
Authors: Tony Mathew, MD (EM Resident Physician, UTSW/Parkland, Dallas, TX) and Taylor Terlizzese, OMS-IV (Medical Student, TCOM, Fort Worth, TX) // Reviewed by: Sophia Görgens, MD (EM Resident Physician, Zucker-Northwell NS/LIJ, NY); Cassandra Mackey, MD (Assistant Professor of Emergency Medicine, UMass Chan Medical School); Brit Long, MD (@long_brit); Alex Koyfman, MD (@EMHighAK)
Welcome to EM@3AM, an emDOCs series designed to foster your working knowledge by providing an expedited review of clinical basics. We’ll keep it short, while you keep that EM brain sharp.
A 75-year-old male with a history of hypertension and hypothyroidism presents to the ED with 4 days of abdominal distention, constipation, and decreased PO intake due to nausea. He reports that his symptoms are worse after eating or drinking and that he is able to pass gas but has not had a bowel movement in the past 4 days.
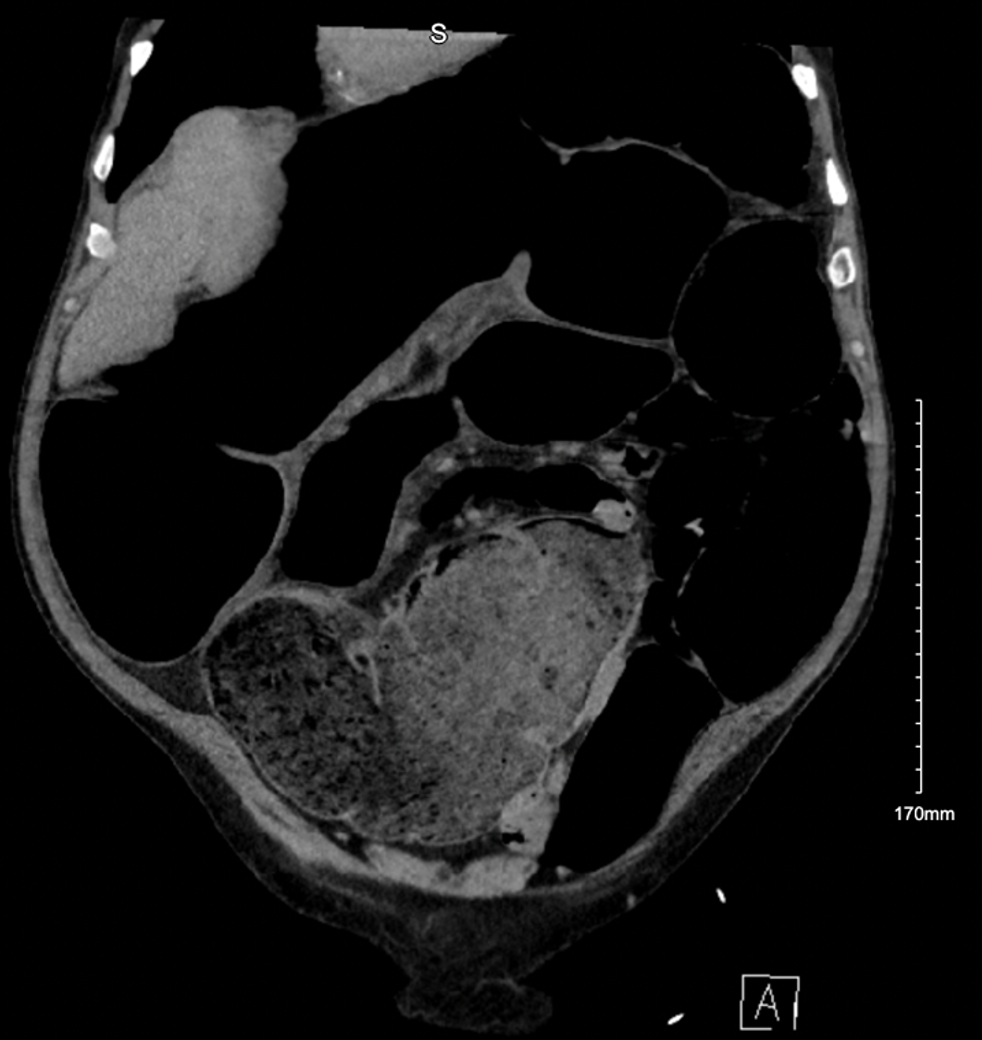
On initial presentation to the ED, the patient’s vitals are notable for mild hypertension of 150/102, but otherwise he is afebrile, HR 87, and oxygen saturation 100% on room air. His EKG is normal sinus rhythm with no ischemic changes. On exam, he appears anicteric while his abdomen is soft, non-tender, but massively distended asymmetrically with no bowel sounds heard on auscultation. Initial labs are notable for K 3.0, WBC 10.6 BUN, and Cr 1.45 (prior level 1.3). Initial POCUS abdominal ultrasound shows no fluid collection concerning for ascites. CT Abdomen/Pelvis with contrast reveals the following:

What is the most likely diagnosis?
