Authors: Corey Hazekamp, MD (@coreyhazekamp, EM Resident Physician, Lincoln Emergency Medicine) and Tony Spadaro, MD (EM Resident Physician, University of Pennsylvania Emergency Medicine) // Reviewed by: Alex Koyfman, MD (@EMHighAK); Brit Long, MD (@long_brit); and Marina Boushra, MD
Case
A 46-year-old patient is evaluated in the Emergency Department (ED) for vomiting. The patient is anxiously rocking back and forth on the stretcher and has an emesis basin filled with non-bloody, non-bilious vomit. The patient states that they are addicted to heroin and are withdrawing. The patient reports they feel anxious and have muscle aches everywhere. The patient’s clothes and shoes appear to be soiled and torn. When asked about their history of using medications for opioid use disorder, the patient reports they have tried methadone intermittently, but it has been over a year since they last used methadone. They have never tried buprenorphine. The patient admits to daily injection of heroin, denies daily consumption of alcohol because “they cannot afford it,” and denies use of any other illicit substances. When asked where the patient resides, they just respond ‘wherever I can find a place to sleep.” After further discussion, the patient states they are interested in trying buprenorphine as a medication for opioid use disorder.
Significance
The United States has recently experienced an unprecedented increase in opioid overdose deaths.1 While the total number of ED visits for other medical emergencies decreased during the COVID-19 pandemic, the number of opioid overdose-related visits increased.2,3 Medications for opioid use disorder (MOUD) have been shown to reduce morbidity and mortality for patients with opioid use disorder (OUD). However, most patients with OUD do not receive these life-saving treatments.3–5 Furthermore, disparities in access to MOUD remain. For example, access to buprenorphine after discharge from an ED depends on the provider offering buprenorphine treatment and the patient having access to a physical location that offers buprenorphine. Research has shown that communities primarily composed of non-Hispanic Black or Hispanic residents are more likely to have access to methadone clinics and less likely to have access to buprenorphine providers.6 Kilaru et al. provided evidence suggesting that for patients who presented to the ED with a non-fatal opioid overdose, Black patients were approximately half as likely as non-Hispanic White patients to receive follow-up treatment for OUD.7 Similarly, women and Hispanic patients were less likely to receive follow-up for OUD treatment.7 More recently, Stevens et al. found that non-Hispanic Black patients and Hispanic patients had lower rates of filling buprenorphine prescriptions compared to non-Hispanic White patients when being prescribed buprenorphine from the ED.8 They also found that patients with socioeconomic advantages – being male, younger in age, and non-Hispanic White – were more likely to successfully receive buprenorphine as a treatment for OUD from EDs.8 These findings highlight that there are major disparities in accessing this life-saving medication and follow-up treatment, in addition to disparities in patients being offered buprenorphine.
Emergency Medicine will inevitably play a crucial role in the battle against the opioid epidemic currently ravaging the United States. Current and future emergency physicians will play a pivotal role in this effort. Accordingly, education on the effective treatment of OUD is essential. However, there are complexities involved in properly treating OUD from the ED. Physicians’ experiences in treating OUD are widely variable as there are no uniform protocols for initiating buprenorphine in the ED. The arrangement of follow-up treatment is also very different regionally. This article will review the basics of ED-initiated buprenorphine and summarize currently available resources for emergency physicians to learn how to properly offer patients buprenorphine initiation in the ED, how to overcome common barriers to ED-initiated buprenorphine, and how to find reliable long-term treatment for patients upon discharge.
The Basics
In 2015, the Journal of the American Medical Association published a randomized controlled trial showing that initiating buprenorphine in the ED increased treatment engagement, and reduced self-reported opioid use.9 In 2019, the Annals of Emergency Medicine published an expert clinical management manuscript covering the management of opioid withdrawal in the ED with buprenorphine.10 Finally, in 2021 the American College of Emergency Physicians (ACEP) released a consensus statement recommending that providers offer to treat opioid use disorder with buprenorphine in the ED.11 Although some may perceive MOUD initiation as the role of outpatient providers, each additional step a patient must take before buprenorphine initiation leads to a drop-off in retention in treatment and exposes patients to a potential overdose death.12 Initiating buprenorphine in the ED has many beneficial effects for patients, including reducing acute care visits, decreasing hospital readmissions, decreasing the use of non-prescribed opioids, and reducing all-cause mortality risk by 50%.13–15
There are also clinical benefits for providers who initiate buprenorphine in the ED. Buprenorphine is a partial agonist at the m opioid receptor and a weak antagonist at the k opioid receptor, with a higher affinity for the m opioid receptor and a slow dissociation which results in a longer duration of action compared to other agonists.16 This partial agonist quality leads to a plateau effect on respiratory depression at higher doses16,17 These specific properties confer a higher safety profile than other opioid agonists due to a ‘ceiling effect.’16,17 Since buprenorphine will not act as a complete agonist and plateaus, there is minimal respiratory depression compared to other opioid agonists such as heroin, morphine, and fentanyl.16,17 Furthermore there is minimal euphoria experienced by the patients leading to a decreased potential for abuse. Finally, compared to methadone, there is less of a risk of prolonging the QTc interval.16–18 In summary, if a patient presents following the pharmacologic reversal of an overdose from an unknown opioid, buprenorphine use can treat opioid overdose or withdrawal symptoms from naloxone reversal and will decrease the risk of apnea. Buprenorphine can also be a safer option for treating opioid withdrawal compared to methadone or some supportive medications in patients who have electrolyte abnormalities or who use other QTc-prolonging medications.
Barriers
Though the Accreditation Council for Graduate Medical Education (ACGME) has set requirements for an Emergency Medicine Residency to be accredited, residency training occurs in highly variable environments. Emergency departments with established protocols for initiating buprenorphine in the ED are still a novelty. Accordingly, most current emergency medicine residents train in a department with no set protocol for initiating buprenorphine. Furthermore, there is no specific ACGME requirement or single resource for teaching residents how to initiate buprenorphine. There are no unified recommendations regarding the timing and dosing of buprenorphine. Guo et al. recently reviewed buprenorphine protocols nationwide, highlighting widespread variability and concluding that future research should focus on the variation in protocols and patient outcomes.19 In May 2022, the Annals of Emergency Medicine published the results of Project ED Health which highlights how four diverse urban, academic medical centers implemented different protocols for ED-initiated buprenorphine.20 This manuscript provides a template, shown below, for departments to utilize as a protocol for ED-initiated buprenorphine.20
Figure 1: Yale School of Medicine ED pathway to initiate buprenorphine (https://medicine.yale.edu/edbup/)

In addition to treatment algorithms, Yale School of Medicine Emergency Medicine also provides assessment tools and an overview of how to perform a brief negotiating interview. This resource also provides training videos for the screening brief intervention and referral to treatment (SBIRT) method for healthcare providers who are positioned to help patients with substance use disorders.
CA Bridge has a quick-start protocol that differs slightly from other published protocols in that it begins with higher doses of buprenorphine. CA Bridge protocol begins with 8-16 mg of buprenorphine as the starting dose for induction in the ED, as opposed to other protocols with initial doses of 4mg.
