Originally published at EM Cases – Visit to listen to accompanying podcast. Reposted with permission.
Follow Dr. Anton Helman on twitter @EMCases
Podcast production, sound design & editing by Anton Helman. Voice editing by Sucheta Sinha.
Written Summary and blog post by Shaun Mehta & Anton Helman, December, 2018
Cite this podcast as: Helman, A, Bosman, K, Hicks, C, Petrosoniak, A. Trauma – The First and Last 15 Minutes Part 1. Emergency Medicine Cases. December, 2018. https://emergencymedicinecases.com/trauma-first-last-15-minutes-part-1/. Accessed [date].
Prepare the team, your gear and yourself for trauma resuscitation
Preparing the team for trauma
Prepare your team in the few minutes prior to the patient arriving in your ED based on the little information you have garnered from the EMS call, so that this complex logistical co-ordination can occur as an efficient flow [1].
Team-Based Preparation: 4 Discussion Points
- What do we know? The stem that you receive from the EMS call
- What do we expect to see/What are the possibilities? Run through the most likely immediate life-threatening issues/injuries
- What do we do? And discuss contingencies if those actions fail. What is your response if the initial plan fails or does not produce expected results?
- Role assignment. Assign logistical tasks to team members.
Team Preparation with Hicks from SMACC
Preparing the gear for trauma resuscitation
Ensure that your ED has a well thought out trauma cart that clearly contains the gear that you may require, including a pelvic binder, thoracostomy kit, cricothyrotomy kit etc. When assigning roles, assign gear preparation with each role.
Preparing yourself for trauma resuscitation
Mental preparation, including visualization of complex tasks, deep breathing exercises, and positive self-talk to help focus. See Weingart’s ‘Beat the Stress Fool‘ technique.
Consider calling for help early (anesthesia, surgery, orthopaedics, paediatrics etc) if you work in a center that does not have a dedicated trauma team. Tie up loose ends with other patients in your ED if time permits before the trauma patient arrives, so that after you’re done managing the trauma patient, your ED is not a disaster zone.
Resequencing the trauma resuscitation
Intubation causes an increase in intrathoracic pressure, resulting in a decrease in right atrial pressure which negatively impacts both hemorrhagic and obstructive shock. Pre-intubation hypotension is a significant risk factor for postintubation cardiac arrest. Hence, the adage “resuscitate before you intubate” in volume depleted patients, and procedures to relieve obstructive shock such as bilateral finger thoracostomies and thoracotomy, should be considered prior to endotracheal intubation.
Focus on physiologic priorities rather than always “ABC”. Tailor your approach to the most severe life-threatening injuries first. Vocalize your assessment and plan.
Two categories of immediate life-threats in trauma:
- Massive external hemorrhage
- Critical airway compromise a) critical/refractory hypoxia (<90% oxygen saturation despite maximal noninvasive ventilation) b) dynamic airway (anticipate evolving disruption of airway, head/neck injuries that are expected to worsen over the next few minutes)
Once these two immediate life threats have been ruled out or managed, resuscitation should focus on hemodynamic optimization before definitive airway management.

Source – Resuscitation Resequenced: A Rational Approach to Patients with Trauma in Shock. Emergency Medicine Clinics of North America [2].
Occult shock in trauma resuscitation
The early identification of occult shock is important because under-recognition is associated with worse patient outcomes.
How to assess for occult shock in the first 15 minutes of trauma resuscitation
- Calculate the Shock index (HR/SBP) [10] and/or delta Shock Index; if shock index > 1 or delta Shock Index ≥ 0.1, assume occult shock
- Assess the lowest BP measured and trend of BP over time; if isolated or persistent SBP <110, assume occult shock [7]
- FAST positive with flat IVC
- Feel for the presence of peripheral pulses and look for signs of poorly perfused extremities
- Altered LOA in the absence of severe head injury
Shock index >1 or Delta Shock Index ≥0.1 is a sign of occult shock and is predictive of post-intubation hypotension, transfusion requirements, injury severity and mortality
A single drop in BP in the field or in the ED is predictive of need for surgical intervention and mortality. An isolated decrease in SBP <105 mmHg is associated with a 12-fold increase in the need for immediate therapeutic intervention [6].
