
A 15-year-old female with past medical history of polycystic ovarian syndrome, obesity, asthma, and recurrent otitis media with bilateral tympanostomy tube placement reports three weeks of increasing sanguineous drainage, ear pain, fevers to 101°F, and worsening left-sided headaches not improving with NSAIDs. She localizes the pain behind the left eye and additionally reports loss of lateral vision in her left eye, as well as double vision when looking to the left.
Vitals: T: 36.5 °C HR: 99 RR: 19 BP: 157/108 SpO2: 95% WT: 129.5 kg
On exam, she has a thickened, inflamed appearing left tympanic membrane with sanguinopurulent drainage from the left tympanostomy tube. She additionally has tenderness and swelling to the left mastoid process. Examination of the eyes reveals normal, symmetric, and reactive pupils. The patient has binocular horizontal diplopia on left lateral gaze and downgaze, which resolves with covering either eye. She has decreased vision in the lateral visual fields of the left eye on confrontational field exam.
The diagnosis of Gradenigo syndrome is made. What group of pathologies does this fall under?
Answer: Cranial nerve (CN) syndromes
Background:
To understand CN syndromes, a review of CN anatomy and physiology is in order (Figure 1, Table 1).
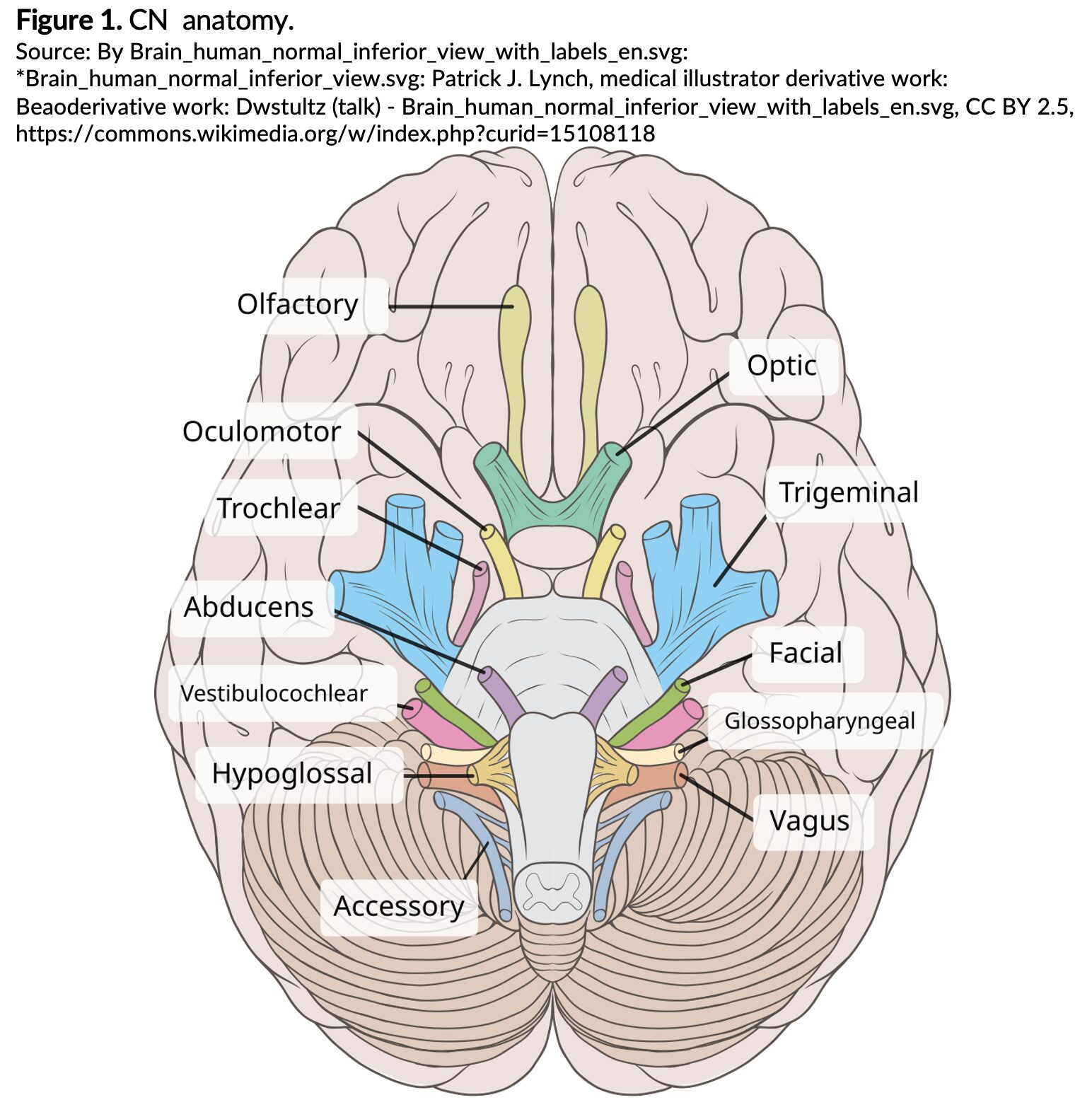
Table 1. Normal CN functions.4 Adapted from Table 1 of: Libreros-Jiménez HM, Manzo J, Rojas-Durán F, et al. On the Cranial Nerves. NeuroSci. 2023;5(1):8-38. doi:10.3390/neurosci5010002
| CN | Function |
| CN I Olfactory | Smell |
| CN II Optic | Vision |
| CN III Oculomotor | Ocular movements, pupil control, and elevation of the eyelids |
| CN IV Trochlear | Binocular vision coordination |
| CN V Trigeminal | Facial sensation; some facial motor function (mastication) |
| CN VI Abducens | Abduction of the eyes |
| CN VII Facial | Facial motor function, taste (anterior ⅔ of tongue) |
| CN VIII Vestibulocochlear | Balance, hearing |
| CN IX Glossopharyngeal | Taste, swallowing |
| CN X Vagus | Cardiac, digestive, respiratory, speech functions |
| CN XI Accessory | Movement of head/neck/shoulders |
| CN XII Hypoglossal | Tongue movement, speech |
Etiology:
The causes of CN palsies are many and are reviewed in Table 2.