A recent review proposes a neuropharmacological working model to address the challenge of achieving opioid balance with the appropriate buprenorphine dose.21 This review covers different scenarios including macro-dosing and micro-dosing buprenorphine and presents data from clinical studies outlining the complexities of acute clinical success of buprenorphine induction.21 An emerging scenario in which macro-dosing buprenorphine induction in the ED may become more common is for patients who present with opioid-related complaints that are chronically exposed to fentanyl, which has different pharmacological properties than other opioids.21
Figure 2: CA Bridge ED Buprenorphine guide (https://cabridge.org/resource/buprenorphine-bup-hospital-quick-start)

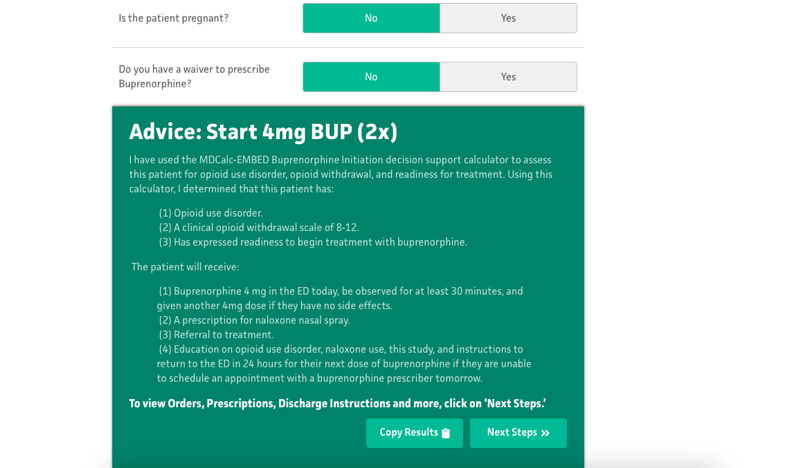
For physicians who prefer to learn on shift and are eager to offer buprenorphine to their patients with OUD, MDCalc has the Emergency Department-Initiated Buprenorphine for Opioid Use Disorder (EMBED) tool, shown below, which provides a step-by-step assessment tool with next steps including order sets and discharge instructions.
Figure 3: MD Calc ED-Initiated Buprenorphine guide (https://www.mdcalc.com/emergency-department-initiated-buprenorphine-opioid-use-disorder-embed)
The BUP Initiation App is available to be downloaded on cell phones. It provides an algorithm and next steps for providers initiating buprenorphine in the ED. If a provider has completed their X-waiver training, there is also an app called Buprenorphine Home Induction for unobserved buprenorphine induction. Using this app, the patient will be prescribed buprenorphine with specific instructions for taking buprenorphine at home once they start to experience more severe withdrawal symptoms. It is worth noting that once X-waiver training is completed, it never expires. As such, residents can complete their X-waiver training in residency and apply for their X-waiver once a DEA license is obtained after training. Providers Clinical Support System provides free online X-waiver training. Additionally, the American Medical Association has partnered with the American Society of Addiction Medicine to offer a free mini-course on prescribing buprenorphine for healthcare providers.
For clinicians looking to initiate buprenorphine in the ED, the goal is to wait until mild-to-moderate withdrawal symptoms develop before the first dose of buprenorphine. From the Guo et al study, most sites surveyed recommended a minimum COWS score of 8.9 Additionally, for sites that did have recommendations for periods of abstinence from full opioid agonists before buprenorphine initiation, most recommended 12 hours for short-acting opioids, 24 hours for long-acting opioids, and 48-72 hours for methadone.9 While the optimal initial dose of buprenorphine is not known and likely depends on the degree of severity of withdrawal and risk of precipitated withdrawal., 4mg of buprenorphine is a common initial dose.22
An additional barrier to prescribing buprenorphine is recency bias or the availability heuristic. Recency bias is a type of cognitive bias in which recent events are more likely to impact a decision or judgment more than distant events. EM physicians likely succumb to recency bias and heuristics daily. The Annals of Emergency Medicine published a manuscript on this topic in 2021, showing evidence that emergency physicians likely fall prey to the availability heuristic often.23 To overcome this, physicians who have had a bad experience with one patient who has OUD should take care not to carry any bias from that experience into their next encounter with a patient who has OUD. Physicians’ attitudes and biases may very well be another barrier that is contributing to the slow adoption of ED-initiated buprenorphine around the nation. Developing a culture of prescribing buprenorphine for OUD in the ED and having local departmental champions can increase the confidence of individual prescribers in the ED initiating buprenorphine.24 Financial incentives can also increase the uptake of X-waiver training in individual emergency departments, which will increase the number of clinicians who can prescribe buprenorphine.25
Importantly, it is a misconception that ED clinicians cannot administer buprenorphine in the ED without an X-waiver. Short-term treatment with direct administration of an opioid approved for use in maintenance or detoxification (e.g. methadone and buprenorphine) in the ED is allowed under the Drug Addiction Treatment Act of 2000, and the patient may return to the ED daily to receive the medication for up to 72 hours under the “3-day rule.”10 Having patients return to the ED for additional doses of buprenorphine may also be helpful to have them present during hours when social workers or clinical resource managers will be available to help connect them to outpatient care.
