Author: Anna Pickens, MD (@AnnaEMin5, Creator of EM in 5) // Edited by: Alex Koyfman, MD (@EMHighAK), Brit Long, MD (@long_brit), and Manpreet Singh, MD (@MprizzleER)
Welcome to this week’s edition of EM in 5 with Dr. Anna Pickens. Today we cover treatment of hypertensive emergencies, with a detailed look at medications. Enjoy the video!
Video
Hypertensive Urgency – High BP, but no end-organ damage
versus
Hypertensive Emergency:

OR

Acute CHF: Nitroglycerin and BiPaP. Avoid beta blockers.
Preeclampsia or Eclampsia: Magnesium 6 g load, labetalol, nicardipine, hydralazine. Delivery if still pregnant. Avoid Nitroglycerin.
ACS: Nitroglycerin. Avoid hydralazine. Morphine and beta blockers are controversial. We have better medications than these for HTN and analgesia, which should be avoided if possible.
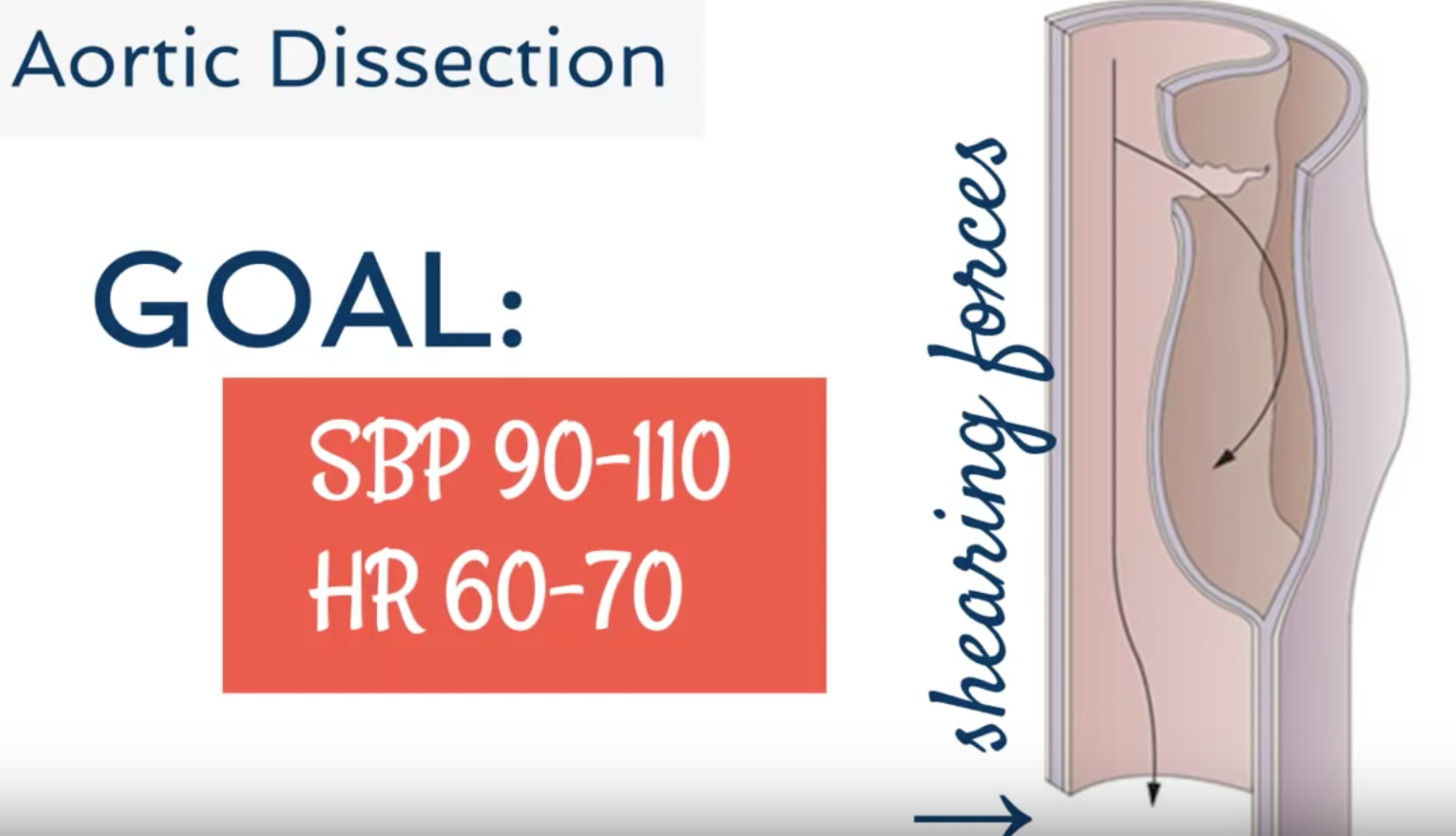
Aortic dissection: Treat heart rate first with esmolol/labetolol. Then treat blood pressure with nitroprusside or nicardipine. Pain control is essential.
Stroke: If hemorrhagic, goal SBP around 160 mm Hg. If ischemic and patient eligible for tPA, goal SBP is < 185 mm Hg. If not eligible, goal SBP is < 220 mm Hg. Options include labetalol or nicardipine. Avoid hydralazine.
Summary:

Suggested/Further Reading:
- Articles/Posts:
- Podcasts/Videos:




