
Author: Davin Brar, MD (EM Resident Physician, UT Southwestern, Dallas, TX) // Reviewed by: Alex Koyfman, MD (@EMHighAK) and Brit Long, MD (@long_brit)
Welcome to EM@3AM, an emDOCs series designed to foster your working knowledge by providing an expedited review of clinical basics. We’ll keep it short, while you keep that EM brain sharp.
A 66-year-old male presents via EMS in respiratory distress. For the past several days he has had worsening productive cough, chest pain, dyspnea, and fever. He appears fatigued, is sitting up in bed, and has increased work of breathing. On exam there is no JVD, 1+ edema, and crackles bilaterally. Vital signs include T 102.1 F, HR 110, RR 28, BP 94/62. Chest Xray is shown below.
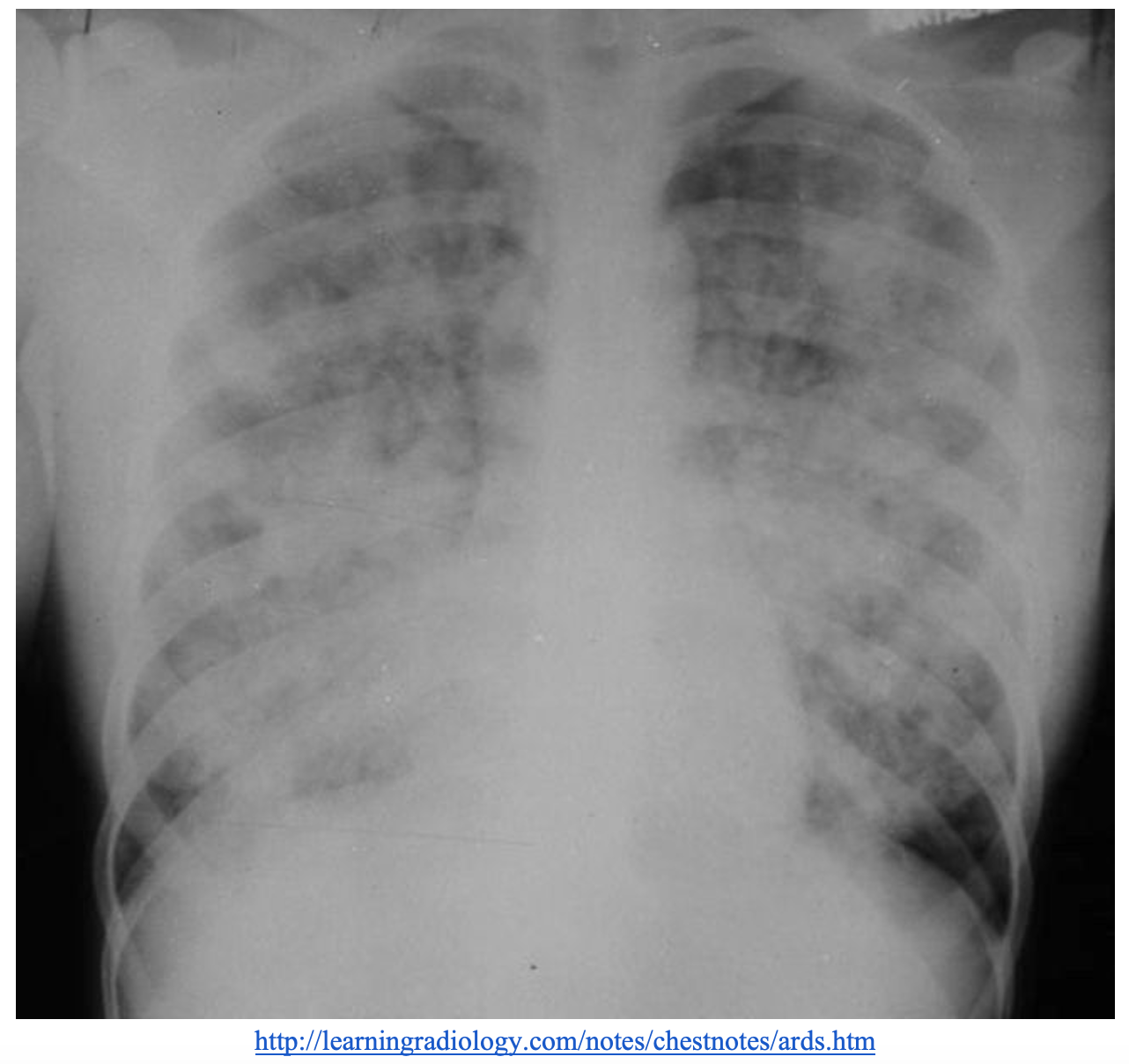
What is the likely diagnosis, and what’s the next step in your evaluation and treatment?