Beyond
Ensuring safe and dependable follow-up for patients should be a priority for Emergency Physicians. Follow-up care might be the most important component of ED-initiated buprenorphine. Follow-up availability can vary from state to state, region to region, and even hospital to hospital. A few options for mitigating this barrier are to familiarize oneself with local harm reduction clinics as some have buprenorphine clinics or at least know the providers in the area that prescribe buprenorphine. Physicians should research whether their hospital has an addiction team or a bridge clinic and if social work is able to help with managing the care of patients with OUD. Some communities are allocating significant resources to help improve access to buprenorphine. The New York City Department of Health and Mental Hygiene dedicated funding to establish the Buprenorphine Nurse Care Manager Initiative (BNCMI) to increase the capacity of primary care providers offering buprenorphine in safety-net settings.26 This model proved to be highly successful in increasing access to buprenorphine for patients who reside in high-poverty neighborhoods comprised of primarily non-Hispanic Black and Hispanic populations. From 2016 to 2020 the BNCMI was able to enroll 1212 new patients, most of whom identified as Hispanic and had public health insurance coverage.26 This model was adapted from the Massachusetts Model of Office-Based Opioid Treatment with Buprenorphine, as such, there might be similar initiatives in other states nationwide – something that would take minimal time for healthcare providers to familiarize themselves with. Cunningham et al. showed that despite the overwhelming increase in opioid overdoses during the COVID-19 pandemic, a primary care-based buprenorphine clinic was able to maintain OUD treatment for patients referred to their clinic and found that treatment retention improved during the pandemic compared to before the pandemic.27
Martin et al. reviewed three different types of follow-up options providers can utilize after initiating buprenorphine in the ED: (1) the Project Alcohol and Substance Abuse Services and Referral to Treatment (ASSERT) model, (2) the Bridge model, and (3) the ED-Bridge model.28 To summarize, the Bridge and the ED-Bridge models require buy-in from the department. In the Bridge model, the ED provider initiates buprenorphine, prescribes a short course of buprenorphine, and has a follow-up provider within the same hospital.28 The ED-Bridge is a model in which a dual-trained Emergency Medicine/Addiction Medicine physician can screen and initiate buprenorphine in the ED and then provide longitudinal care.28 The ASSERT model is an alternative that utilizes peer educators and community workers in the ED that help refer the patient to local addiction treatment services.28
Depending on location, there may be a large referral system such as in New York and California. New York Medication for Addiction Treatment and Electronic Referrals (MATTERS) is a state-wide system to support ED-initiated buprenorphine and urgent referrals to long-term care.29 CA Bridge is similar in that it provides follow-up options for patients throughout California who are initiated on buprenorphine. However, providers and patients may not have the luxury of a state-wide referral system for longitudinal treatment after buprenorphine initiation in the ED. The American Journal of Emergency Medicine recently published a manuscript showing the scalability of the SBIRT screening, treatment, and referral method.30 This method is effective and generally easily implemented in EDs.30 If physicians do not have access to a large referral network for follow-up treatment for patients with OUD, there may be harm reduction clinics nearby to which they can refer patients. If possible, physicians should always discharge patients with OUD with naloxone. During the COVID-19 pandemic, telemedicine became a popular option to continue with treatment for patients utilizing MOUD.31 Weintraub et al. published results showcasing the utility of combining telemedicine with mobile treatment.32 They found that a combined telemedicine-mobile treatment model for the initiation of buprenorphine provided similar results to office-based telemedicine MOUD models.32 Although they primarily focused on the utilization of the combined telemedicine mobile treating model for rural populations, there is no reason this could not be applied for anyone, anywhere, anytime.
Summary
1 – Treating OUD in the ED matters. It is lifesaving, and it is the duty of physicians to offer patients the resources to get the help they need.
2 – The basics of ED-initiated buprenorphine are as easy as opening MDCalc
3 – Due to wide local variability, physicians should research available local resources for patients with OUD and how to arrange safe and reliable follow-up for patients with OUD.