Table 2. Potential etiologies of CN palsies.5
| Causes | Examples |
| Congenital/Developmental | Chiari malformation, hydrocephalus, IIH |
| Iatrogenic | CEA surgery, post-neurosurgery/ENT surgery, shunt malfunction/malpositioning |
| Idiopathic | IIH |
| Inflammatory | AIDP, Behcet’s syndrome, Guillain-Barré/Miller-Fischer syndrome, GCA, granulomatosis with polyangiitis, periarteritis nodosa, sarcoidosis |
| Infectious | Listeriosis, Lyme infection, meningitis, otitis media/mastoiditis/petrous apicitis, rhinosinusitis, skull base osteomyelitis, syphilis, TB, VZV |
| Musculoskeletal | Fibrous dysplasia, hyperostosis cranialis interna, osteopetrosis (Albers-Schonberg/marble bone disease), Paget’s disease |
| Neoplastic | CPA tumors, other intracranial masses (meningioma, lymphoma, etc.), Pancoast tumor, parotid gland tumor, pituitary apoplexy, vestibular schwannoma |
| Neurologic | Alzheimer’s, Graves’ disease, MS, Parkinson’s |
| Nutritional | Wernicke’s encephalopathy |
| Toxin induced | Aminoglycosides, botulism, chemotherapy, elapid snake bite, streptomycin |
| Trauma* | Increased ICP due to basilar skull fracture/intracranial hemorrhage, uncal/other herniation |
| Vascular | Aneurysm, AV malformations, carotid artery dissection, carotid-cavernous fistula, cavernous sinus thrombosis, microvascular/ischemia, PICA Syndrome, SAH, Wallenberg syndrome |
AV = arteriovenous, AIDP = acute inflammatory demyelinating polyneuropathy, CEA = carotid endarterectomy, CPA = cerebellopontine angle, ENT = ear, nose, and throat, GCA = giant cell arteritis, HTN = hypertension, ICP = intracranial pressure, IIH = idiopathic intracranial HTN, MS = multiple sclerosis, PICA = posterior inferior cerebellar artery, SAH = subarachnoid hemorrhage. TB = tuberculosis, VZV = varicella zoster virus. *Trauma is the most common cause of multiple cranial neuropathies.5,6
Epidemiology:
The incidence and etiologies of CN palsies are reviewed in Table 3.
Table 3. Incidence and etiologies of CN palsies.