Answer: ARDS secondary to infection/sepsis
Background:
- ARDS is a complication of various different diseases and is associated with significant morbidity and mortality. Early recognition and treatment are essential.1
- ARDS is relatively common in ICU patients:10% of all admitted ICU patients and 23% of mechanically vented patients..2
- Patients who survive are high risk of cognitive decline, depression, PTSD, skeletal muscle weakness.1
- ARDS affects about 200,000 patients every year in the United States and about 3 million patients worldwide. 2
- Mortality from ARDS is high ranging from 35-45%.2
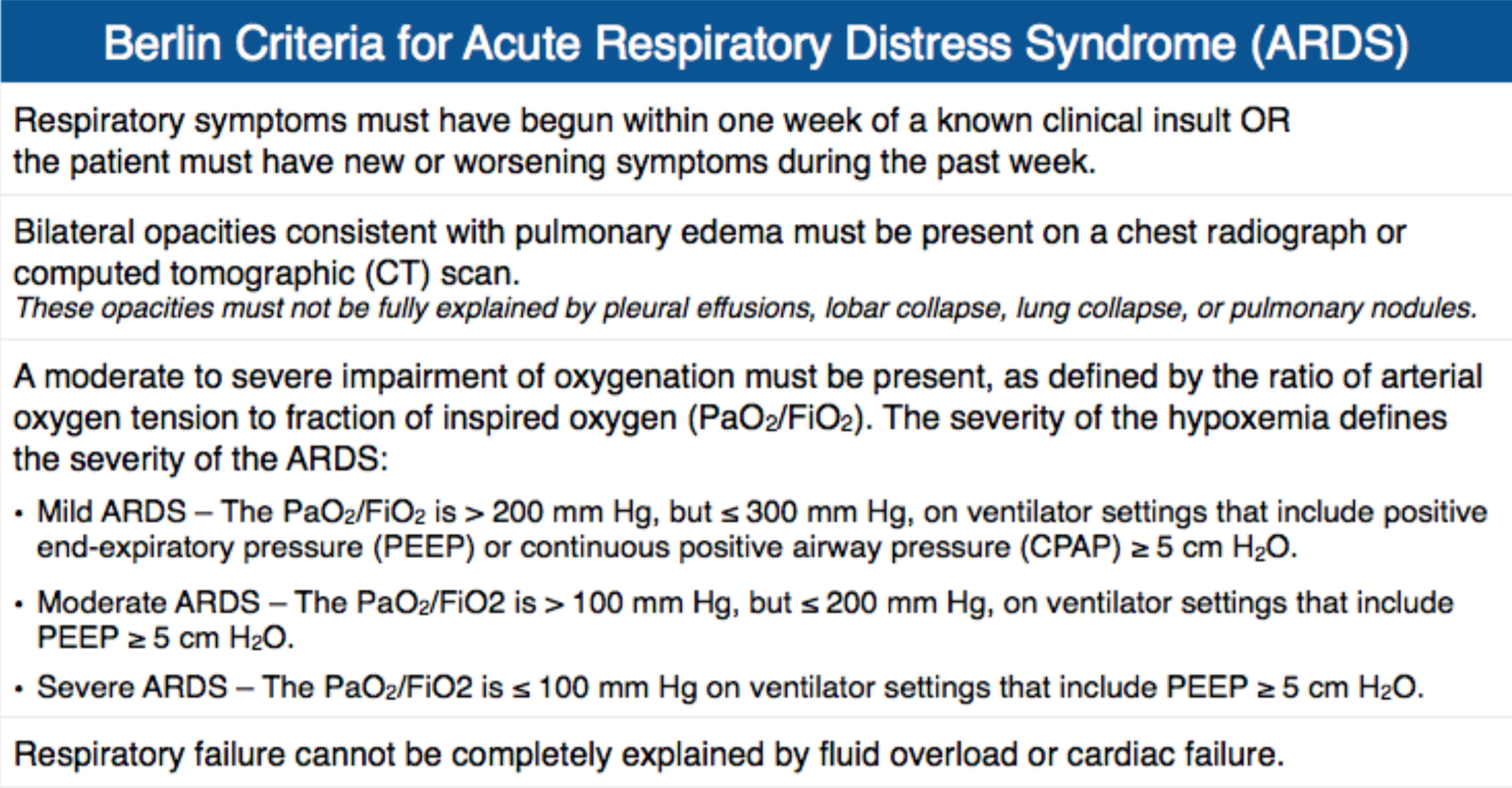
ARDS is defined by the Berlin Criteria3
- Presents within 1 week within clinical insult.
- Imaging findings include bilateral diffuse ground glass opacities.
- Findings not explained by cardiogenic pulmonary edema.
- PaO2/FiO2 ratio <300