References
- Ahmad F, Rossen L, Sutton P. Provisional Drugs Overdose Death Counts.; 2021.
- Soares WE, Melnick ER, Nath B, et al. Emergency Department Visits for Nonfatal Opioid Overdose During the COVID-19 Pandemic Across Six US Health Care Systems. Ann Emerg Med. 2022;79(2):158-167. doi:10.1016/j.annemergmed.2021.03.013
- D’Onofrio G, Venkatesh A, Hawk K. The Adverse Impact of Covid-19 on Individuals with OUD Highlights the Urgent Need for Reform to Leverage Emergency Department–Based Treatment. Nejm Catal Innov Care Deliv. 2020;(May).
- Rhee TG, D’Onofrio G, Fiellin DA. Trends in the Use of Buprenorphine in US Emergency Departments, 2002-2017. JAMA Netw open. 2020;3(10). doi:10.1001/jamanetworkopen.2020.21209
- Hawk KF, D’Onofrio G, Chawarski MC, et al. Barriers and Facilitators to Clinician Readiness to Provide Emergency Department-Initiated Buprenorphine. JAMA Netw open. 2020;3(5). doi:10.1001/jamanetworkopen.2020.4561
- Goedel WC, Shapiro A, Cerdá M, Tsai JW, Hadland SE, Marshall BDL. Association of Racial/Ethnic Segregation with Treatment Capacity for Opioid Use Disorder in Counties in the United States. JAMA Netw Open. 2020;3(4). doi:10.1001/jamanetworkopen.2020.3711
- Kilaru AS, Kilaru AS, Xiong A, et al. Incidence of Treatment for Opioid Use Disorder following Nonfatal Overdose in Commercially Insured Patients. JAMA Netw Open. 2020;3(5). doi:10.1001/jamanetworkopen.2020.5852
- Stevens MA, Tsai J, Savitz ST, et al. Trends and Disparities in Access to Buprenorphine Treatment Following an Opioid-Related Emergency Department Visit Among an Insured Cohort 2014-2020. JAMA Netw Open. 2022;5(6).
- D’Onofrio G, O’Connor PG, Pantalon M V., et al. Emergency department-initiated buprenorphine/naloxone treatment for opioid dependence: A randomized clinical trial. JAMA – J Am Med Assoc. 2015;313(16):1636-1644. doi:10.1001/jama.2015.3474
- Herring AA, Perrone J, Nelson LS. Managing Opioid Withdrawal in the Emergency Department With Buprenorphine. Ann Emerg Med. 2019;73(5):481-487. doi:10.1016/j.annemergmed.2018.11.032
- Hawk K, Hoppe J, Ketcham E, et al. Consensus Recommendations on the Treatment of Opioid Use Disorder in the Emergency Department. Ann Emerg Med. 2021;78(3):434-442. doi:10.1016/j.annemergmed.2021.04.023
- Khalid L, Cunninghma C, Deng Y, et al. Cascade of care for office-based buprenorphine treatment in Bronx community clinics. J Subst Abuse Treat. 2022;139(108778).