Answers: Sigmoid Volvulus
Epidemiology:
- A sigmoid volvulus is an uncommon but potentially life-threatening cause of large bowel obstruction (LBO). Representing only 5% of LBOs, a sigmoid volvulus may initially present with mild symptoms but can quickly result in large bowel perforation if left untreated.1
- Patients with a sigmoid volvulus are most likely to be men with a mean age of 70 and a history of constipation.2
- Risk factors for a sigmoid volvulus include causes of sigmoid dilation such as Crohn’s disease, redundant colon, constipation, Hirschsprung’s disease and, more commonly in developing nations, Chagas disease.3-5
- Immobility and altered mental status also contribute to constipation, dilating the sigmoid colon and setting the stage for a sigmoid volvulus. Up to 71% of sigmoid volvulus are associated with neuropsychiatric disease, supporting the association with incapacitation.6
Pathophysiology:
- A volvulus of the sigmoid colon occurs when an air-filled sigmoid torses around its mesenteric attachments. As the segment torses, the lumen becomes obstructed while stool and gas continue to fill the proximal colonic segment causing distention. If left untreated, the torsed segment’s vasculature can become impaired and result in bowel ischemia.8
- Additionally, the severity of the presentation may mirror the extent of torsion with 180º rotation blocking stool transit and 360º rotation sufficiently obstructing arterial flow to the tissue. In the absence of ischemia, the mortality rate of sigmoid volvulus is less than 5%; however, if arterial flow is compromised, bowel ischemia may result in gangrenous bowel which increases mortality to nearly 50%.7
Evaluation:
- A sigmoid volvulus will often present with symptoms of gradually worsening nausea, constipation, abdominal distention, and abdominal pain that can be colicky in nature associated with peristalsis.12
- The time course for a sigmoid volvulus to develop into a painful, distended abdomen is only a few days; however, gangrenous bowel and perforation may be seen early in the disease course and should be suspected in patients who present with fever, hemodynamic instability, or peritonitis.12
- On physical exam, the abdomen is expected to be distended and tympanic, potentially with diminished bowel sounds. A patient that presents with severe, sharp abdominal pain, fever, and abdominal rigidity is worrisome for gangrene that has resulted in perforation and peritonitis.
- Classically, plain films are sufficient to diagnose a sigmoid volvulus. The distended sigmoid will appear as a dilated loop of bowel without haustral markings, absence of air in the rectum, and characteristically has a “bent inner-tube” or “U-shaped tube” appearance, called the “coffee bean sign.”9
- However, plain films only established the diagnosis of sigmoid volvulus in around 60% of cases because other causes of distal colon obstruction may present with similar radiographic findings.6
- CT abdomen/pelvis with contrast can be more appropriate to delineate sigmoid volvulus from other causes of distal colon obstruction such pseudo-obstruction (Ogilvie’s syndrome), toxic megacolon, and neoplastic disease.