| CN | Incidence n/100k/yr | Etiologies |
| CN I Olfactory2 | Prevalence estimated 5.6% in the general population, 16% of the elderly | Most commonly due to trauma or inflammation/infection from rhinosinusitis |
| CN II Optic2 | Unknown/unclear due to multiple etiologies | Graves orbitopathy, inflammatory conditions/MS, post-septal complications of rhinosinusitis/infection, pseudotumor cerebri/compressive lesions, traumatic optic neuropathy |
| CN III Oculomotor | Miller-Fischer syndrome 0.1/100,0007
Isolated/acquired all causes 4-6.62/100,0008 Age > 60 12.5/100,0009 |
Acute: Trauma (26%), compression due to uncal herniation or aneurysm (10%), stroke, cavernous sinus thrombosis (get venogram), iatrogenic (10%), infection (5%), Guillain-Barré syndrome (3%), idiopathic cavernous sinusitis (3%)
Chronic: Microvascular ischemia due to Diabetes (11%)/Hypertension (typically spares pupil), neoplasia (12%), congenital10
|
| CN IV Trochlear | 3.74-5.73/100,00010 | Congenital (49%), microvascular disease/hypertension (18%-32%), Trauma(18%-37%), Unknown (3%) brainstem CVA5,10 |
| CN V Trigeminal | Classic Trigeminal Neuralgia 4-13/100,000;11
poor epidemiologic data for other causes |
Trigeminal neuralgia: Nerve root compression within a few mm of the pons, usually due to an artery or a vein (the superior cerebellar artery is most common)11
Other: |
| CN VI Abducens | 8.4-11.3/100,0002,8
Wernicke’s: 0.4-2.8% of the population per autopsy study12 |
Most common nerve affected by intracranial hypertension due to a tumor or IIH13
Vascular disorders (35.9%), neoplasm (22.2%), congenital (6.8%), trauma (6.8%), cavernous sinus thrombosis(headache + CN palsy), Wernicke’s, infection (Gradenigo syndrome), demyelination2 |
| CN VII Facial | Isolated: 15-40/100,000
Bell’s Palsy: 11.5-53.5/100,0002 13-34/100,0007
Ramsay Hunt Syndrome: 5/100,000 |
Most common: Bell’s palsy, congenital, trauma2
Other: HSV/VZV, Ramsay Hunt, Lyme (bilateral Bell’s), pregnancy, immune reaction post vaccine (1 month), bacterial complication, malignant otitis externa/skull base osteomyelitis Central palsy: Stroke, MS, tumor7
|
| CN VIII Vestibulocochlear5
|
3.5-15.5/100,000 | Peripheral causes: vestibular neuritis, Meniere’s, BPPV(common), labyrinthitis
Central causes: brainstem/cerebellar/posterior circulation mass(CPA tumors)/CVA, vestibular migraine, acoustic neuroma, labyrinthine tumor2
Medications: aminoglycosides, streptomycin Behcet’s, Ramsay Hunt |
| CN IX Glossopharyngeal | Unknown incidence/rare | |
| CN X Vagus | Unknown incidence/rare | |
| CN XI Accessory | Unknown incidence/rare | |
| CN XII Hypoglossal | Unknown incidence/rare | |
| Multiple CNs: | ||
| Trauma14 | 4.3-17.6% of all traumatic head injuries have multiple CN | Most common isolated CN: VII
Most common multi-cranial neuropathy: III, IV, VI |
| Pituitary pathology15 | Adenoma 3.9-7.4/100,000 *most common intracranial tumor ~15% of population est. prevalence
Apoplexy 0.17-1.6/100,000 |
Can involve CN III, IV, VI due to proximity to the cavernous sinus. |
| Cavernous Sinus Syndrome5,14 | 0.2-1.3/100,000 est.
Cavernous Sinus Thrombosis 0.2-1.6/100,000 |
(CN III, IV, V1, V2, VI) Tumor (most common cause, including pituitary tumors), infectious, trauma, carotid cavernous fistulaCavernous sinus thrombosis is usually secondary to paranasal sinus infection, orbital cellulitis, or facial infection |
| Jugular Foramen Syndrome & Lower Cranial neuropathies16 | Unknown incidence/rare | Mass in retrostyloid parapharyngeal space must be ruled out
Lesion at the jugular foramen or retroparotid space, glomus tumors(paragangliomas) are a common cause of this syndrome, less common: schwannomas, meningiomas, metastases, retroparotid abscess, chordoma, thrombosis of jugular bulb
Cervical artery dissection
ICA dissections result in CN palsies in 7-12% of cases, most commonly CN XII is involved, presenting with tongue motor weakness; less common are CN IX, X, XI |
| Horner Syndrome17 | 2.95/100,000 adults | Ptosis, miosis, and anhidrosis; associated with Pancoast tumor |
CN = cranial nerve, IIH = idiopathic intracranial hypertension, MS = multiple sclerosis
Evaluation:2,5,7,18
The physical exam findings for cranial neuropathies can be subtle and overlap with other pathologies due to the many functions of the CNs. Still, a thorough neurologic exam can often cue the examiner into the specific nerve lesion and/or pathology.
- NEURO: A comprehensive CN exam, as well as evaluation of gait, reflexes, and cerebellar function, is important
- For example, the combination of ataxia, ophthalmoplegia, and areflexia is the triad associated with the Miller-Fischer variant of Guillain-Barré, and these three findings are used for clinical diagnosis
- HEAD: Presence of a ventriculoperitoneal shunt or craniotomy scar on examination of the scalp could help identify an iatrogenic cause of a CN palsy due to shunt complications, and indicate underlying pathology such as hydrocephalus
- EYES:
- Look for proptosis or papilledema that might indicate increased intracranial pressure (ICP), or Graves’ disease
- Ptosis, miosis, and myopia can all be CN-related or endocrinologic, such as myasthenia gravis
- Test visual fields and extraocular muscles for ophthalmoplegia.