Pearl: When receiving handover from EMS ask not only the most recent BP but the lowest BP recorded.
Shock index is predictably unreliable in the following circumstances
- Altered physiologic compensation (e.g. older patients [9]) – consider *delta shock index
- Presence of underlying medical conditions (eg.. undertreated hypertension)
- Medication-related disturbances (e.g. B-blockers)
*Delta shock index ≥0.1 predicts increased transfusion requirements and mortality and may be a more useful prognostication tool than shock index, especially in older patients and those with a history of untreated hypertension.
Pitfall: Prehospital hypotension that normalizes without intervention that is ignored. A single prehospital drop in BP may be a clue to impending catastrophic shock.
Early actions to consider in the first 15 minutes of trauma resuscitation
- Direct pressure/tourniquet on wounds/splint obvious fractures
- Bilateral finger thoracostomies
- Pelvic binder application
- IV tranexamic acid
- Blood products/massive transfusion protocol
- Call to trauma center – request transfer/retrieval as soon as the need for higher level of trauma care is presumed
- Vasopressors only if neurogenic shock suspected
Vascular access in the first 15 minutes of trauma resuscitation
Two short large bore peripheral IVs are recommended for initial vascular access in the trauma patient.
If a peripheral IV cannot be rapidly obtained a humerus IO with pressure bag has adequate infusion rates but should be used only as a bridge to venous access and should be checked frequently for flow.
A central line is not mandatory if two well running peripheral lines are established but should be considered for patients requiring long transport times or when REBOA is being planned.
Volume resuscitation, volume challenge, controlled resuscitation and early resuscitation targets
Consider the following before volume resuscitation. The patient that is bleeding may not appear to be in shock, and the patient who is in shock may not be actively bleeding. Your job is to not only identify shock/occult shock but to identify active bleeding, obstructive and neurogenic shock.
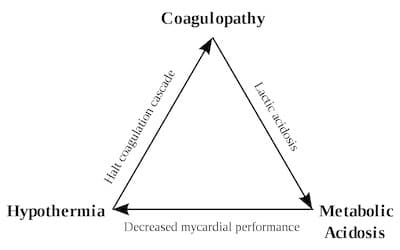
Large volumes of crystalloid contribute to the trauma “triangle of death” (metabolic acidosis, hypothermia and coagulation derangements).
Consider a volume challenge to assess for active occult hemorrhage. 250mL of crystalloid under pressure followed by assessment of signs of perfusion. If a patient transiently responds to 250mL of crystalloid, you may assume active occult hemorrhage. If there is no response consider other causes of shock (obstructive, neurogenic). If you suspect active occult hemorrhage based on severe mechanism (e.g. fall from 7 stories), clinical assessment and/or volume challenge, start blood products ASAP.
Controlled resuscitation (previously termed “permissive hypotension”)[13]. While there are fairly well studied resuscitation targets in the first few hours of trauma resuscitation (urine output, lactate clearance, base deficit etc), there is little to guide us in the first 15 minutes of trauma resuscitation. If there is a delay to starting blood transfusion in a patient presumed to have hemorrhagic shock, consider only small boluses of crystalloid (i.e. 250mL), just enough to maintain adequate tissue perfusion (peripheral pulses present in blunt trauma or central pulses in penetrating injury) and maintain a SBP ≥ 70. For most trauma patients consider targeting this SBP throughout your resuscitation. This approach has been termed “Controlled Resuscitation” and is recommended by our experts a reasonable early resuscitation target. One prospective RCT showed a NNT of 11 for inhospital mortality [13]. Keep in mind the elderly patient, the patient with uncontrolled hypertension at baseline, the patient with a major head injury and the patient with neurogenic shock, may require adjustment in their BP target.