Categories of ARDS3
- 3 mutually exclusive categories defined by PaO2/FiO2 ratios
- Mild (200-300)
- Moderate (100-200)
- Severe ( <100)
Pathogenesis:
- Lungs response to injury (3 phases) 2
- Exudative phase
- immune cell mediated damage of alveolar endothelial and epithelial barriers
- Protein rich edema within interstitium and alveoli
- Proinflammatory cytokines released by macrophages
- Proliferative (repair) phase
- Reabsorption of alveolar edema to restore normal alveolar architecture/function
- Fibrotic phase
- Final phase
- Not in all patients but is thought to be cause of prolonged ventilation in some patients.
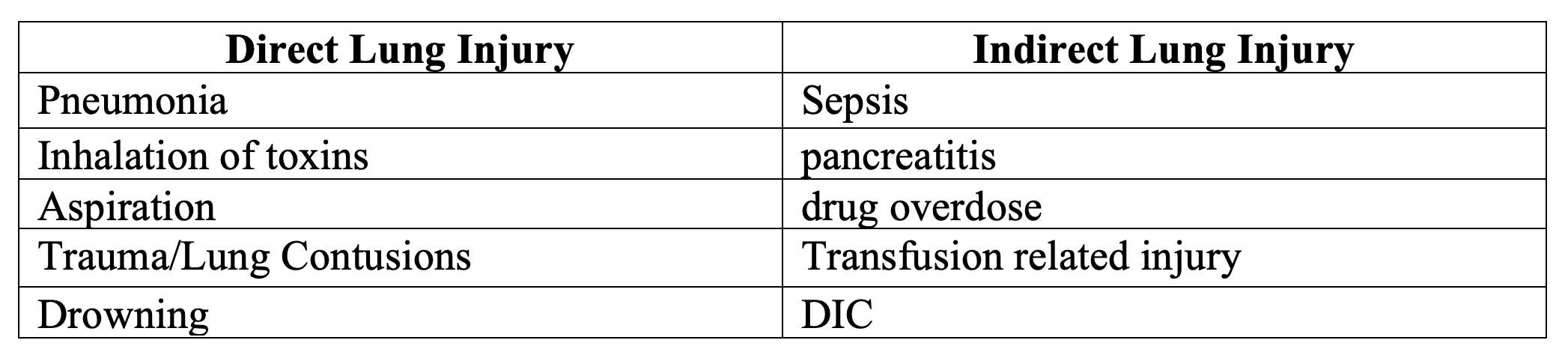
- Causes of ARDS1
- Exudative phase
History:
- Patients typically present in respiratory distress
- Hypoxic with bilateral pulmonary infiltrates
- Symptoms are typically acute in onset , usually within 7 days.
