
Authors: Kyrra Engle, ScM (@KyrraEngle, University of Miami Miller School of Medicine); Alessandra Della Porta (@MedEdtweeter, University of Miami Miller School of Medicine); Zoe Kornberg, MD, MPH (Department of Obstetrics and Gynecology, University of Texas Rio Grande Valley); Kasha Bornstein (@BornsteinKasha) // Reviewed by: Marina Boushra, MD; Alex Koyfman, MD (@EMHighAK); Brit Long, MD (@long_brit)
Case
A 27-year-old P3G3 woman is found by her partner seizing at home one-week post-partum from a preterm (31 weeks + 4 days) pregnancy complicated by gestational hypertension. She was unable to schedule obstetric appointments during her second trimester due to loss of her insurance. She had been complaining of a headache earlier in the day, worsening prior to the seizure. On arrival to the patient’s home, paramedics find her altered, weak, and incontinent of urine. Pre-hospital vital signs included a heart rate of 110 bpm and a blood pressure of 180/110 mmHg. En route to the emergency department (ED), paramedics witnessed a second generalized seizure, started an IV, and administered midazolam. She continued to seize, requiring a repeat dose of midazolam. As she is transferred from the stretcher to a hospital bed, she has a third seizure with tonic/clonic activity.
Introduction
Pregnancy-related conditions are the sixth most common reason for presentation to the ED in female patients of childbearing age, and account for 1.3% of ED visits overall.1,2 Furthermore, of the four million patients that give birth in the United States each year, approximately 5% will present to the ED in the 6 weeks following delivery, highlighting the importance of emergency providers’ ability to recognize and acutely manage obstetric complications.3,4
The most common neurologic complication of pregnancy is seizures, with a prevalence of 1.2% in the United States.5,6Although epilepsy is the most common cause of seizures in gravid patients, eclampsia remains a major cause of gestational morbidity and mortality due to the risk of hypoxic-ischemic brain injury and seizure-related intracranial hemorrhage 5,7-9 Eclampsia is among the top six causes of maternal death in the United States following postpartum hemorrhage, infection, and cardiovascular conditions.10,11 Emergency providers can play a key role in recognizing and acutely managing patients with eclampsia, especially those who may not be able to access prenatal care or those who present in the postpartum period.
Definition
Eclampsia is defined as the occurrence of one or more generalized tonic-clonic convulsions unrelated to other medical conditions in pregnant or postpartum patients with hypertensive disorders of pregnancy.8-10 Hypertensive disorders of pregnancy are a spectrum of clinical conditions including chronic hypertension, gestational hypertension, preeclampsia, preeclampsia superimposed on chronic hypertension, and Hemolysis, Elevated liver enzymes and Low platelets (HELLP) syndrome.12,13 Defining characteristics of the hypertensive disorders of pregnancy can be observed in Table 1. As convulsions may be the presenting symptom of preeclampsia, seizures in pregnant or postpartum patients should be considered eclampsia until proven otherwise.14

Epidemiology
In the United States, eclampsia occurs in approximately 0.3% of live births with significant variation in incidence between states.15 This variation is likely due to differences in screening and the use of magnesium sulfate, economic inequity, quality and access to obstetric care, and the distribution of physical factors associated with eclampsia.15Socioeconomic status has been found to play an important role in the incidence of eclampsia with the presence of public insurance and fewer than five prenatal visits significantly increasing the risk of eclampsia.16 Other factors associated with eclampsia are similar to those for preeclampsia, and include, extremes of maternal age, nulliparity, multiple gestations, obesity, diabetes, and preterm delivery at <32 weeks of gestation.10,16-18 Eclampsia is also more common among women who self-identify as Black or Hispanic for reasons that are multifactorial and likely related to social determinants of health, including access to prenatal care and chronic stress associated with experiences of racial discrimination. 16,17,19,20
Maternal Fetal Outcomes
In the acute setting, complications associated with highest morbidity include stroke, coma or persistent loss of consciousness, heart failure, pulmonary edema, venous thrombosis, and disseminated intravascular coagulation. Pregnant patients with a history of eclampsia have a 25% risk of developing eclampsia in subsequent pregnancies and long term sequelae, including a 12-fold risk of cardiovascular-related pathologies, such as myocardial infarction, cerebrovascular disease and heart failure.21 Neonates born to patients with eclampsia are at increased risk of being small for gestational age due to intrauterine growth restriction and complications associated with premature birth, including neonatal respiratory distress syndrome.10,22,23
Time of Onset
Eclampsia can present during the antepartum, intrapartum, or postpartum period.24-26 In the postpartum period, the onset of convulsions may occur within the first 48 hours (early postpartum) or up to six weeks following delivery (late postpartum).24,27 Among eclampsia cases, 59-70% of occur during the antepartum period, around 20- 30% occur during labor (intrapartum), and 20- 30% occur in the postpartum period, including 15- 16% in the late postpartum period.10,26,28,29 In the antepartum period, virtually all eclamptic seizures occur after 28 weeks of gestation. When seen before 20 weeks of gestation, eclampsia is usually associated with a molar pregnancy, multiple gestations, or severe maternal renal disease.5,10,30,31
Presentation
More than 50% of eclamptic seizures are preceded by prodromal symptoms.14,26,32 The most common reported symptoms are headache (66-82%), visual disturbances (27-44%), and epigastric pain (25%).14,29,33 Visual disturbances include blurry vision, diplopia, scotoma, photopsia, and transient cortical blindness.10,34,35 However, none of these symptoms have been found to accurately predict, or rule out, imminent eclampsia.8,14,29,36 Additionally, if the patient is unresponsive and records or family members are unavailable, it may not be possible to evaluate for these prodromal symptoms.5 For this reason, many clinicians rely on exam findings and laboratory evidence of eclampsia including hypertension and proteinuria.
While hypertension has long been recognized as a manifestation of preeclampsia and a warning sign for eclampsia, the degree of hypertension may not always predict the risk of eclampsia.30 Approximately 20% of eclampsia cases occur in patients with only mild hypertension. Furthermore, hypertension may be absent in up to 25% of cases.8-10,29 Severe hypertension is more common in pregnant patients who developed eclampsia in the antepartum period rather than the postpartum period.26
Differential Diagnosis
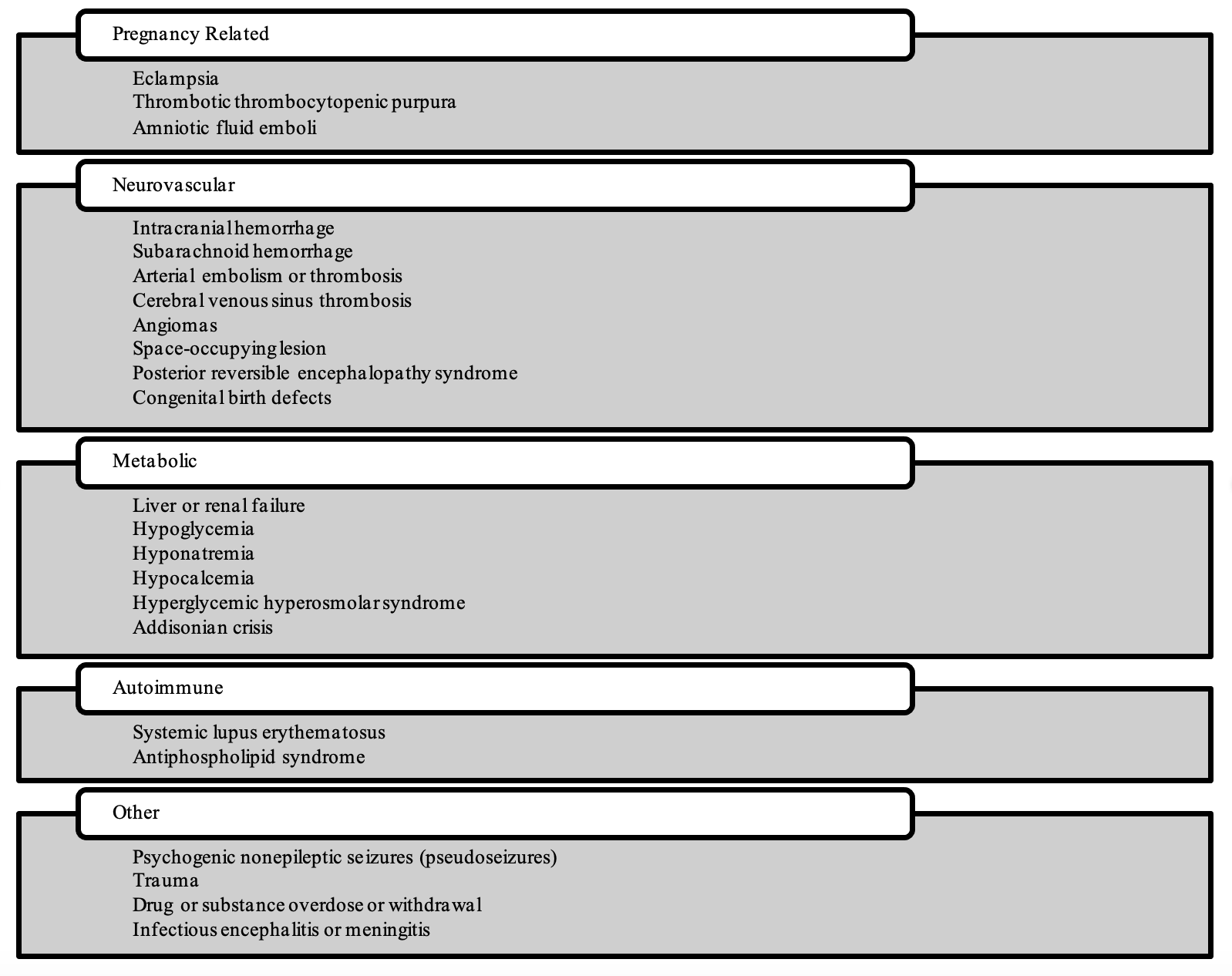
While the evaluation of seizure in pregnant or postpartum patients should begin with a consideration of eclampsia, alternative diagnoses should also be considered in certain circumstances.10 These circumstances include patients with normal blood pressure and the absence of proteinuria, focal neurologic deficits, onset before 20 weeks of gestation or >48 hours after delivery, or prolonged loss of consciousness.10,37 In these cases, the differential diagnosis can generally be broken down into three categories of conditions: exacerbation of known pre-existing seizure disorder (mainly epilepsy), new onset of seizures due to non-pregnancy related problem (eg, metabolic alterations, brain tumors, infections), and neurologic conditions either specific to or frequently occurring during pregnancy.14,38-40 A complete differential diagnosis of seizures that should be taken into consideration is listed in Figure 1.5,7,10,14
Figure 1: Differential Diagnosis of Seizure During Pregnancy or After Delivery.5,10
History and Physical Exam
A thorough history and physical examination are key to narrowing the differential diagnosis. Seizure activity in a pregnant or postpartum patient without a history of epilepsy should be considered eclampsia until proven otherwise.5 In 78-83% of eclampsia cases, the seizures are preceded by signs of cerebral irritation, such as persistent headaches, blurred vision, photophobia, or altered mental status.12 As eclamptic seizures are typically tonic-clonic in nature and often last less than one minute, obtaining as much history of the event, including any symptoms prior to the onset of seizure activity, length of time and bodily location of convulsions, and presence of post-ictal state can be useful in ruling out potential etiologies.26,32 A full history may be difficult to obtain from the patient if there are alterations in mental status. However, when possible, information regarding the pregnancy, including gestational age, complications, mode of delivery if postpartum and maternal history should be obtained.
While all patients presenting with seizure—especially new onset—should have a full neurological examination in the ED, physical examination following eclamptic seizure may be unremarkable, apart from hypertension or residual confusion. Clonus or hyperreflexia may be found on focused neurology exam.35,41 Patients who go on to develop eclamptic seizures often present with symptoms of headache, visual disturbance, or altered mental status. Neuroimaging is not recommended in the routine care or diagnosis of patients with eclampsia. However, in patients with atypical presentations, including recurrent convulsions, prolonged coma or focal neurologic deficits, neuroimaging may be warranted to rule out cerebral edema, infarction, and hemorrhage, which would require additional pharmacologic or surgical intervention.10,41,42
Recognizing the manifestations of eclampsia is particularly important as eclampsia is one of the most preventable causes of gestational mortality, which occurs secondary to high rates of diagnostic delay, ineffective control of blood pressure, and lack of continuity of care.43 A recent study among Ob/Gyn residents found that while all learners were familiar with the management of pre-eclampsia and emergent hypertension, none were able to stop an eclamptic seizure in a case-based simulation.44 Furthermore, all participants indicated they had no exposure to patients with eclampsia and found the simulation immensely valuable, suggesting a gap in resident medical education and that exposure may contribute to the preventable deaths associated with eclampsia.
Management
As with all patients who arrive at the emergency department with active seizure-like movements, initial consideration for respiratory and circulatory status should take precedence. Any concern for patency of the airway should be addressed immediately and obstruction with secretions should be addressed with suctioning of the oropharynx following cessation of seizure activity.5 Oxygenation and prevention of hypoxia for both patient and fetus should be addressed with supplemental oxygen as appropriate. Additionally, maternal repositioning to the left lateral decubitus position can increase placental blood flow and reduce risk of aspiration.45
In gravid or peripartum patients who present with seizure or concern for eclampsia, OB/GYN consult should be obtained early in emergency department evaluation. Following stabilization, patients should be admitted or transferred to a tertiary medical center with OB/GYN service for continuous monitoring, assurance of fetal wellbeing, and delivery planning ifprepartum.10
Seizure activity
The mainstay of treatment for eclampsia is magnesium sulfate, both as seizure prophylaxis in patients with preeclampsia and as a first line antiepileptic when seizures occur.44,46-49 A 2010 Cochrane review evaluating the evidence supporting magnesium sulfate vs. diazepam in the treatment of eclampsia demonstrated fewer maternal deaths and recurrence of seizures in patients receiving magnesium. There was no difference in neonatal outcomes.50 The largest trials included in this review demonstrated a 52% lower risk of recurrent convulsions in patients receiving magnesium sulfate when compared with diazepam and a 67% lower risk when compared with phenytoin.51 The American College of Obstetrics and Gynecology (ACOG) currently maintains a level A recommendation for the use of magnesium sulfate in the prevention and treatment of eclampsia. A summary of the following recommendations can be seen in Table 2.
Mechanistically, magnesium has many sites of action, but exerts its main therapeutic effect by stabilizing cell membrane potentials and inducing smooth muscle relaxation.52 Therapeutic plasma levels of magnesium necessary to reduce and prevent seizures (3.5-7mEq/L) are much greater than those used in treatment of other conditions.53 The most recent ACOG guidelines recommend initial dosing in any patient suspected to have eclampsia includes a loading dose of 4 or 6 grams over 15-20 minutes, followed by maintenance with continuous infusion at a rate of 2 g/hr.10 If IV magnesium sulfate is not available or IV access cannot be established, administer a 10g loading dose IM (5g IM in each buttock) followed by 5g IM every 4 hours.
There are few absolute contraindications to magnesium sulfate therapy, including myasthenia gravis, severe hypocalcemia, complete heart block, and myocarditis.12 Renal failure is a relative contraindication. Magnesium is fully excreted by the kidneys and therefore dosing should be adjusted in patients with potential for reduced clearance.44Patients with serum creatinine > 1.2mg/dL should receive a standard loading dose of 4 to 6 grams, but a maintenance infusion at a lower rate of 1g/hr.54 Caution is advised in patients taking labetalol and nifedipine; administration of magnesium sulfate may produce a synergistic effect leading to bradycardia and/or hypotension.55 Monitoring of magnesium levels is not universally recommended, except in patients with renal dysfunction or those showing signs of toxicity, such as loss of deep tendon reflexes, respiratory depression, or cardiac arrest.10 Attention should be taken to limit total IV fluid administration to an average of <125 mL/hr to avoid pulmonary edema, a common complication of severe preeclampsia.56
Despite proper dosing and monitoring, approximately 10% of eclamptic patients will have recurrence of seizure activity following administration of magnesium sulfate.55 Return of convulsions should be addressed with a second 2g bolus of magnesium sulfate given over a course of 3 to 5 minutes. While rare, seizures resistant to magnesium sulfate, or with recurrence following a second magnesium bolus, treatment with benzodiazepines can be considered, with recent reviews recommending dosing 4 mg lorazepam over 3 to 5 minutes.10 In cases where magnesium sulfate is unavailable, or there is a significant delay in preparation, patients may be initiated on benzodiazepine therapy with intravenous diazepam at a rate of 2mg/min with a maximum of 10mg, or clonazepam 1-2mg over 2-5 minutes.57 In patients of childbearing age with recurrent seizure activity and unknown history of recent or current pregnancy, magnesium sulfate therapy should be considered, especially if seizures are refractory to typical therapy.

Hypertension
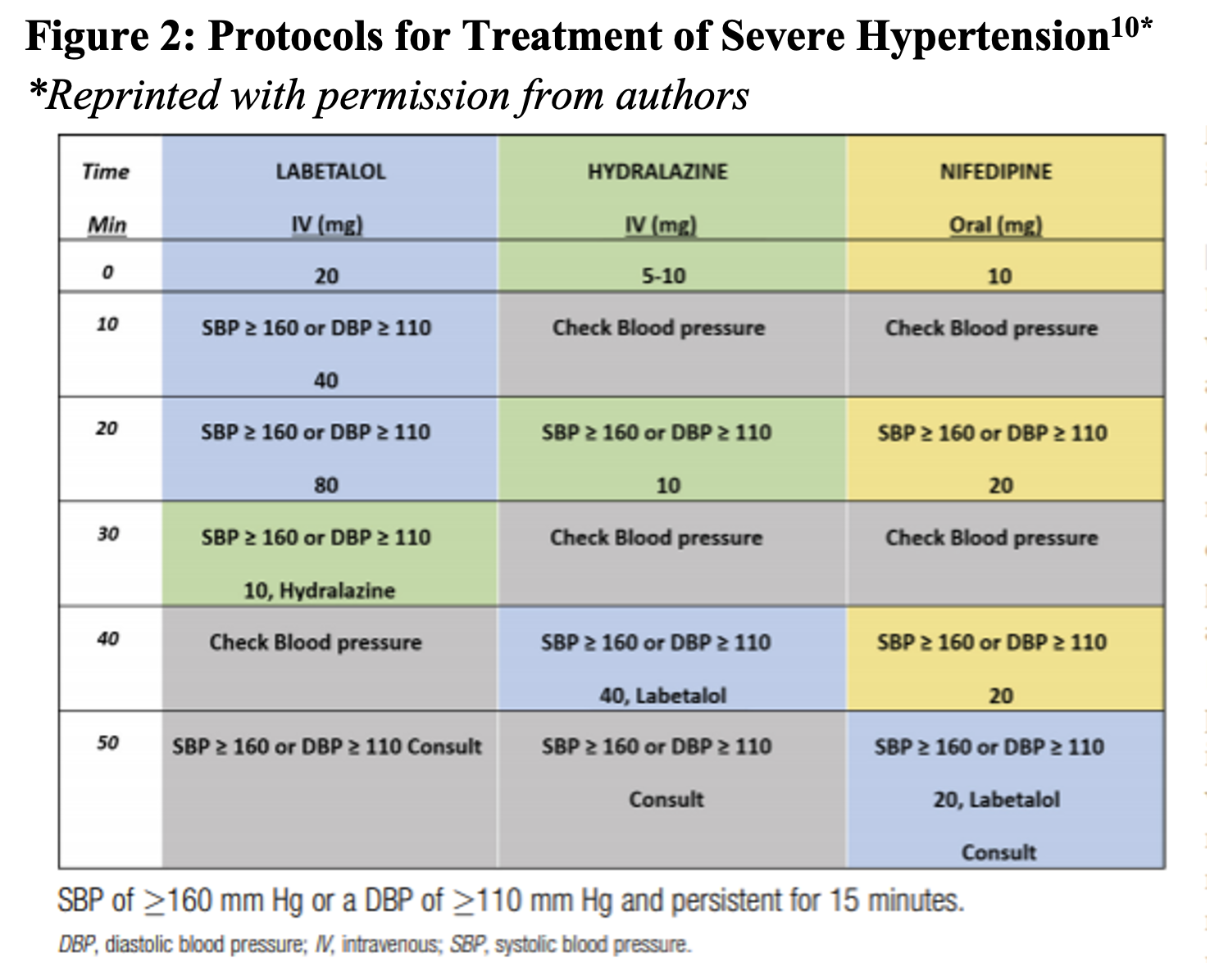
Severe range hypertension in pregnancy is defined as systolic blood pressures >160 mmHg and/or diastolic blood pressures >110 mmHg.10,58 This is the range at which the likelihood of the patient developing eclampsia, stroke, and/or vasogenic edema, rises precipitously.46 Note that these threshold values for hypertensive emergency in pregnancy are much lower than the blood pressure ranges considered to be emergent in non-pregnant adults. Prior research has demonstrated that increased cerebral perfusion and vasogenic edema secondary to hypertension can independently produce seizure activity, thus, increasing the importance of maintaining blood pressures below the severe range.59
While definitive management of severe hypertension from preeclampsia is delivery of the fetus and placenta, temporizing antihypertensive medications should be administered as soon as possible.58 Anti-hypertensive agents other than labetalol, hydralazine, and nifedipine (immediate release formulation) have either not been tested in pregnant populations or are associated with fetal toxicity and should be avoided whenever possible. Immediately following administration, blood pressures should be reassessed at 10-minute intervals, with additional dosing as described in Figure 2.