Indications for massive transfusion and resuscitation intensity in trauma resuscitation
Formula to assess which patients need massive transfusion protocol (MTP)
Clinical judgement + Mechanism of injury + Pitfall conditions
It is important to identify early on if your patient requires MTP and the logistics of how to administer it.
Step 1: If the patient is in an obvious shock state, or shock index is >1 [11], or delta shock index is ≥0.1 [16], or has an ABC score ≥ 2* [14], activate the MTP.
Step 2: If none of these are present, consider the resuscitation intensity [19,20]: patients who require 4 units of any combination of crystalloids or blood products to maintain adequate perfusion are considered to have high resuscitation intensity which predicts higher mortality, and should be considered for a MTP.
*ABC score [14]
1 point for each of: penetrating injury, positive FAST, SBP ≤90, HR ≥120.
A score of ≥2 indicates requirement for activation of MTP
Pitfall conditions – consider a lower threshold for activating MTP
- Anticoagulation – patients taking anticoagulants are not well represented in MTP studies; have a lower threshold for calling for blood
- Elderly
- Medications such as B-blockers
How to give MTP
Give the MTP in balanced blood products 1:1:1 [18]. Although the ratio of red cells to FFP to platelets is meant to be 1:1:1 over the first 24hrs, that does not mean the patient requires FFP and platelets immediately in the ED. Rather, give 4 units of red cells up front as they can usually be delivered faster that FFP and platelets.
Take Home Points for Trauma – The First and Last 15 Minutes Part 1
- Prepare your team, your gear and yourself prior to patient arrival with 4 discussion points, assigning specific gear preparation to specific team members and mental preparation
- Resequence the trauma resuscitation by managing massive external hemorrhage and active/dynamic airway first, then concentrating on hemodynamic optimization before definitive airway management in those patients without active/dynamic airways
- Identify occult shock using shock index >1, delta shock index ≥0.1, the lowest BP recorded, FAST/IVC, a fluid challenge and clinical exam
- Consider the patient’s age, blood pressure medications and baseline blood pressure in assessing for occult shock, interpreting the shock index and in deciding to activate massive transfusion protocol
- Early actions to consider include control of massive external hemorrhage, bilateral finger thoracostomies, pelvic binder, tranexamic acid, activation of massive transfusion protocol and call for help
- Two large bore IVs are the preferred initial access in most trauma patients
- Avoid transferring a patient long distances with IO access only
- Large volumes of crystalloid may lead to the “triangle of death”; your goal should be no crystalloid
- Controlled resuscitation to a target SBP of ≥70 is reasonable in most young, otherwise healthy trauma patients presumed to be in hemorrhagic shock
- Use clinical judgement, mechanism of injury, pitfall conditions, shock index and resuscitation intensity to help in decisions to activate massive transfusion protocol
Management of trauma arrest Joe Nemeth’s Best Case Ever
Dr. Petrosoniak’s EMU 365 video talk on Massive Transfusion in Trauma
Best Case Ever on What We Can Learn from Prehospital Trauma Management
Episode 39 Trauma Literature Update
Drs. Bosman, Helman, Hicks, Mehta and Petrosoniak have no conflicts of interest to declare.
References
- Petrosoniak, A. Hicks, C. Beyond crisis resource management: new frontiers in human factors training for acute care medicine. Curr Opin Anaesthesiol. 2013 Dec;26(6):699-706.
- Petrosoniak A, Hicks C. Resuscitation Resequenced: A Rational Approach to Patients with Trauma in Shock. Emerg Med Clin North Am. 2018;36(1):41-60.
- Kim WY, Kwak MK, Ko BS, et al. Factors associated with the occurrence of cardiac arrest after emergency tracheal intubation in the emergency department. PLoS One 2014;9(11):e112779.
- Heffner AC, Swords DS, Neale MN, et al. Incidence and factors associated with cardiac arrest complicating emergency airway management. Resuscitation 2013;84(11):1500–4.
