
Authors: Amanda Dalpiaz, DO (EM Resident Physician, NSLIJ / Manhasset, NY); Jessica Army, MD (EM Attending Physician, Associate Program Director NS/LIJ, NY) // Sophia Görgens, MD (EM Resident Physician, Zucker-Northwell NS/LIJ, NY); Cassandra Mackey, MD (Assistant Professor of Emergency Medicine, UMass Chan Medical School); Alex Koyfman, MD (@EMHighAK); Brit Long, MD (@long_brit)
Welcome to EM@3AM, an emDOCs series designed to foster your working knowledge by providing an expedited review of clinical basics. We’ll keep it short, while you keep that EM brain sharp.
An 83-year-old female presents to the ED with dyspnea at rest following a syncopal episode. Patient reports she was out for a walk with her husband when she began to feel lightheaded, short of breath, and then fainted. Triage vitals include BP 88/50, HR 115, RR 24, O2 98%. ECG is without signs of acute ischemia. On exam, the patient appears slightly tachypneic, with rales noted at bilateral lungs. There is a systolic murmur along with 2+ pitting edema at the lower extremities. Cardiac POCUS shows grossly decreased left ventricular ejection fraction (LVEF) with a hyperechoic structure at the aortic valve.
What is the most likely diagnosis?
Answer: Aortic stenosis causing acute decompensated systolic and diastolic heart failure, and cardiogenic shock.
Epidemiology:
- Affects 2-3% of patients > 65 years old1-4
- 10% of patients > 80 years old2, 4
- High mortality rate within 2-3 years of symptom onset in untreated patients2, 5, 6
- About 25% mortality rate per year7
Etiology:
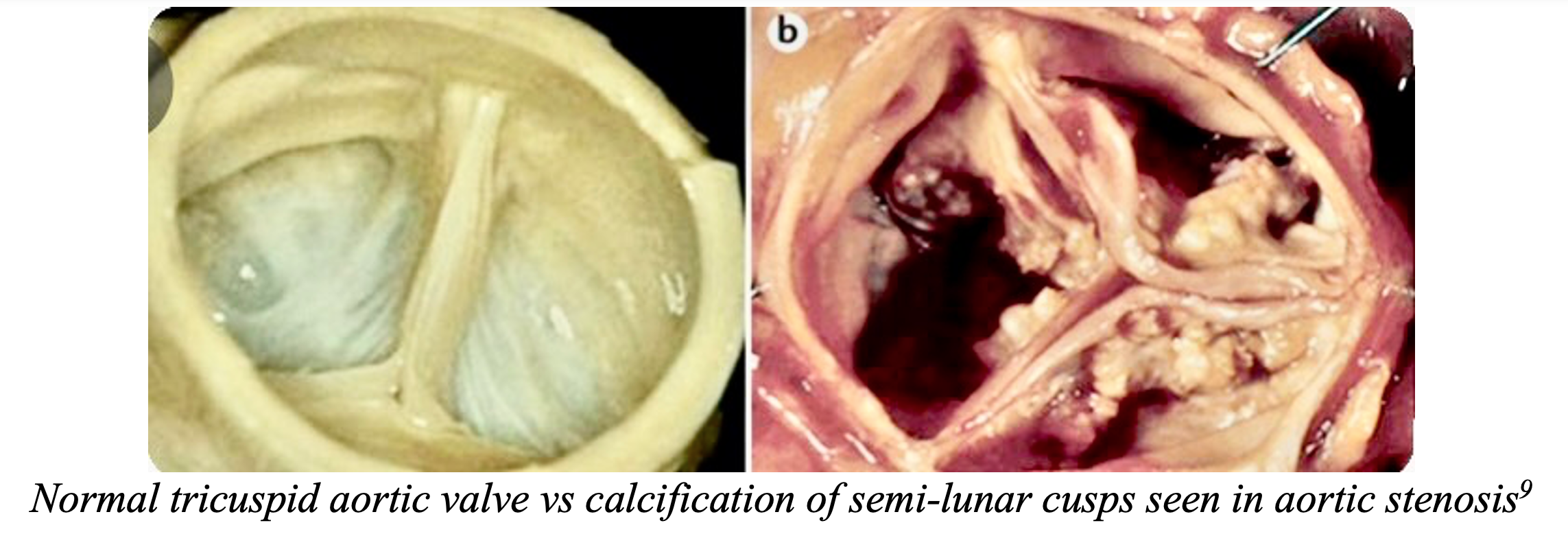
- Degenerative
- Tricuspid valve calcification due to aging (most common cause in developed countries)1, 5, 8
- Congenital bicuspid valve calcification (earlier symptom onset)1, 2, 5, 8
- Rheumatic Heart Disease
- Most common cause in developing countries1, 2, 5, 8
- Fusion of valve commissure 2, 5
- Usually with concomitant mitral valve stenosis8
- Other causes (less common): End stage renal disease, systemic lupus erythematosus, Fabry Disease, unicuspid valve5
Pathophysiology2:
- Narrow aortic valve opening => increased pressure gradient across valve => increased LV afterload
- Increased afterload => increased LV hypertrophy to maintain cardiac output
- LV hypertrophy decreases compliance => decreased filling => diastolic dysfunction & decreased stroke volume
- Decreased LV filling and decreased stroke volume => diastolic and/or systolic heart failure
- LV hypertrophy increases myocardial O2 demand and decreases coronary artery filling
Clinical Presentation:
- Asymptomatic during early part of disease; patients can go years without symptoms4, 5
- Later in disease => LV cannot overcome aortic outflow obstruction => develop symptoms2, 5
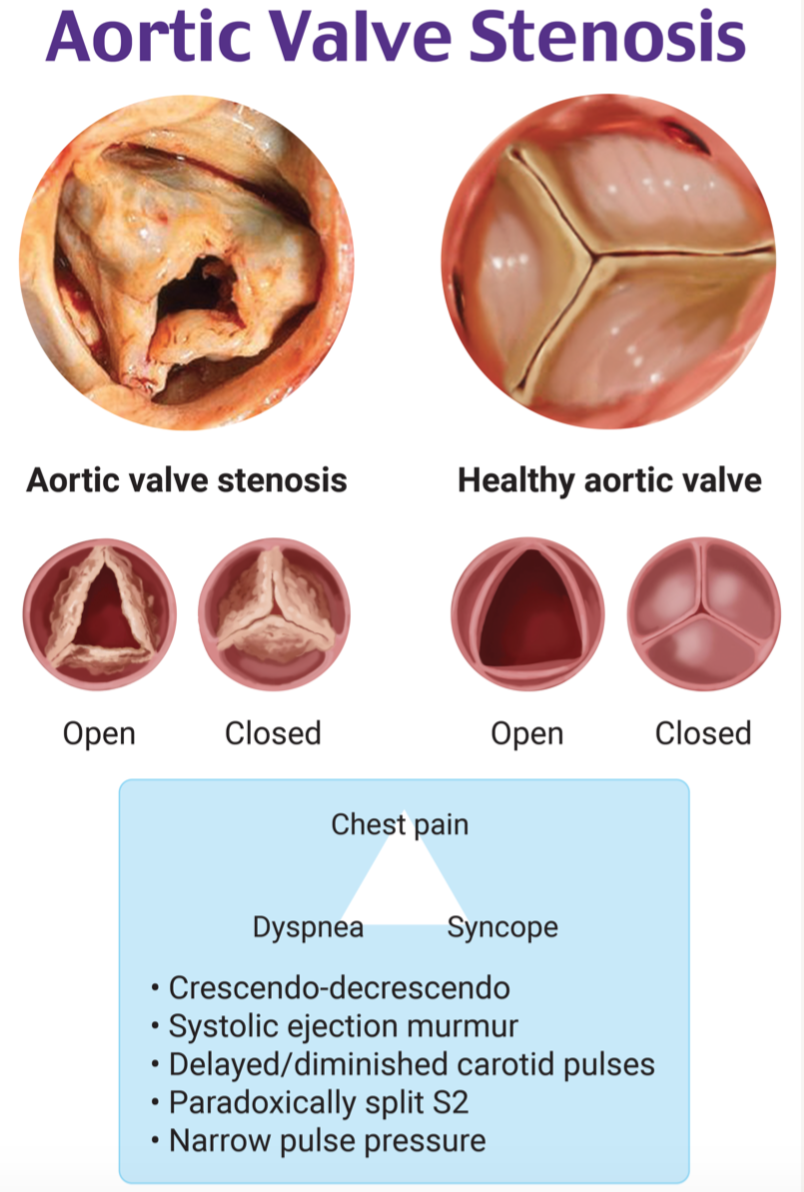
- Symptoms include angina, exertional syncope, dyspnea, fatigue2, 5, 8
Evaluation:
- Gold Standard: transthoracic echocardiogram (TTE)2, 3
- Severe stenosis criteria3
- Valve area < 1 cm1
- Peak velocity > 4 m/s
- Mean gradient 40 mmHg or more
- Qualitative POCUS can be helpful for hemodynamically unstable ED patient10