- Signs of dendritic keratitis or endophthalmitis should raise suspicion for herpesvirus infection
- The presence of afferent pupillary defects, or a Marcus-Gunn or Argyll Robertson pupil, may also help to identify an inflammatory/infectious condition
- ENT:
- In a trauma, hemotympanum, raccoon eyes, or battle sign suggest intracranial injuries such as a basilar skull fracture that can increase the ICP as well as cause direct trauma to the CNs
- A bulging ear and tender mastoid process would indicate infectious etiologies secondary to otitis/mastoiditis and spread to the temporal bone (Gradenigo syndrome)
- Vesicular lesions on the ear may be Ramsay Hunt syndrome secondary to varicella zoster virus
- NECK: Thyromegaly or nodularity can be evaluated for suspicion of thyroid disease
- BREAST: A history of galactorrhea might indicate a pituitary prolactinoma
- SKIN:
- A port wine stain may indicate Sturge-Weber syndrome and the presence of arteriovenous malformations
- A bullseye rash is suggestive of Lyme, or a bite wound may help declare a snake bite injury
- Caput medusae, telangiectasias, or palmar erythema would guide a diagnosis related to alcohol use (Wernicke’s)
- CARDIOVASCULAR: Carotid bruit may be present in carotid stenosis or dissection
- MSK:
- If the patient is tilting their head to the side, it may be secondary to ocular torticollis, which can be congenital or may result from an acquired trochlear nerve palsy
- Bowed or deformed long bones could be a sign of Paget’s disease
Diagnosis:2,5
Diagnostic testing will vary primarily based on the underlying suspected etiology of the presenting cranial neuropathy. Some presentations require absolutely no laboratory evaluation; however, others do. For example, trigeminal neuralgia and Bell’s Palsy do not require more than a clinical diagnosis.
Labs:
- CBC, CMP, ESR, CRP
- Lumbar puncture (LP, urine, or blood cultures may be ordered if an infectious agent is suspected.
- LP is also useful to look for signs of Guillain-Barré syndrome or multiple sclerosis.
- Other tests to consider:
- Testing for suspected neurosyphilis
- HIV
- Thyroid function
- Vitamin B-12
- Folate levels may be ordered if indicated following a detailed history and examination
- Quantiferon Gold testing in suspected tuberculosis
- Serum/PCR vesicular lesions for VZV
Imaging:
- Studies to consider:
- Computed tomography (CT) or CT angiography
- MRI or MRV of head, orbits (optic neuropathy)
- MRI of the brain with/without contrast is generally considered the gold standard for evaluation of cranial neuropathies
- MRI is superior to CT in identifying marrow-space abnormalities such as edema or osteomyelitis, meningeal inflammation, extra-axial empyemas, and early cerebritis
- In general, if more than one CN is involved, MRI should be utilized in definitive diagnosis2
- There are a few exceptions in which advanced imaging is not required for diagnosis, but can be useful for treatment
- Isolated CN I palsy or typical Bell’s palsy2
- To distinguish between Bell’s and stroke pathology, the forehead is spared from facial droop in MCA ischemia/stroke7
- Classic trigeminal neuralgia2
- Isolated oculomotor nerve palsy (CN III, IV, VI) in patients over the age of 50 with atherosclerotic risk factors and intact pupillary function2
- Isolated CN I palsy or typical Bell’s palsy2
- MRI of the brain with/without contrast is generally considered the gold standard for evaluation of cranial neuropathies
Treatment:
A breakdown of common causes of cranial neuropathies and their treatments is shown in Table 4.
Table 4. Most common causes of cranial neuropathies and their treatment.
| Etiology | Treatment |
| Trauma ~12% of all multiple cranial neuropathy presentations5,6,14,20 | Possible neurosurgical consultation for fracture/increased ICP/intracranial hemorrhage
● HOB elevation 15-30 degrees, consider reverse Trendelenburg ● Maintain hemodynamic stability (fluids/vasopressors) to maintain cerebral perfusion pressure ● Osmotherapies: Hypertonic saline/mannitol in conjunction with neurosurgical consultation ● Seizure prophylaxis |
| Ischemic microvascular disease2 | Treat the chronic hypertension/atherosclerosis; the CN palsy typically self-resolves spontaneously within a few months |
| Wernicke’s21 | B1 (thiamine) 500mg IV or IM TID x 3 days initial, (parental route preferred due to poor absorption) continue 250 IV/IM additional 3-5 days or until clinical improvement ceases/plateaus |
| Bell’s Palsy22 | Initiate therapy within 72 hours of symptom onset when possible
● Steroid (prednisone 1mg/kg x 5 d) + antiviral (valacyclovir 1g TID x 5d or acyclovir 400mg 5x daily x 10 d) ● IV therapy is indicated for complications or immunocompromised patients ● Eye patch + artificial tears if unable to close eye to prevent corneal abrasion or keratitis ● Hearing protection ● ENT/ophthalmology follow-up |
| Trigeminal Neuralgia23 | Carbamazepine: first-line agent – Initial dose: 100mg 1-2x daily, may increase by 100-200mg every 3 days. Maintenance: 400-800mg daily. Monitor LFTs. Works within hours to days. Therapeutic serum level: 24-43 μmol/L, Can add Phenytoin 200-400mg/day if monotherapy is not adequate
Alternative therapies: oxcarbazepine, baclofen, lamotrigine, gabapentin, clonazepam, and valproic acid |
| Ramsay Hunt Syndrome24 | Primarily, CN VII *can also involve CN VIII, IX, X Same treatment as Bell’s palsy, but consider admission for severe vertigo, tinnitus, or hearing loss present, topical acyclovir to prevent herpes keratitis |
CN = cranial nerve, ENT = ear, nose, and throat, HOB = head of bed, IV = intravenous, LFT = liver function test.
Selected CN Palsies:
While there are a multitude of CN nerve palsies, the following are some of the less common but critical pathologies and their clinical presentations (Table 5). Note that CN I dysfunction is generally not evaluated in an emergency setting.
Table 5. Less common cranial neuropathies.
| CN Syndrome | Clinical Presentation | Evaluation | Diagnosis | Treatment |
|---|---|---|---|---|
| CN II Optic N palsy 2 | Blindness, hemianopia, quadrantanopia | Snellen / visual acuity
Ophthalmologic consultation |
CT head + CT orbits if infectious / traumatic concerns
If atrophy or signs of optic neuritis: MRI orbits with and without contrast |
Treat the underlying cause |
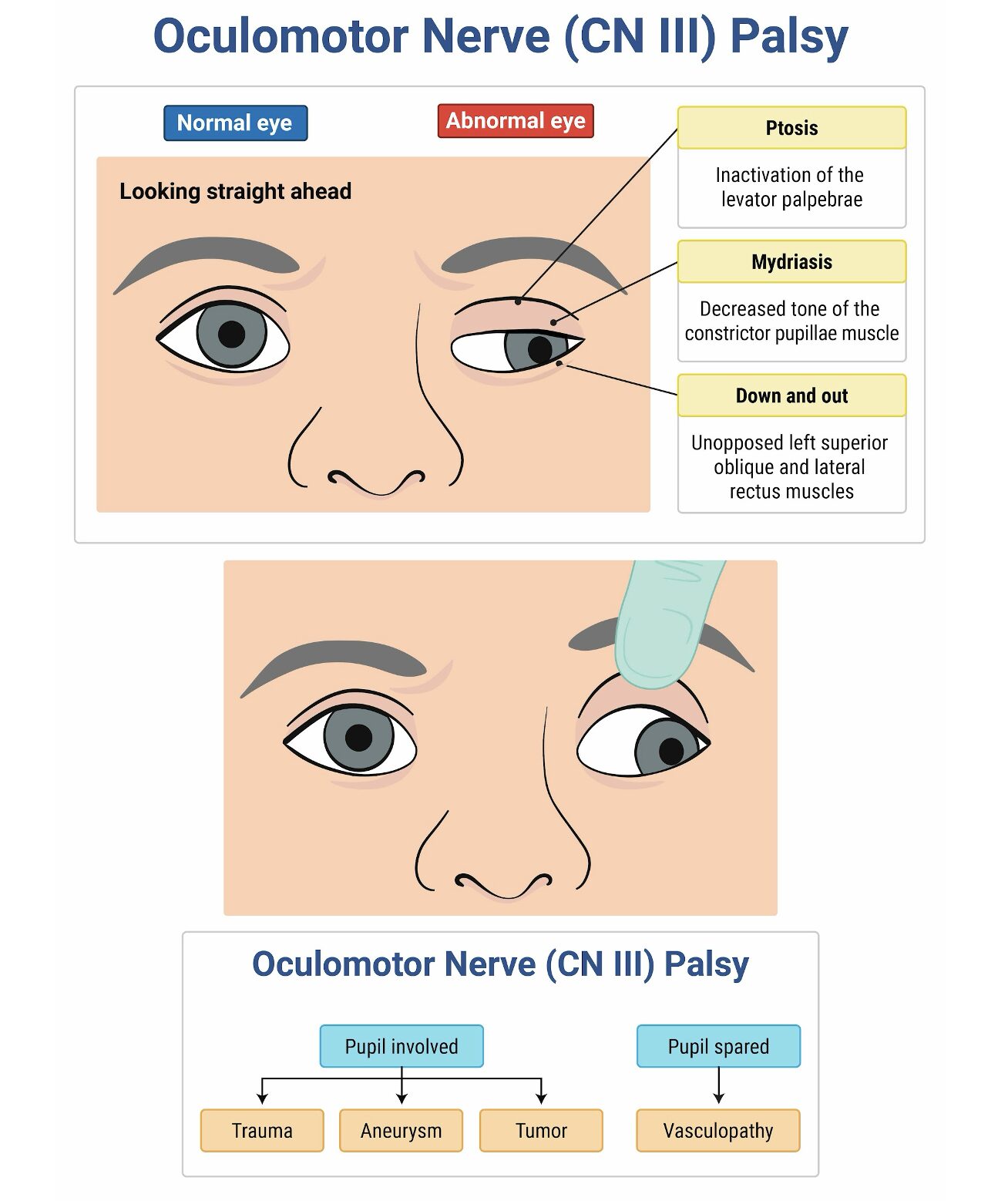
| CN III Oculomotor N palsy 2,6 | Diplopia, blurry vision, headache, photosensitivity
CN III palsy + thunderclap headache → rule out aneurysm CN III palsy + contralateral hemiparesis → consider Weber syndrome |
Complete palsy: ptosis, dilated unreactive or sluggish pupil, downward/outward gaze | Trauma (26%), compression due to uncal herniation or aneurysm (10%), stroke, CVST, iatrogenic (10%), infection (5%), GBS (3%), idiopathic cavernous sinusitis (3%)If ptosis, pupil involvement, or additional CN involvement: obtain non-contrast CT head and CTA head/neck to rule out PCA aneurysmIf no pupil involvement: CT head with and without contrast plus ischemic / infectious / inflammatory workup per clinical discretionIf >50 years with atherosclerotic risk factors, isolated CN III palsy, and no pupil involvement: imaging not recommendedIf CVST suspected: CTV or MRV |
Treat the underlying cause |
| CN IV Trochlear N palsy 2 | Vertical diplopia* | One iris sits higher than the other
Patient may tilt head to unaffected side (ocular torticollis) |
Clinical diagnosis
Rule out mimics (thyroid eye disease, MG) Multiple CN involvement requires further workup for mass, infection, or vascular lesion |
Treat the underlying cause
Symptomatic: prism glasses, patching, Botox, surgery |
| CN V Trigeminal N palsy 23 | Facial/oral pain or numbness in V1–V3 distribution
Neuropathic pain (“electric shocks”) lasting seconds to minutes ± spasms Triggered by chewing, temperature change, brushing teeth, touching face, talking Difficulty with mastication |
Sensory changes in CN V distribution
Facial spasms with severe pain, eye redness, tearing, rhinorrhea |
Clinical diagnosis; MRI may guide treatment | Carbamazepine first-line; monitor LFTs
Add phenytoin if inadequate response Alternatives: oxcarbazepine, baclofen, lamotrigine, gabapentin, clonazepam, valproic acid Refractory cases: surgery, nerve block, radiotherapy, rhizotomy |
| CN VI Abducens N palsy 2,5 | Isolated: diplopia, eye pain, dizziness, strabismus
Cavernous sinus syndrome: headache, diplopia, ophthalmoplegia, ptosis, proptosis, Gradenigo syndrome: otorrhea + V1 pain + CN VI palsy Wernicke’s: CN VI palsy, ataxia, AMS |
Inability to abduct affected eye; esotropia
Cavernous sinus syndrome may involve CN III, IV, V1, V2 |
MRI brain and orbits with contrast (preferred); CT with contrast if unavailable
LP if meningitis or IIH suspected ESR / CRP if GCA suspected |
Prism, patch, Botox, treat cause
Cavernous sinus thrombosis: anticoagulation Gradenigo: IV antibiotics, ENT/ID consult Wernicke’s: thiamine replacement |
| CN VII Facial N palsy 2,22,24 | Bell’s palsy: ear pain, facial numbness, hyperacusis, taste abnormality, decreased lacrimation, inability to close eye (must involve forehead)Ramsay Hunt: facial paralysis + otalgia + vesicular rash ± tinnitus, vertigo, hearing loss |
Bell’s: facial droop, loss of forehead wrinkles, flattened nasolabial fold, incomplete eye closure
Ramsay Hunt: facial paralysis with auricular or EAC vesicles |
Imaging not recommended for idiopathic Bell’s palsy within 72 hours
Inconsistent findings require CVA/infection workup Ramsay Hunt: VZV testing via serology, PCR, or CSF |
Bell’s: steroids + antivirals within 72 hours; eye protection
Ramsay Hunt: similar treatment; admit for severe vertigo or hearing loss |
| CN VIII Vestibulocochlear N palsy | Dizziness, ataxia, vertigo, nausea, vomiting, hearing changes, tinnitus | HINTS exam for AVS
Dix-Hallpike if BPPV suspected |
MRI IAC and brain with contrast preferred | Epley maneuver for BPPV
Vascular neurology consult for stroke ENT / neurosurgery consult for neoplasm |
| CN IX–XII palsies 2,5,18 | Vernet syndrome: CN IX–XI palsies
Collet-Sicard syndrome: CN IX–XII palsies Villaret syndrome: Collet-Sicard + Horner syndrome |
Hoarseness, loss of gag reflex, tongue and shoulder weakness | MRI preferred; CTA head/neck alternative | Treat the underlying cause |
AMS = altered mental status, AVS = acute vestibular syndrome, BPPV = benign paroxysmal positional vertigo, CN = cranial nerve, CRP = C-reactive protein, CSF = cerebrospinal fluid, CT = computed tomography, CTA = CT angiography, CVST = cerebral venous sinus thrombosis, ENT = ear/nose/throat, ESR = erythrocyte sedimentation rate, GBS = Guillain-Barré syndrome, IAC = internal auditory canal, IIH = idiopathic intracranial hypertension, LFT = liver function test, MG = myasthenia gravis, LP = lumbar puncture, MRI = magnetic resonance imaging, MRV = magnetic resonance venography, NSGY = neurosurgery, OM = otitis media, PCA = posterior communicating artery, PCR = polymerase chain reaction, TEVS = triggered episodic vestibular syndrome, TID = three times daily, TN = trigeminal neuralgia. *Patient cannot look down, read, or walk down stairs. **Forehead is spared in middle cerebral artery ischemia/stroke. ♱AVS = constant continuous dizziness, worrisome for central cause of dizziness.25 ♱♱TEVS = dizziness triggered by either change in position from supine to sitting or sitting to standing (i.e., orthostatic dizziness) or head movements (i.e., BPPV).25
Prognosis:
- There is a variable prognosis for cranial neuropathies due to the wide range in etiologies.
