
Author: Rachel Bridwell, MD (@rebridwell, EM Resident Physician, San Antonio, TX) // Reviewed by: Brit Long, MD (@long_brit, EM Attending Physician, San Antonio, TX) and Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UTSW / Parkland Memorial Hospital)
Welcome to EM@3AM, an emDOCs series designed to foster your working knowledge by providing an expedited review of clinical basics. We’ll keep it short, while you keep that EM brain sharp.
A 2-year-old male is brought to the ED by his mom for right ear pain and high fevers. His right ear is notably pushed forward. Mom reports a recent ear infection in that same ear. He denies any headache, weakness, neck stiffness. recent trauma, dental work, or travel. The patient is up to date on vaccinations. Review of systems is remarkable for a recent sinus infection.
Exam reveals BP 105/60, HR 133, T 102.3, RR 30, SpO2 98% on room air. He is alert but fussy. He has right auricular proptosis, mastoid redness, swelling and tenderness with loss of skin crease, and his right TM is protruded with erythema and purulence.
What’s the next step in your evaluation and treatment?
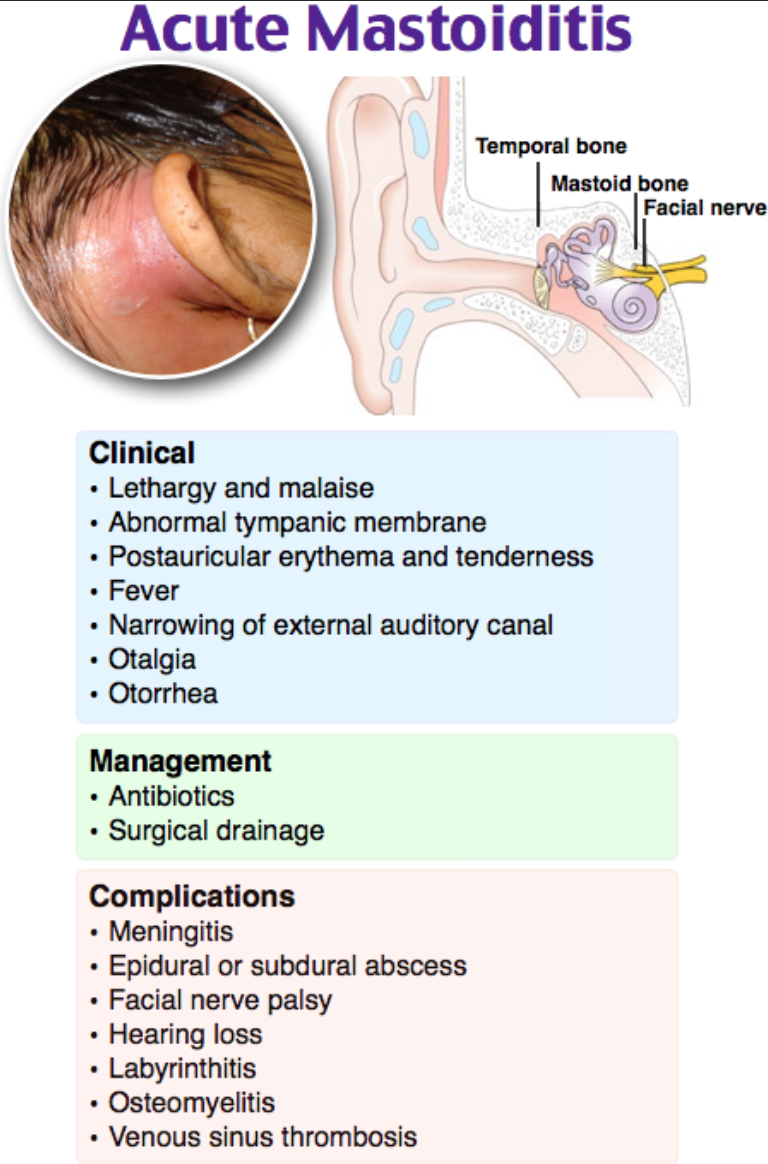
Answer: Mastoiditis1-14
Epidemiology:
- Incidence of 0.6-4.2/100,000 children per year1,2
- Most common complication of acute otitis media (AOM)3
- Middle ear infection extends to mastoid cells generating periostitis or osteitis4
- Retention of purulence generates increased pressure, which doesn’t allow mastoid and tympanic cavity to communicate, blocking eustachian drainage or TM perforation3
- 4% of AOM cases develop into mastoiditis5
- Younger children are more prone to mastoiditis—pneumatization of mastoid begins at birth and concludes around age 183
- 28% cases <1 years, 38% cases 1-4 years, 21% 4-8 years, 12%12-18 years.5
- 30% of pediatric patients with mastoiditis suffer from recurrent AOM5
- 3% of mastoiditis patients have receive antibiotics in the preceding 3 weeks5
- Causative bacteria: Upper respiratory flora both aerobic and anaerobic
- S. pneumonia, H. influenza, M. catarrhalis, S. pyogenes, S. aureus, P. aeruginosa, M. tuberculosis, Enterobacter5
- With new pneumococcal vaccination, rates of admission for mastoiditis and intracranial complications have remained the same6,7
- S. pneumonia, H. influenza, M. catarrhalis, S. pyogenes, S. aureus, P. aeruginosa, M. tuberculosis, Enterobacter5
- Middle ear infection extends to mastoid cells generating periostitis or osteitis4
Clinical Presentation:
- Signs and symptoms of acute otitis media are present in 1/3 of patients5
- 1/3 with symptoms for 1-2 days, while 1/3 with symptoms for 3-6 days
- Common in recurrent AOM, previous episodes of mastoiditis
Evaluation:
- Assess ABCs and obtain VS, to include visual acuity
- +/- fever8
- Perform a complete physical examination; mastoiditis is primarily a clinical diagnosis
- Evaluate ears to include otoscopy
- Erythema of the TM is present in 80%, while 3% of patients will have a normal TM5
- Mastoid tenderness, erythema, edema, tenderness (80% of patients)5
- Auricular proptosis
- Loss of skin crease
- Neuro: Focal neurologic deficits, CN III, IV, VI palsies
- Also assess for signs and symptoms of meningitis or subdural empyema
- ENT: dental exam to assess for tonsillar exudates and other concomitant infections
- Evaluate ears to include otoscopy
- Imaging: CT face to include mastoid—Will see air cell thickening and opacification as well as complications with contrast9
- Consider MRI to assess for complications, though clinical urgency precedes the need for sedation and delay to definitive management7
- Laboratory evaluation:
- CBC with differential
- Culture purulence from external auditory canal
- Utility in identifying S. aureus and P. aeruginosa 31% and 50% of the time, respectively5
- CRP is often elevated
Treatment:
- ABCs—If in the setting of toxic patient with potential encephalitis, meningitis, cerebral venous sinus thrombosis, subdural empyema, consider treatment to reduce elevated intracranial pressure9
- Antibiotics:
- Treat with broad spectrum antibiotics for 48 hours—target pneumoniae and other AOM causing bacteria
- 3rd generation cephalosporin with clindamycin or metronidazole
- Coverage for P. aeruginosa is not typically needed and should only be considered if there is no clinical response to initial empiric coverage
- Consult ENT for evaluation
- Mastoidectomy is the definitive treatment10