- Views: Parasternal long, parasternal short, apical 5 view4
- Assess aortic valve appearance4
- Presence/absence of calcification
- Leaflet mobility
- Assess LV size8
- LV wall hypertrophy
- Increased overall LV size compared to RV
- Estimate ejection fraction qualitatively via visualization 8
- Evaluate for decreased movement of mitral valve and decreased movement of LV wall during systole
- Severe stenosis criteria3
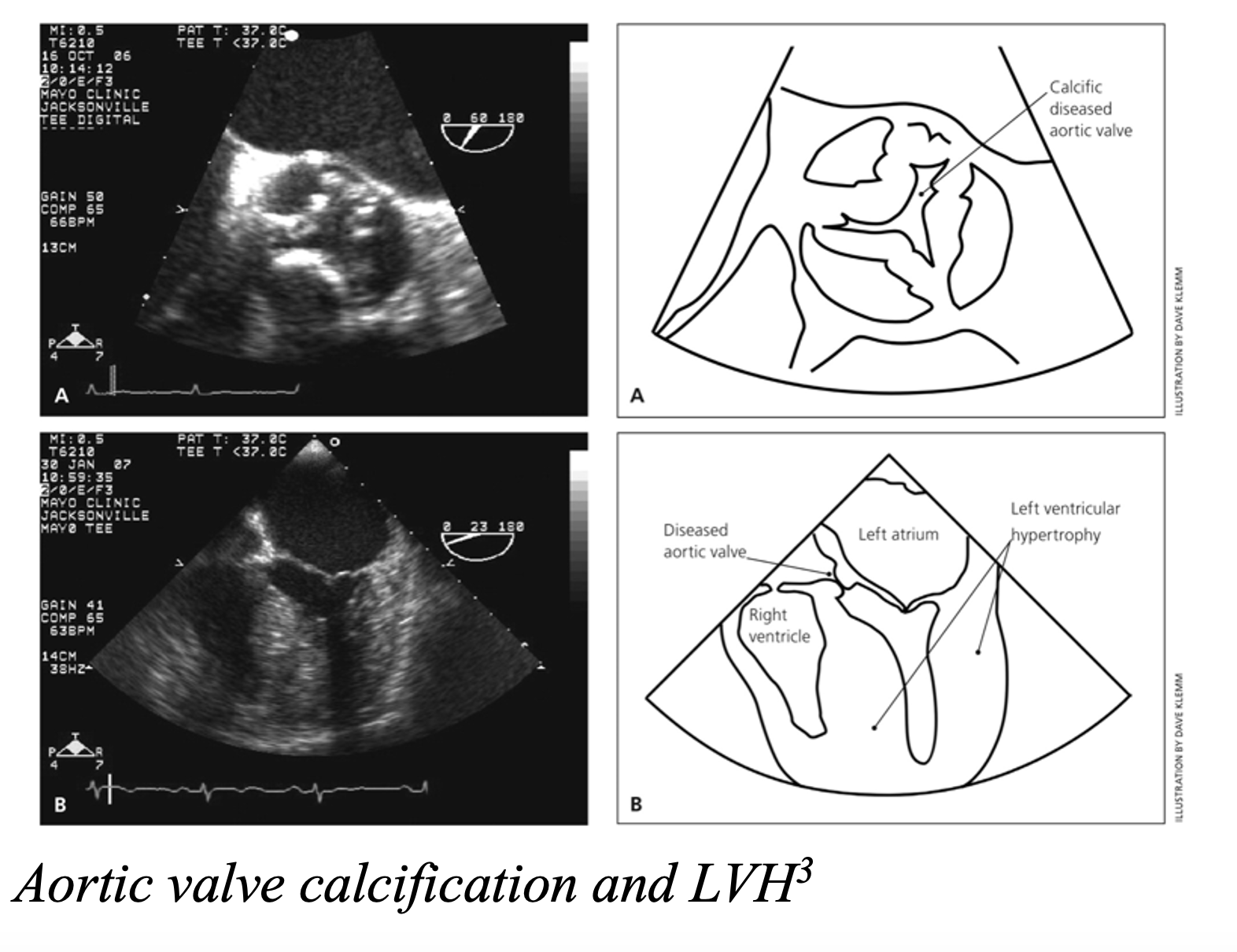
- ECG to evaluate for ischemia and LVH2
- CXR to evaluate for pulmonary edema, aortic valve calcification2
- Resuscitation and stabilization in the hemodynamically unstable patient:
- Hypotension2, 8
- Preload dependent and prone to pulmonary edema
- Administer IVF in small bolus with frequent reassessment of fluid status
- Vasopressors
- Phenylephrine is preferred (alpha1 receptor agonist)
- increases diastolic BP => increases coronary blood flow
- reflex bradycardia => increased diastolic filling
- Low LVEF => consider norepinephrine for inotropic effects (alpha1, alpha2, beta receptors)
- Avoid epinephrine => reflex tachycardia => decreased diastolic filling and increased O2 requirements of myocardium
- Phenylephrine is preferred (alpha1 receptor agonist)
- Preload dependent and prone to pulmonary edema
- Tachycardia
- Avoid beta-blockers and calcium channel blockers => decrease contractility2, 8
- Avoid epinephrine when choosing vasopressor2, 8
- Atrial fibrillation with RVR => loss of atrial kick + tachycardia => decreased diastolic filling => decreased preload3, 8
- Low threshold for cardioversion