- Codner P, Obaid A, Porral D, et al. Is field hypotension a reliable indicator of significant injury in trauma patients who are normotensive on arrival to the emergency department? Am Surg 2005;71(9):768–71.
- Lipsky AM, Gausche-Hill M, Henneman PL, et al. Prehospital hypotension is a predictor of the need for an emergent, therapeutic operation in trauma patients with normal systolic blood pressure in the emergency department. J Trauma 2006;61(5):1228–33.
- Shapiro NI, Kociszewski C, Harrison T, et al. Isolated prehospital hypotension after traumatic injuries: a predictor of mortality? J Emerg Med 2003;25(2):175–9.
- Bilello JF, Davis JW, Lemaster D, et al. Prehospital hypotension in blunt trauma: identifying the “crump factor”. J Trauma 2011;70(5):1038–42.
- Oyetunji TA, Chang DC, Crompton JG, et al. Redefining hypotension in the elderly: normotension is not reassuring. Arch Surg 2011;146(7):865–9.
- King RW, Plewa MC, Buderer NM, et al. Shock index as a marker for significant injury in trauma patients. Acad Emerg Med 1996;3(11):1041–5.
- Vandromme MJ, Griffin RL, Kerby JD, et al. Identifying risk for massive transfusion in the relatively normotensive patient: utility of the prehospital shock index. J Trauma 2011;70(2):384–8 [discussion: 388–90].
- Dutton RP, Mackenzie CF, Scalea TM. Hypotensive Resuscitation during Active Hemorrhage: Impact on InHospital Mortality. J Trauma. June 2002;52(6):1141-46.
- Schreiber MA, Meier EN, Tisherman SA, Kerby JD, Newgard CD, Brasel K, Egan D, Witham W, Williams C, Daya M, Beeson J, McCully BH, Wheeler S, Kannas D, May S, McKnight B, Hoyt DB; ROC Investigators. A Controlled Resuscitation Strategy is Feasible and Safe in Hypotensive Trauma Patients: Results of a Prospective Randomized Pilot Trial. J Trauma Acute Care Surg. Apr 2015;78(4):687-95.
- Nunez TC, Voskresensky IV, Dossett LA, Shinall R, Dutton WD, Cotton BA. Early prediction of massive transfusion in trauma: simple as ABC (assessment of blood consumption)?. J Trauma. 2009;66(2):346-52.
- Schroll R, Swift D, Tatum D, et al. Accuracy of shock index versus ABC score to predict need for massive transfusion in trauma patients. Injury. 2018;49(1):15-19.
- Schellenberg M, Strumwasser A, Grabo D, et al. Delta Shock Index in the Emergency Department Predicts Mortality and Need for Blood Transfusion in Trauma Patients. Am Surg. 2017;83(10):1059-1062.
- Nascimento B, Callum J, Tien H, et al. Effect of a fixed-ratio (1:1:1) transfusion protocol versus laboratory-results-guided transfusion in patients with severe trauma: a randomized feasibility trial Canadian Medical Association Journal. 2013; 185(12):E583-E589.
- Holcomb JB, Tilley BC, Baraniuk S, et al. Transfusion of Plasma, Platelets, and Red Blood Cells in a 1:1:1 vs a 1:1:2 Ratio and Mortality in Patients With Severe Trauma JAMA. 2015; 313(5):471-478.
- Rahbar E, Fox EE, Del junco DJ, et al. Early resuscitation intensity as a surrogate for bleeding severity and early mortality in the PROMMTT study. J Trauma Acute Care Surg. 2013;75(1 Suppl 1):S16-23.
- Meyer DE, Cotton BA, Fox EE, et al. A comparison of resuscitation intensity and critical administration threshold in predicting early mortality among bleeding patients: A multicenter validation in 680 major transfusion patients. J Trauma Acute Care Surg. 2018;85(4):691-696.




