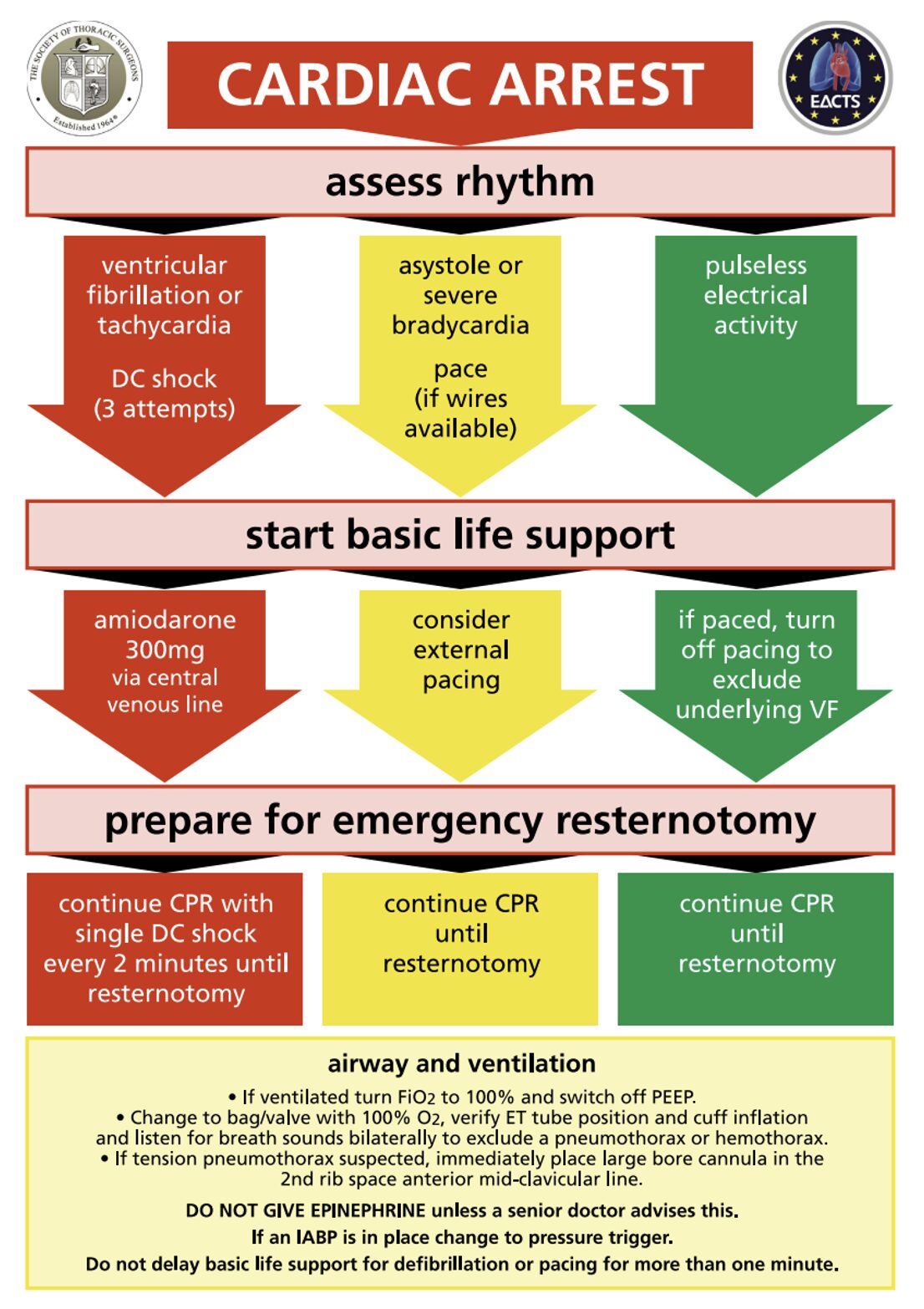
In 2017, the Society of Thoracic Surgeons wrote an Expert Consensus for the Resuscitation of Patients who Arrest After Cardiac Surgery that re-examined these guidelines. They built on the initial flowsheet provided by the first paper:
Cite: https://pubmed.ncbi.nlm.nih.gov/28122680/
If we take a look at the data here, first let’s start with early defibrillation (red arrow). Assuming you can get the machine set up to defibrillate under a minute, external CPR is not indicated before shocking 3 times back to back if the rhythm doesn’t convert (it’s harder than it sounds to get the machine and pads ready to go in 60 seconds). Why 3 shocks? Well, the authors pooled data from 15 papers and found that your chance of successfully cardioverting out of a dysrhythmia goes from 78% after the first shock to 35% after the second to 14% after the third. After 3 unsuccessful shocks, external CPR and emergent resternotomy is indicated as your chances of converting out of a dysrhythmia by defibrillating after 3 failed attempts is extremely low.
Now let’s briefly talk through the green and yellow arrows. If the patient is arresting and the rhythm isn’t amenable to defibrillation, consider pacing if the patient has severe bradycardia or asystole. From the paper:
“For asystole or severe bradycardia connect the epicardial pacing wires and set to DDD mode at 80 to 100 bpm at the maximum atrial and ventricular output voltage. If the pacing generator has an emergency pacing button, it may be used.
If the rhythm is pulseless electrical activity and a pacemaker is connected and functioning, then briefly turn off the pacemaker to exclude underlying ventricular fibrillation”
This paper also reexamined epi in the peri-arrest state and arrest state. If the senior physician decides to use epi, push-dose epinephrine, which is a lower concentration, (0.1mg/ml=100mcg/ml) is recommended. This is prepared by withdrawing 1 mL from the code epinephrine (1 mg/10 mL syringe) and diluting it with 9 mL of normal saline. The code leader will decide how much epi to give, but doses between 50 to 300 mcg are reasonable.
The paper also walks you through the steps of an emergency re-sternotomy, which can be found on page 1015.
Also, if you’re at one of these codes, remember that the patient will have lots of monitors and wires on them. So, consider using an arterial line or Swan-Ganz catheter to assist with pulse checks rather than relying on traditional, tactile checks.
Case wrap up:
“Ok guys, let’s run the sim again now that we’ve talked through CALS and have a better idea what to do,” Dr. Philippo says. “Control room, we’re going to do simulation 2, starting in 3.. 2.. 1! Good luck residents.”
Summary:
- Ventricular fibrillation: CALS recommends three rapid sequential defibrillation attempts (when immediately available) before initiating chest compressions. ACLS prioritizes immediate CPR with single-shock cycles.
- Asystole or severe bradycardia: CALS prioritizes immediate pacing (if available) before external cardiac massage. ACLS begins with CPR and medications rather than primary pacing.
- Refractory arrest / true Pulseless Electrical Activity: CALS advocates early resternotomy to address reversible surgical causes. ACLS relies on medical management and evaluation of H’s and T’s.
- Epinephrine: CALS does not recommend routine early epinephrine administration. When indicated, the standard ACLS code-dose concentration (1 mg/10 mL) should not be administered as a 1 mg bolus. Instead, push-dose epinephrine, which is a lower concentration, (0.1mg/ml=100mcg/ml) is recommended. This is prepared by withdrawing 1 mL from the code epinephrine (1 mg/10 mL syringe) and diluting it with 9 mL of normal saline. ACLS incorporates scheduled 1 mg (1 mg/10 mL) boluses as standard therapy every 3-5 minutes. The senior physician running the code should be the one deciding if epi should or should not be given.