- The abdominal CT will show a whirl pattern of the sigmoid due to the torsion of the mesentery and vessels as well as a “bird beak” appearance proximal and distal to the obstructed segment. While CT abdomen has 100% sensitivity and 90% specificity for sigmoid volvulus, emergent surgical intervention when required in the setting of bowel perforation and peritonitis should not be delayed for CT.9
Treatment:
- In addition to routine lab work such as CBC and CMP to assess for leukocytosis and secondary electrolyte abnormality, serum lactate is a useful marker for bowel ischemia. IV fluid resuscitation is indicated in patients with signs of shock or unstable vital signs. Early administration of broad-spectrum IV antibiotics after obtaining blood cultures is indicated to control bacterial translocation across ischemic intestinal wall. 12
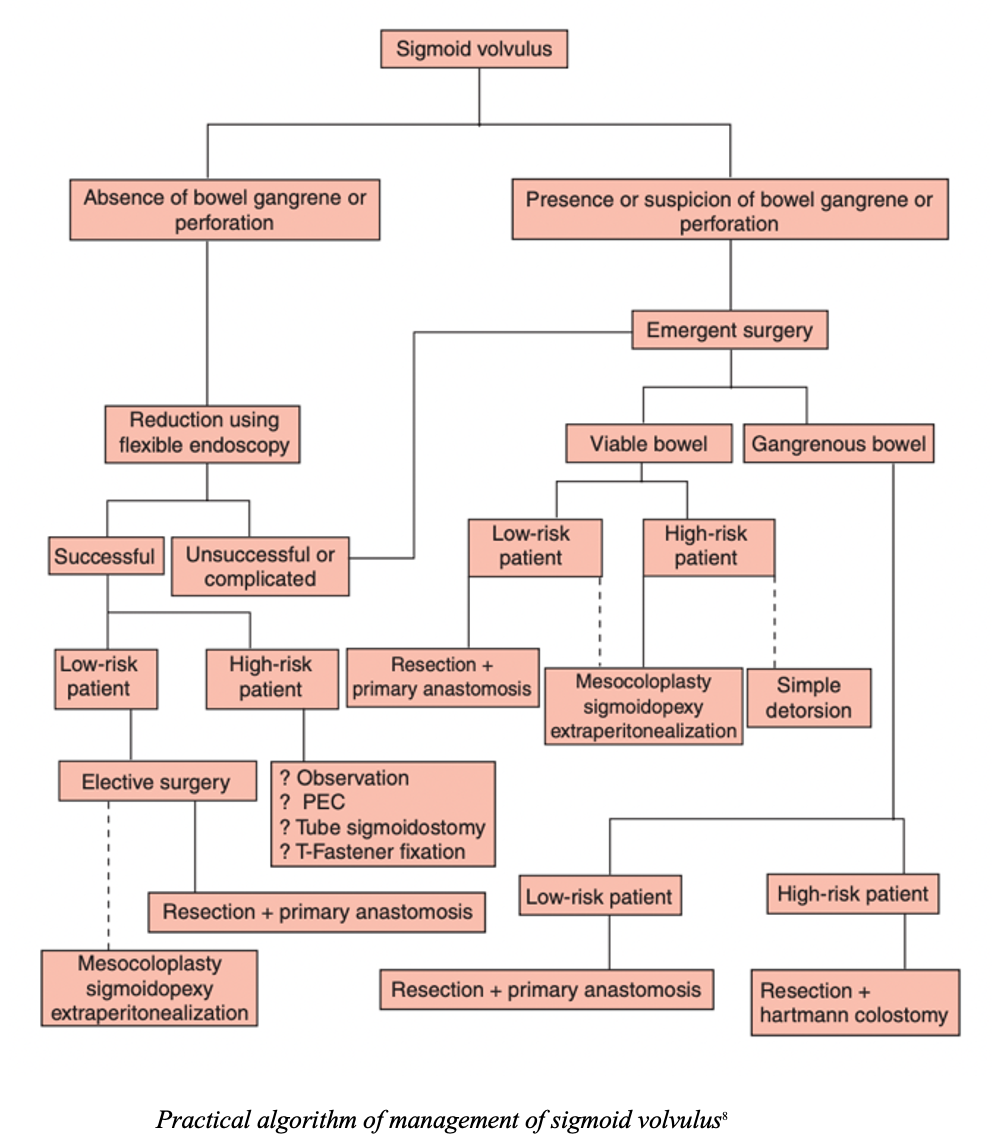
- The relief of obstruction and prevention of recurrence are the two cardinal goals of sigmoid volvulus management.7
- Patients with alarming signs consistent with bowel perforation, bowel compromise, or peritonitis should receive emergent surgical intervention with resection and primary anastamosis.7
- In patients without alarming signs, the American Society of Colon and Rectal Surgeons recommends an endoscopic decompression via sigmoidoscopy, given that spontaneous detorsion is generally uncommon.7,10
- A sigmoidoscope is placed with insufflation into the torsed segment and used to straighten the sigmoid, returning blood flow and patency to the lumen. Endoscopic decompression is effective in detorsion of approximately 85% of sigmoid volvuli.11
- However, non-operative reduction of sigmoid volvulus does not constitute adequate treatment as high rates of recurrence and high mortality is associated with non-operative reduction1 Elective resection of the sigmoid colon and anastomosis (ELRSA) is the gold standard with a mean mortality of 8%, a mean recurrence of 1.2% and a morbidity of 13–26%.7
Disposition:
- Initial urgent sigmoidoscopy is important to de-torse the sigmoid volvulus. If detorsion is successful, prognosis is very good, and the patient can be admitted for observation and with planned elective surgical resection either inpatient or outpatient to prevent recurrence.
- Outcomes for sigmoid volvulus are significantly worse in patients who develop bowel gangrene; therefore, emergent surgical intervention is critical to patient outcomes in the setting of LBOs.
Pearls:
- Patients with suspected sigmoid volvulus that present with symptoms of bowel gangrene or perforation – hemodynamic instability, fever, obstipation, abdominal rigidity – require emergent surgical intervention. Manage ABCs, administer IV fluids and broad-spectrum
- Plain films are sensitive but are not specific for sigmoid volvulus. Look for the classic ‘coffee bean sign’. CT non-contrast can be used to confirm sigmoid volvulus or identify alternative causes of LBO.
- Prognosis of sigmoid volvulus is good if detected early with initial treatment of endoscopic decompression via sigmoidoscopy. However, high rates of recurrence and high mortality is associated with solely non-operative reductions.
- Gold standard treatment for sigmoid volvulus involves elective resection of the sigmoid colon and anastomosis (ELRSA).