- Signs and symptoms of other disease entities:4
- Infection (pneumonia, aspiration)
- Sepsis
- Pulmonary contusions
- Drowning/ near drowning
- Pancreatitis
- Inhalation injuries
- Burns
- Overdose
- High altitude sickness
- Transfusion related injury
Exam:
- Patient with respiratory symptoms likely in respiratory distress
- Evaluating for volume overload (ie JVD, peripheral edema, S3 heart sound) can help differentiate heart failure from ARDS.
- Complete physical exam to assess for signs of infection or injury
- If intubated be sure to check and optimize patients vent settings to reduce lung injury.
Evaluation:
- Usually these are critically ill patients that require a broad work up
- There is no lab test that is diagnostic for ARDS. Instead, use Berlin criteria and assess for other pathologies.
- Arterial blood gas is helpful to calculate the PaO2/FiO2 ratio.
- Cultures (blood, urine) to investigate for a possible infectious source of concomitant sepsis.
- CBC, chemistries, lactate, inflammatory markers.
- Imaging should include chest x-ray; however, CT may also be obtained.
- Per Berlin Criteria: Bilateral opacities that are consistent with pulmonary edema on either chest x-ray or chest CT.
- These findings should not be fully explained by other causes such as heart failure, effusions, atelectasis, and masses.
- There can be heterogeneity in imaging.
- Point of care ultrasound (POCUS) is useful to assess for other causes of symptoms including decompensated heart failure
- POCUS views of the heart and lungs can evaluate for evidence of decreased ejection fraction, pericardial/pleural effusions, pulmonary edema, and consolidations which may be causing the patients symptoms.
Treatment
- Supportive treatment with focus on limiting further injury
- Treat the underlying cause (ie if you suspect infection give antibiotics)
- Patients may require mechanical ventilation. It is important to limit damage to lungs while patients are intubated.
- Lung protective vent settings
- Use low tidal volumes (6 mL/kg).5
- Use ideal body weight which is calculated by height (lung size doesn’t change with BMI).
- Patients are at risk for ventilator induced lung injury (VILI) due to over distention, repetitive opening/closing of lung units and translocation of proinflammatory mediators.2
- Consider that with low tidal volume vent settings patients may become hypercapnic causing a respiratory acidosis.
- This is known as “permissive hypercapnia”.
- No known upper limit for PCO2 levels, however, some studies suggest PCO2 of 60-70 mmHg and pH of 7.2-7.25 are safe for most patients.1
- Vent modes
- Volume control allows for precise control of the tidal volume patients receive.
- Airway pressure release ventilation (APRV) may improve oxygenation however it has not been shown to reduce mortality. It may be helpful for patients who are not tolerating the vent.5
- Keep Plateau pressures <30 cmH2) to avoid VILI.
- Recruitment maneuvers to improve oxygenation.9
- No high quality evidence.
- Sustained inflation: PEEP 30-40 held for 30 seconds.
- Staircase recruitment maneuver: increasing PEEP every 2 min to a peak of 55 then titrated back down.
- Consider proning in moderate to severe cases6
- Reduces ventilator associated lung injury
- Improved V/Q matching
- Usually used in patient with severe ARDS.6
- PaO2/FiO2 ratio < 150 mm Hg.
- FiO2 >0.6, PEEP >5, tidal volume 6mL/kg.
- Intubated and on ventilator for less than 36 hours.
- Proning can be resource intense requiring a team of trained staff or rotating mechanical beds.
- There is a risk tubes, lines and equipment can be dislodged during when the patient is being proned.