- Wakeman SE, Larochelle MR, Ameli O, et al. Comparative Effectiveness of Different Treatment Pathways for Opioid Use Disorder. JAMA Netw Open. 2020;3(2). doi:10.1001/jamanetworkopen.2019.20622
- Moreno JL, Wakeman SE, Duprey MS, Roberts RJ, Jacobson JS, Devlin JW. Predictors for 30-Day and 90-Day Hospital Readmission Among Patients With Opioid Use Disorder. J Addict Med. 2018;12(6). doi:10.1097/ADM.0000000000000437
- Pearce LA, Min JE, Piske M, et al. Opioid agonist treatment and risk of mortality during opioid overdose public health emergency: Population based retrospective cohort study. BMJ. 2020;368. doi:10.1136/bmj.m772
- Sporer KA. Buprenorphine: A Primer for Emergency Physicians. Ann Emerg Med. 2004;43(5). doi:10.1016/j.annemergmed.2003.11.006
- Cisewski DH, Santos C, Koyfman A, Long B. Approach to buprenorphine use for opioid withdrawal treatment in the emergency setting. Am J Emerg Med. 2019;37(1). doi:10.1016/j.ajem.2018.10.013
- Poole SA, Pecoraro A, Subramaniam G, Woody G, Vetter VL. Presence or Absence of QTc Prolongation in Buprenorphine-Naloxone among Youth with Opioid Dependence. J Addict Med. 2016;10(1). doi:10.1097/ADM.0000000000000176
- Guo CZ, D’Onofrio G, Fiellin DA, et al. Emergency department‐initiated buprenorphine protocols: A national evaluation. J Am Coll Emerg Physicians Open. 2021;2(6):1-11. doi:10.1002/emp2.12606
- Whiteside LK, D’Onofrio G, Fiellin DA, et al. Models for Implementing Emergency Department–Initiated Buprenorphine with Referral for Ongoing Medication Treatment at Emergency Department Discharge in Diverse Academic Centers. Ann Emerg Med. Published online 2022. doi:10.1016/j.annemergmed.2022.05.010
- Greenwald MK, Herring AA, Perrone J, Nelson LS, Azar P. A Neuropharmacological Model to Explain Buprenorphine Induction Challenges. Published online 2022:1-16.
- Spadaro A, Long B, Koyfman A, Perrone J. Buprenorphine precipitated opioid withdrawal: Prevention and management in the ED setting. Am J Emerg Med. 2022;58(August 2022):22-26.
- Ly DP. The Influence of the Availability Heuristic on Physicians in the Emergency Department. Ann Emerg Med. 2021;78(5):650-657. doi:10.1016/j.annemergmed.2021.06.012
- Lowenstein M, Kilaru A, Perrone J, et al. Barriers and facilitators for emergency department initiation of buprenorphine: A physician survey. Am J Emerg Med. 2019;37(9). doi:10.1016/j.ajem.2019.02.025
- Foster SD, Lee K, Edwards C, et al. Providing Incentive for Emergency Physician X-Waiver Training: An Evaluation of Program Success and Postintervention Buprenorphine Prescribing. Ann Emerg Med. 2020;76(2). doi:10.1016/j.annemergmed.2020.02.020
- Kaplan-Dobbs M, Kattan JA, Tuazon E, Jimenez C, Saleh S, Kunins H V. Increasing access to buprenorphine in safety-net primary care clinics: The new york city buprenorphine nurse care manager initiative. Am J Public Health. 2021;111(2). doi:10.2105/AJPH.2020.306000
- Cunningham CO, Khalid L, Deng Y, et al. A comparison of office-based buprenorphine treatment outcomes in Bronx community clinics before versus during the COVID-19 pandemic. J Subst Abuse Treat. 2022;135. doi:10.1016/j.jsat.2021.108641
- Martin A, Butler K, Chavez T, et al. Beyond Buprenorphine: Models of Follow-up Care for Opioid Use Disorder in the Emergeny Department. West J Emerg Med. 2020;21(6):257-263. doi:10.5811/WESTJEM.2020.7.46079
- Irvine UC, Rachel A, Susan J. Implementing a Novel Statewide Network to Support Emergency Department-initiated Buprenorphine Treatment. Published online 2022. doi:10.5811/westjem.2022.3.54680
- Monico LB, Oros M, Smith S, Mitchell SG, Gryczynski J, Schwartz R. One million screened: Scaling up SBIRT and buprenorphine treatment in hospital emergency departments across Maryland. Am J Emerg Med. 2020;38(7). doi:10.1016/j.ajem.2020.03.005
- Buchheit BM, Wheelock H, Lee A, Brandt K, Gregg J. Low-barrier buprenorphine during the COVID-19 pandemic: A rapid transition to on-demand telemedicine with wide-ranging effects. J Subst Abuse Treat. 2021;131. doi:10.1016/j.jsat.2021.108444
- Weintraub E, Seneviratne C, Anane J, et al. Mobile Telemedicine for Buprenorphine Treatment in Rural Populations with Opioid Use Disorder. JAMA Netw Open. 2021;4(8):1-11. doi:10.1001/jamanetworkopen.2021.18487