Takeaways
- Eclampsia is among the top six causes of maternal death in the United States
- Eclampsia should be in the differential in any female or antepartum or postpartum patient presenting with altered mental status, persistent headache, visual changes, or convulsive symptoms.
- The immediate management of eclampsia for both seizure treatment and prophylaxis is IV magnesium sulfate.
- Hypertension of greater than or equal to 160/110 in the pregnant patient is an emergency and should be managed with immediate administration of antihypertensive medications safe for use in pregnancy.
From Dr. Katy Hanson at Hanson’s Anatomy:

References/Further Reading:
- Rui P KK, Albert M. National Hospital Ambulatory Medical Care Survey: 2013 Emergency Department Summary Tables. Available at: http://www.cdc.gov/nchs/data/ahcd/nhamcs_emergency/2013_ed_web_tables.pdf.
- Robinson DW, Anana M, Edens MA, et al. Training in Emergency Obstetrics: A Needs Assessment of U.S. Emergency Medicine Program Directors. West J Emerg Med. 2018;19(1):87-92.
- Sheen JJ, Smith HA, Tu B, Liu Y, Sutton D, Bernstein PS. Risk Factors for Postpartum Emergency Department Visits in an Urban Population. Matern Child Health J. 2019;23(4):557-566.
- Clark SL, Belfort MA, Dildy GA, et al. Emergency department use during the postpartum period: implications for current management of the puerperium. Am J Obstet Gynecol. 2010;203(1):38 e31-36.
- Bollig KJ, Jackson DL. Seizures in Pregnancy. Obstet Gynecol Clin North Am. 2018;45(2):349-367.
- Zack MM, Kobau R. National and State Estimates of the Numbers of Adults and Children with Active Epilepsy – United States, 2015. MMWR Morb Mortal Wkly Rep. 2017;66(31):821-825.
- Hart LA, Sibai BM. Seizures in pregnancy: epilepsy, eclampsia, and stroke. Semin Perinatol. 2013;37(4):207-224.
- Hastie R, Brownfoot FC, Cluver CA, et al. Predictive Value of the Signs and Symptoms Preceding Eclampsia: A Systematic Review. Obstet Gynecol. 2019;134(4):677-684.
- Sibai BM. Diagnosis, prevention, and management of eclampsia. Obstet Gynecol. 2005;105(2):402-410.
- Fishel Bartal M, Sibai BM. Eclampsia in the 21st century. Am J Obstet Gynecol. 2020.
- Davis NL SA, Goodman DA. Pregnancy-related deaths: data from 14 US maternal mortality review committees, 2008-2017. https://www.cdc.gov/reproductivehealth/maternal-mortality/erase-mm/mmr-data-brief.html. Updated September 4, 2019. Accessed January 8, 2021, 2021.
- Gestational Hypertension and Preeclampsia: ACOG Practice Bulletin, Number 222. Obstet Gynecol. 2020;135(6):e237-e260.
- American College of O, Gynecologists’ Committee on Practice B-O. ACOG Practice Bulletin No. 203: Chronic Hypertension in Pregnancy. Obstet Gynecol. 2019;133(1):e26-e50.
- Aya AG, Ondze B, Ripart J, Cuvillon P. Seizures in the peripartum period: Epidemiology, diagnosis and management. Anaesth Crit Care Pain Med. 2016;35 Suppl 1:S13-S21.
- Butwick AJ, Druzin ML, Shaw GM, Guo N. Evaluation of US State-Level Variation in Hypertensive Disorders of Pregnancy. JAMA Netw Open. 2020;3(10):e2018741.
- Esakoff TF, Rad S, Burwick RM, Caughey AB. Predictors of eclampsia in California. J Matern Fetal Neonatal Med. 2016;29(10):1531-1535.
- Liu S, Joseph KS, Liston RM, et al. Incidence, risk factors, and associated complications of eclampsia. Obstet Gynecol. 2011;118(5):987-994.
- Sibai BM, Hauth J, Caritis S, et al. Hypertensive disorders in twin versus singleton gestations. National Institute of Child Health and Human Development Network of Maternal-Fetal Medicine Units. Am J Obstet Gynecol. 2000;182(4):938-942.
- Grobman WA, Parker CB, Willinger M, et al. Racial Disparities in Adverse Pregnancy Outcomes and Psychosocial Stress. Obstet Gynecol. 2018;131(2):328-335.
- Johnson JD, Louis JM. Does race or ethnicity play a role in the origin, pathophysiology, and outcomes of preeclampsia? An expert review of the literature. Am J Obstet Gynecol. 2020.
- Ackerman CM, Platner MH, Spatz ES, et al. Severe cardiovascular morbidity in women with hypertensive diseases during delivery hospitalization. Am J Obstet Gynecol. 2019;220(6):582 e581-582 e511.
- Hypertension in Pregnancy: Executive Summary. Obstetrics & Gynecology. 2013;122(5):1122-1131.
- Emergent Therapy for Acute-Onset, Severe Hypertension During Pregnancy and the Postpartum Period: COMMITTEE OPINION SUMMARY, Number 692. Obstetrics & Gynecology. 2017;129(4):769-770.
- Chames MC, Livingston JC, Ivester TS, Barton JR, Sibai BM. Late postpartum eclampsia: a preventable disease? Am J Obstet Gynecol. 2002;186(6):1174-1177.
- Lopez-Llera M. Main clinical types and subtypes of eclampsia. Am J Obstet Gynecol. 1992;166(1 Pt 1):4-9.
- Mattar F, Sibai BM. EclampsiaVIII. Risk factors for maternal morbidity. American Journal of Obstetrics and Gynecology. 2000;182(2):307-312.
- Lubarsky SL, Barton JR, Friedman SA, Nasreddine S, Ramadan MK, Sibai BM. Late postpartum eclampsia revisited. Obstet Gynecol. 1994;83(4):502-505.
- Cooray SD, Edmonds SM, Tong S, Samarasekera SP, Whitehead CL. Characterization of symptoms immediately preceding eclampsia. Obstet Gynecol. 2011;118(5):995-999.
- Berhan Y, Berhan A. Should magnesium sulfate be administered to women with mild pre-eclampsia? A systematic review of published reports on eclampsia. J Obstet Gynaecol Res. 2015;41(6):831-842.
- Sibai BM, Stella CL. Diagnosis and management of atypical preeclampsia-eclampsia. Am J Obstet Gynecol. 2009;200(5):481 e481-487.
- Hazra S, Waugh J, Bosio P. ‘Pure’ pre-eclampsia before 20 weeks of gestation: a unique entity. BJOG. 2003;110(11):1034-1035.
- Douglas KA, Redman CW. Eclampsia in the United Kingdom. BMJ. 1994;309(6966):1395-1400.
- Watson DL, Sibai BM, Shaver DC, Dacus JV, Anderson GD. Late postpartum eclampsia: an update. South Med J. 1983;76(12):1487-1489.
- Roos NM, Wiegman MJ, Jansonius NM, Zeeman GG. Visual disturbances in (pre)eclampsia. Obstet Gynecol Surv. 2012;67(4):242-250.
- Shah AK, Rajamani K, Whitty JE. Eclampsia: A neurological perspective. Journal of the Neurological Sciences. 2008;271(1):158-167.
- Martin JN, Jr., Rinehart BK, May WL, Magann EF, Terrone DA, Blake PG. The spectrum of severe preeclampsia: comparative analysis by HELLP (hemolysis, elevated liver enzyme levels, and low platelet count) syndrome classification. Am J Obstet Gynecol. 1999;180(6 Pt 1):1373-1384.
- Morton A. Imitators of preeclampsia: A review. Pregnancy Hypertens. 2016;6(1):1-9.
- Pollock W, Rose L, Dennis CL. Pregnant and postpartum admissions to the intensive care unit: a systematic review. Intensive Care Med. 2010;36(9):1465-1474.
- Harrison DA, D’Amico G, Singer M. Case mix, outcome, and activity for admissions to UK critical care units with severe acute pancreatitis: a secondary analysis of the ICNARC Case Mix Programme Database. Crit Care. 2007;11 Suppl 1:S1.
- Zwart JJ, Richters JM, Ory F, de Vries JI, Bloemenkamp KW, van Roosmalen J. Severe maternal morbidity during pregnancy, delivery and puerperium in the Netherlands: a nationwide population-based study of 371,000 pregnancies. BJOG. 2008;115(7):842-850.
- Moeller JJ, Hirsch LJ. Diagnosis and classification of seizures and epilepsy. In: Winn RH, editor. Youmans and Winn neurological Surgery. 7th edition. Philadelphia: Elsevier; 2017. p. 388–95.
- Hecht JL, Ordi J, Carrilho C, et al. The pathology of eclampsia: An autopsy series. Hypertens Pregnancy. 2017;36(3):259-268.
- Main EK, McCain CL, Morton CH, Holtby S, Lawton ES. Pregnancy-related mortality in California: causes, characteristics, and improvement opportunities. Obstet Gynecol. 2015;125(4):938-947.
- Abraham C, Kusheleva N. Management of pre-eclampsia and eclampsia: a simulation. MedEdPORTAL. 2019;15:10832. https://doi.org/10.15766/mep_2374-8265.10832.
- Gerard EE, Samuels P. Neurologic disorders in pregnancy. In: Gabbe SG, editor. Obstetrics: normal and problem pregnancies. 7th edition. Philadelphia: Elsevier; 2017. p. 1030–56.
- Garg D, Rahaman B, Stein EG, Dickman E. Late Postpartum Eclampsia with Postpartum Angiopathy: An Uncommon Diagnosis in the Emergency Department. J Emerg Med. 2015;49(6):e187-191.
- Sibai BM. Magnesium sulfate prophylaxis in preeclampsia: Lessons learned from recent trials. Am J Obstet Gynecol. 2004;190(6):1520-1526.
- Eclampsia checklist. In ACOG safe motherhood initiative. 2017. Available at: https://www.acog.org/-/media/Districts/District-II/Public/SMI/v2/sm02a170713EclampsiaCheckRev072017.pdf?dmc51&ts520170928T0147570258. Accessed January 18, 2021.
- Lucas MJ, Leveno KJ, Cunningham FG. A comparison of magnesium sulfate with phenytoin for the prevention of eclampsia. N Engl J Med. 1995;333(4):201-205.
- Duley L, Henderson-Smart DJ, Walker GJ, Chou D. Magnesium sulphate versus diazepam for eclampsia. Cochrane Database Syst Rev. 2010(12):CD000127.
- The Eclampsia Trial Collaborative G. Which anticonvulsant for women with eclampsia? Evidence from the Collaborative Eclampsia Trial. The Lancet. 1995;345(8963):1455-1463.
- Tso E, Reid RP, Barish RA, Browne BJ. Late postpartum eclampsia. Ann Emerg Med. 1987;16(8):907-909.
- Euser AG, Cipolla MJ. Magnesium sulfate for the treatment of eclampsia: a brief review. Stroke. 2009;40(4):1169-1175.
- Alexander JM, McIntire DD, Leveno KJ, Cunningham FG. Selective magnesium sulfate prophylaxis for the prevention of eclampsia in women with gestational hypertension. Obstet Gynecol. 2006;108(4):826-832.
- Gilardi E, Marsiliani D, Nicolo R, et al. Magnesium sulphate in the Emergency Department: an old, new friend. Eur Rev Med Pharmacol Sci. 2019;23(9):4052-4063.
- Anthony J, Schoeman LK. Fluid management in pre-eclampsia. Obstet Med. 2013;6(3):100-104.
- Lowe SA, Bowyer L, Lust K, et al. SOMANZ guidelines for the management of hypertensive disorders of pregnancy 2014. Aust N Z J Obstet Gynaecol. 2015;55(5):e1-29.
- Kattah AG, Garovic VD. The management of hypertension in pregnancy. Adv Chronic Kidney Dis. 2013;20(3):229-239.
- Zeeman GG, Hatab M, Twickler DM. Maternal cerebral blood flow changes in pregnancy. Am J Obstet Gynecol. 2003;189(4):968-972.





1 thought on “Eclampsia in the ED: Presentation, Differential Diagnosis, and Treatment”
Pingback: Conference Recap 11/29/23 – BMC EM Blog