- Patients will spend most the day (usually 16 hours) in the prone position and the remainder of the day supine.
- Steroids
- Several studies on steroids in ARDS have shown benefit when steroids are given early.10
- May increase vent free days, reduce mortality, & decrease ICU length of stay.
- Dexamethasone was used in DEXA-ARDS trial.10
- ARDS patients with PaO2/FiO2 ratio <200.
- 20mg IV for 5 days then tapering down.
- Paralysis is controversial
- Theorized to help patient-ventilator synchrony which can reduce VILI.
- Older trials showed improved outcomes however in 2018 the ROSE trial did not find a reduction in mortality and was associated with some harm.11
- ECMO may be considered, but this is controversial. 7
- No clear evidence that ECMO reduces mortality.
- Trials looked at some of the sickest patients with ARDS.
- Recent trial looked at patients with PaO2/FiO2 ratios <80 & pH <7.25 and did not find a mortality reduction in patients who underwent ECMO12
- Lung protective vent settings
Disposition:
- ARDS patients are critically ill and require ICU admission.
Pearls:
- Patients with ARDs are some of the sickest we see in the ED. Timely recognition and intervention are essential.
- ARDS is not a primary disorder but instead secondary to other illnesses.
- Treatment is focused on supportive care and limiting lung injury.
- Use lung protective ventilation with low tidal volumes.

A 34-year-old woman presents to the emergency department with shortness of breath and worsening right flank pain. She has a history of nephrolithiasis and was diagnosed with a 6 mm stone almost 3 days ago. Her temperature is 39°C (102.2°F), pulse rate is 114 beats/min, respirations are 28/min, blood pressure is 105/70 mm Hg, and SaO2 is 89% on 4L NC. She has bilateral diffuse airspace opacities on the chest X-ray. Which of the following findings is most likely to be seen?
A) Decreased ejection fraction
B) Decreased ratio of PaO2 to FiO2
C) Increased NT-proBNP
D) Increased pulmonary capillary wedge pressure
Answer: B
Based on this patient’s abnormal vital signs and recent history of nephrolithiasis, it is likely she is now presenting with urosepsis as a result of a retained infected stone. The findings of hypoxemia and diffuse pulmonary infiltrates on chest X-ray is concerning for acute respiratory distress syndrome (ARDS). Radiographic findings are usually bilateral. The clinical picture, including age, lack of cardiac comorbidities, and the presence of fever, makes pulmonary edema from a cardiac etiology far less likely. Pulmonary edema is a salient feature in these cases, as a result of leaky alveolar-capillary membranes. ARDS can occur in a variety of conditions, such as sepsis, pneumonia, freebase cocaine smoking, trauma, toxic inhalation, radiation pneumonitis, and disseminated intravascular coagulation. Treating the underlying disease (e.g., antibiotics and urology evaluation) and supportive care with mechanical ventilation and vasopressor support are the mainstays of management. One of the required criteria in the Berlin definition of ARDS is moderate to severe impairment of oxygenation, as defined by the ratio of arterial oxygen tension to fraction of inspired oxygen. A decreased ratio of PaO2 to FiO2 is present in ARDS.
Decreased ejection fraction (A) is suggestive of decreased cardiac output in the context of heart failure. Congestive heart failure is unlikely to be driving the pulmonary edema in this case. Plasma BNP can be a useful surrogate marker for volume overload in cardiac dysfunction, where an increased NT-proBNP (C) would support a diagnosis of cardiogenic pulmonary edema. A pulmonary artery catheter can measure the pulmonary capillary wedge pressure, which can elucidate the etiology of pulmonary edema. Generally, cardiogenic pulmonary edema is more likely to have an increased pulmonary capillary wedge pressure (D).