- Severe decompensated CHF exacerbation2, 8
- Noninvasive ventilation (NIV)
- Diuretics (use with caution as patients are preload dependent)
- Nitrate use for afterload reduction is controversial due to preload reduction since aortic stenosis is preload dependent => consider cardiology consult
- Intubation2, 8
- Resuscitate before you intubate
- IV fluids
- Vasopressors
- Use induction agents with good hemodynamic profile
- Etomidate
- Ketamine
- Resuscitate before you intubate
- Hypotension2, 8
- Stabilizing/bridging measures for patients unable to undergo immediate valve replacement2
- Percutaneous aortic balloon dilatation
- Extracorporeal membrane oxygenation
- Definitive treatment: aortic valve replacement6, 11
- Surgical/open
- Low and intermediate risk surgical candidates1, 3
- TAVR (transcatheter aortic valve replacement)1, 3
- High risk surgical candidates
- Patients who are not surgical candidates
- Indications3
- Symptomatic severe aortic stenosis
- Asymptomatic severe aortic stenosis plus:
- Peak velocity > 5 m/s and mean pressure gradient > 60 mmHg
- LVEF < 50%
- Undergoing CABG or other heart surgery
- Abnormal stress test
- Surgical/open
Disposition:
- Symptomatic aortic stenosis2
- Unstable:
- Admit to ICU
- Consider emergent aortic balloon dilatation
- Valve replacement once stabilized
- Stable with worsening symptoms
- Admit to medicine with telemetry
- TTE
- Cardiology consult
- Evaluation for valve replacement
- Unstable:
Key Takeaways:
- Once symptomatic, aortic stenosis has high mortality rate if left untreated.
- Look for aortic valve calcification and decreased valve movement on POCUS.
- Patients with aortic stenosis are preload dependent.
- Optimize preload with small IVF boluses, reassessing fluid status, and avoiding/treating tachycardia.
- Definitive treatment is aortic valve replacement.

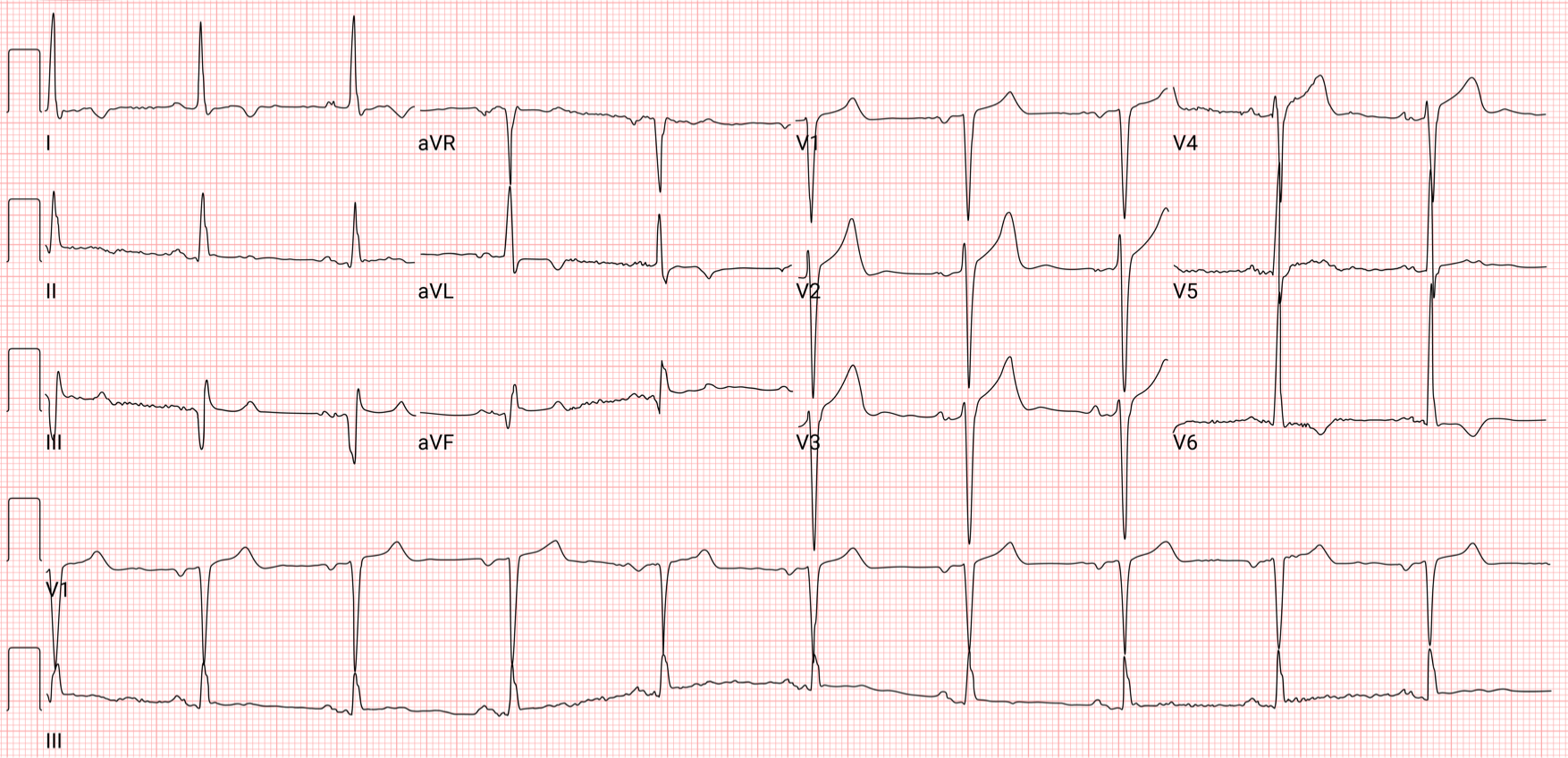
A 78-year-old man with a history of hypertension and diabetes presents to the emergency department after a syncopal episode. The patient reports that he has recently been experiencing shortness of breath when ambulating even short distances. He has also been having occasional episodes of chest pain with exertion. He was having some chest pain before the syncopal episode today, but it is now resolved. His BP is 140/110 mm Hg, HR is 75 bpm, RR is 18/min, and SpO2 is 95%. A cardiac exam reveals a normal rate and rhythm, a 3/6 systolic murmur radiating to the carotids bilaterally, and an S4 gallop. His ECG is shown above. A chest X-ray shows borderline cardiomegaly but no other findings. Which of the following is the most likely underlying cause of the patient’s symptoms?
A) Congenital heart disease
B) Coronary artery disease
C) Degenerative calcification
D) History of rheumatic heart disease
Answer: C
This patient presents with classic symptoms of aortic stenosis, the most common cause of which is degenerative calcification of the valve associated with aging, hypertension, hyperlipidemia, tobacco use, and diabetes. Aortic stenosis impairs left ventricular outflow, eventually resulting in left ventricular hypertrophy. Over time, cardiac output is diminished, and systemic blood flow and circulation to the coronary arteries are impaired. The classic triad of aortic stenosis is syncope, angina, and dyspnea. However, many patients with even severe stenosis may be asymptomatic. Syncope and heart failure are typically