- Early mastoidectomy has been shown to prevent complications3,7
- Myringotomy commonly performed though 60% of cultures were negative5
- Consider neurosurgical consult if subdural empyema present
- Outpatient: ceftriaxone daily if uncomplicated and reliable social situation11
- In a systematic review of 564 pediatric patients, cure rates for surgical treatment was 96.3% while medical treatment was 95.9%10
- Note this study was performed outside the U.S. in settings with universal healthcare
- In a systematic review of 564 pediatric patients, cure rates for surgical treatment was 96.3% while medical treatment was 95.9%10
- Mastoidectomy is the definitive treatment10
Complications:
- Between 5-29% of patients will have intracranial complication7,12
- Greatest complication rates seen in patients with mastoiditis secondary to aureus5
- Recent antibiotic use for AOM generates more aggressive mastoiditis7
- Patients who have received recent antibiotics with CRP>93.5 mg/L have a 22x increased risk of intracranial complications7
- Venous sinus thrombosis—commonly sigmoid
- Anticoagulation—weigh risks of intracranial hemorrhage against benefit of lowering mortality and neurologic sequelae13
- No current studies to tailor anticoagulation in otogenic sigmoid sinus thromboses. The limited available data support choosing a readily reversible anticoagulant (ie, heparin, Vit K antagonists, and dabigatran) 13
- Subdural/epidural abscess—mastoiditis accounts for 14% of subdural empyema cases14
- Facial Paralysis
- Labyrinthitis
- Anticoagulation—weigh risks of intracranial hemorrhage against benefit of lowering mortality and neurologic sequelae13
Disposition: Admit with ENT consult
Pearls:
- Mastoiditis is primarily a clinical diagnosis
- 3% of mastoiditis patients will have normal TM5
- 60% of myringotomy fluid cultures are negative5
- Antibiotics and ENT consultation are needed

A 19-year-old woman with insulin-dependent diabetes mellitus presents with a left-sided headache and fever. Her vital signs are T 101.4ºF, HR 112 beats/minute, RR 12 breaths/minute, BP 105/70 mm Hg, and oxygen saturation 100% on room air. She has left postauricular erythema and tenderness to palpation. The remainder of her ear, nose, and throat exam is unremarkable. Which of the following is the best course of management for this patient?
A) Acyclovir and prednisone
B) Discharge with quinolone-steroid otic suspension
C) Intravenous ceftriaxone and admission
D) Magnetic resonance venogram and anticoagulation
Answer: C
The appropriate management for acute mastoiditis is with systemic antibiotics such as intravenous ceftriaxone and admission. Acute mastoiditis is a potential complication of otitis media, which should serve as a reminder to providers that otitis media is a not altogether a benign condition. Infection from the middle ear spreads contiguously to the mastoid air cells and results in blockage of the aditus ad antrum (a connecting passage in the temporal bone) and subsequent filling of the mastoid air cells with fluid and infectious debris. Streptococcus pneumoniae is the most common causative organism, with S. pyogenes and Pseudomonas aeruginosa causing a minority of cases. Clinical findings include postauricular erythema, swelling, and tenderness with loss of the postauricular crease. CT with contrast of the temporal bone confirms the clinical diagnosis. In addition to admission for IV antibiotics, tympanocentesis and myringotomy may be required. In aggressive cases, subperiosteal abscess drainage or mastoidectomy may be indicated.
Acyclovir and prednisone (A) are treatment options for severe cases of Bell’s palsy. The facial nerve (CN VII) may be affected by malignant otitis externa but is not as commonly affected by mastoiditis. This patient has no findings of facial droop, so this is an unlikely diagnosis. Discharge with quinolone-steroid otic suspension (B) is the preferred management for uncomplicated acute diffuse otitis externa (swimmer’s ear), which affects the external auditory canal and auricle but not the postauricular space. Magnetic resonance venogram and anticoagulation (D) is the diagnostic modality and treatment of choice for cerebral venous thrombosis, which may present with headache, pulsatile tinnitus, or cranial nerve deficits in patients at risk for venous thromboembolism (e.g., pregnant women, oral contraceptive users).






1 thought on “EM@3AM: Mastoiditis”
Very useful thank you