Further Reading:
- Life in the fast lane “ARDS” https://litfl.com/acute-respiratory-distress-syndrome-ards/
- RebelEM “Lung Protective Mechanical Ventilation” https://rebelem.com/rebel-crit-cast-ep-4-0-lung-protective-mechanical-ventilation/
- RebelEM “Therapy options in Acute Respiratory Distress Syndrome” https://rebelem.com/salvage-therapies-in-acute-respiratory-distress-syndrome/
- PulmCrit: ARDS vs pseudoARDS https://emcrit.org/pulmcrit/pseudoards/
- EMCRIT podcast “The logistics of Proning for ARDS” https://emcrit.org/emcrit/logistics-proning/
- EmDOCs “Acute respiratory distress syndrome: who’s at risk and ED relevant management” http://www.emdocs.net/acute-respiratory-distress-syndrome-ards-whos-risk-ed-relevant-management/
- EMRA podcast “ARDS management ED and beyond https://www.emra.org/about-emra/publications/emra-cast/ards-management-ed-and-beyond/
- Core EM “The Benefit of Lung-Protective Ventilation in the ED” https://coreem.net/journal-reviews/lung-protective-vent/
- EMCRIT “Steroids for ARDS? The DEXA-ARDS trial” https://emcrit.org/pulmcrit/dexa-ards/
References
- “Chapter 23 Acute Respiratory Distress Syndrome.” Marino’s the ICU Book, by Paul L. Marino, Wolters Kluwer Health/Lippincott Williams & Wilkins, 2014, pp. 447–461.
- Thompson BT, Chambers RC, Liu KD. Acute Respiratory Distress Syndrome. N Engl J Med. 2017 Nov 9;377(19):1904-1905.
- ARDS Definition Task Force, Ranieri VM, Rubenfeld GD, Thompson BT, et al. Acute respiratory distress syndrome: the Berlin Definition. JAMA. 2012 Jun 20;307(23):2526-33.
- Nickson, Chris. “Acute Respiratory Distress Syndrome – ARDS • LITFL • CCC Ventilation.” Life in the Fast Lane • LITFL, 3 Nov. 2020, litfl.com/acute-respiratory-distress-syndrome-ards/.
- Acute Respiratory Distress Syndrome Network, Brower RG, Matthay MA, Morris A, Schoenfeld D, Thompson BT, Wheeler A. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med. 2000 May 4;342(18):1301-8.
- Guérin C, Reignier J, Richard JC, et al; PROSEVA Study Group. Prone positioning in severe acute respiratory distress syndrome. N Engl J Med. 2013 Jun 6;368(23):2159-68.
- Combes A, Hajage D, Capellier G, et al; EOLIA Trial Group, REVA, and ECMONet. Extracorporeal Membrane Oxygenation for Severe Acute Respiratory Distress Syndrome. N Engl J Med. 2018 May 24;378(21):1965-1975.
- Tintinalli, Judith E., et al. Tintinalli’s Emergency Medicine: a Comprehensive Study Guide. McGraw Hill Education, 2020.
- Poole O. Recruitment manoeuvres in acute respiratory distress syndrome: Little evidence for routine use. Can J Respir Ther. 2013;49(4):30-32.
- Villar J, Ferrando C, Martínez D, et al; dexamethasone in ARDS network. Dexamethasone treatment for the acute respiratory distress syndrome: a multicentre, randomised controlled trial. Lancet Respir Med. 2020 Mar;8(3):267-276. doi: 10.1016/S2213-2600(19)30417-5. Epub 2020 Feb 7. PMID: 32043986.
- National Heart, Lung, and Blood Institute PETAL Clinical Trials Network, Moss M, Huang DT, Brower RG, et al. Early Neuromuscular Blockade in the Acute Respiratory Distress Syndrome. N Engl J Med. 2019 May 23;380(21):1997-2008.
- Combes A, Hajage D, Capellier G, et al; EOLIA Trial Group, REVA, and ECMONet. Extracorporeal Membrane Oxygenation for Severe Acute Respiratory Distress Syndrome. N Engl J Med. 2018 May 24;378(21):1965-1975.