late-stage findings. A physical exam may reveal a systolic murmur at the right second intercostal space radiating to the carotids, a split S2, an S4 gallop, and a diminished carotid pulse with a delayed upstroke. An ECG may show left ventricular hypertrophy (as demonstrated above) and a left or right bundle branch block, but ECG is neither sensitive nor specific for aortic stenosis. Echocardiography confirms the diagnosis and can be used to grade the severity, with aortic valve area < 1.0 cm2 being considered severe stenosis. Patients with aortic stenosis are preload dependent. Therefore, medications that reduce preload, such as nitrates, diuretics, and vasodilators, should be used with extreme caution. Beta-blockers and calcium channel blockers are often not well tolerated due to their negative inotropic effects. Atrial fibrillation in patients with aortic stenosis can be particularly dangerous. Without effective atrial contraction, cardiac output can drop significantly, and cardioversion may be required. Surgical management is the primary treatment, as 40–50% of patients with classic symptoms will die within 1 year without surgical intervention.
Congenital heart disease (A) and bicuspid valves are often causes of aortic stenosis in younger patients. However, this patient’s age and risk factors are suggestive of degenerative calcification as the cause of his stenosis. Coronary artery disease (B) is not typically associated with the development of aortic stenosis. Papillary muscle rupture can occur as a complication of myocardial infarction, but this results in acute mitral valve regurgitation rather than aortic valve pathology. Rheumatic heart disease (D) is a common cause of aortic stenosis worldwide, but it is not the most common cause in the United States due to the widespread treatment of streptococcal infections.





{kind=link}