- Ranging from full recovery in weeks to months, to permanent deficits, the recovery depends on the underlying cause (trauma, tumor, inflammation, infection, diabetes, etc).
- Some etiologies resolve spontaneously without treatment.22
- Others, such as infections, tumors, trauma, or aneurysm need to be urgently addressed for better outcomes. In general, cranial neuropathies due to microvascular ischemia, infections, migraines, and inflammation have a better prognosis than tumors from certain cancers or severe trauma.2
- Microvascular/ischemic palsies typically self-resolve in 3-6 months2
- In traumatic cranial neuropathies, younger age and delayed onset of deficit are associated with better outcomes.26
- Oculomotor nerve palsies of all kinds generally have a good prognosis: Isolated 3rd nerve palsies of all kinds had 90% resolution at 6 months, 90% of 4th nerve palsy and 60% of 6th nerve palsies resolved by 9 months.27
- Wernicke’s Encephalopathy generally has poor prognosis with only 20% of patients fully recovering long-term.12
- Bell’s Palsy has a much better prognosis than Ramsay Hunt syndrome; 80-90% return to baseline within weeks to months, many within the first 3 weeks. Recovery rate improves with prompt treatment within 72 hours of onset.22
- Only an estimated 70% of Ramsay Hunt patients return to baseline; this is even lower for Ramsay Hunt with multineuropathies.28
Pearls:
- CN palsies involve a broad range of etiologies to keep on the differential.
- Advanced imaging is usually indicated, especially in the presence of multiple cranial neuropathies; however, a few CN presentations/syndromes can be identified clinically with a good history and thorough neurological exam.

A 60-year-old man presents to the emergency department with painless atraumatic diplopia. He has no known medical history and has never been to the doctor. The left eye is deviated inferiorly and laterally during frontward gaze. His pupillary exam is normal, and he has no extremity weakness. Which of the following is most likely to determine the etiology of his diplopia?
A) CT angiogram
B) Orbital CT
C) Serum glucose
D) Tonometry
Correct answer: C
The patient is exhibiting an oculomotor nerve (cranial nerve III) palsy. The oculomotor nerve innervates the levator palpebrae, superior rectus, medial rectus, and inferior rectus muscles that control the upper lid and extraocular movements. When an oculomotor nerve palsy exists, patients often present with ptosis and the classic “down and out” finding on examination, meaning the affected eye deviates inferiorly and laterally during normal frontward gaze. It is important to assess pupillary response, a differentiating feature when determining the etiology of oculomotor nerve palsy. A dilated pupil in the setting of an oculomotor palsy is a posterior communicating artery aneurysm until proven otherwise. On the other hand, if the pupil is spared and is reactive, the most likely cause is diabetes-related cranial nerve III mononeuropathy. Diabetes mellitus causes peripheral neuropathy due to nonenzymatic glycosylation of the nerves and vascular damage to the pupillomotor fibers within the nerve bundle. The oculomotor nerve is the most commonly affected cranial nerve from long-standing hyperglycemia. Therefore, in this patient with a normal pupillary exam, a serum glucose is most likely to determine the etiology of the palsy.
While a CT angiogram (A) is indicated in patients presenting with a new cranial nerve III palsy, a normal pupillary exam makes an aneurysm less likely in this patient.
An orbital CT (B) is of little utility in the evaluation of cranial nerve III palsy in the absence of trauma.
Increased intraocular pressure may be a cause of ophthalmoplegia. Conditions that lead to oculomotor palsies in the setting of raised intraocular pressure, such as retrobulbar hematoma, orbital cellulitis, or acute angle closure glaucoma, often present with pain. Because this patient is pain-free, tonometry (D) is not likely to be diagnostic in this case.
Further Reading
Further FOAMed:
- https://www.emdocs.net/em3am-oculomotor-nerve-palsy/
- https://wikem.org/wiki/Fourth_nerve_palsy
- https://www.emdocs.net/cavernous-sinus-thrombosis/
- https://www.emdocs.net/evaluation-dizzy-patient/
- https://www.saem.org/publications/grace/grace-3
- https://www.emdocs.net/bells-palsy-pearls-and-pitfalls-in-evaluation-and-management/
- https://www.emdocs.net/diplopia-evaluation-and-management/
- https://www.ahajournals.org/doi/full/10.1161/STR.0000000000000456?rfr_dat=cr_pub++0pubmed&url_ver=Z39.88-2003&rfr_id=ori%3Arid%3Acrossref.org
- https://litfl.com/thiamine-deficiency/
References:
- Bano S, Nawaz A, Asmar A, Aemaz Ur Rehman M, Farooq H, Ali H. Gradenigo’s syndrome presenting as IX and X cranial nerve palsy without clinically apparent ear infection: A case report and review of literature. eNeurologicalSci. 2022;27:100397. doi:10.1016/j.ensci.2022.100397
- Khaku A, Patel V, Zacharia T, Goldenberg D, McGinn J. Guidelines for Radiographic Imaging of Cranial Neuropathies. Ear Nose Throat J. 2017;96(10-11):E23-E39. doi:10.1177/0145561317096010-1106
- Kong SK, Lee IW, Goh EK, Park SE. Acute otitis media–induced petrous apicitis presenting as the Gradenigo syndrome: successfully treated by ventilation tube insertion. Am J Otolaryngol. 2011;32(5):445-447. doi:10.1016/j.amjoto.2010.07.018
- Libreros-Jiménez HM, Manzo J, Rojas-Durán F, et al. On the Cranial Nerves. NeuroSci. 2023;5(1):8-38. doi:10.3390/neurosci5010002
- Carroll C, Campbell W. Multiple Cranial Neuropathies. Semin Neurol. 2009;29(01):053-065. doi:10.1055/s-0028-1124023
- Keane JR. Third Nerve Palsy: Analysis of 1400 Personally-examined Inpatients. Can J Neurol Sci J Can Sci Neurol. 2010;37(5):662-670. doi:10.1017/S0317167100010866
- Chojdak-Łukasiewicz J, Paradowski B. Facial Asymmetry: A Narrative Review of the Most Common Neurological Causes. Symmetry. 2022;14(4):737. doi:10.3390/sym14040737
- Miyata M, Kido A, Miyake M, et al. Lifetime risk, sex and age differences in annual incidence of ocular motor cranial nerve palsy in Japan for 2019. Commun Med. 2025;5(1):299. doi:10.1038/s43856-025-01027-x
- Fang C, Leavitt JA, Hodge DO, Holmes JM, Mohney BG, Chen JJ. Incidence and Etiologies of Acquired Third Nerve Palsy Using a Population-Based Method. JAMA Ophthalmol. 2017;135(1):23. doi:10.1001/jamaophthalmol.2016.4456
- Dosunmu EO, Hatt SR, Leske DA, Hodge DO, Holmes JM. Incidence and Etiology of Presumed Fourth Cranial Nerve Palsy: A Population-based Study. Am J Ophthalmol. 2018;185:110-114. doi:10.1016/j.ajo.2017.10.019
- Yadav Y, Nishtha Y, Sonjjay P, Vijay P, Shailendra R, Yatin K. Trigeminal neuralgia. Asian J Neurosurg. 2017;12(04):585-597. doi:10.4103/ajns.AJNS_67_14
- Harper C, Gold J, Rodriguez M, Perdices M. The prevalence of the Wernicke-Korsakoff syndrome in Sydney, Australia: a prospective necropsy study. J Neurol Neurosurg Psychiatry. 1989;52(2):282-285. doi:10.1136/jnnp.52.2.282
- Gluckstein J, Prasad S. Infectious ocular motor neuropathies. Curr Opin Ophthalmol. 2019;30(6):454-461. doi:10.1097/ICU.0000000000000615
- Lim HL, Lim JX, Bakthavachalam R, Ker RXJ. Traumatic cavernous sinus syndrome – A peculiar presentation of multiple cranial nerve neuropathies following a minor head injury: Case report and literature review. J Clin Neurosci. 2024;119:180-184. doi:10.1016/j.jocn.2023.12.008
- Daly AF, Beckers A. The Epidemiology of Pituitary Adenomas. Endocrinol Metab Clin North Am. 2020;49(3):347-355. doi:10.1016/j.ecl.2020.04.002
- English SW, Passe TJ, Lindell EP, Klaas JP. Multiple cranial neuropathies as a presentation of spontaneous internal carotid artery dissection: A case report and literature review. J Clin Neurosci. 2018;50:129-131. doi:10.1016/j.jocn.2018.01.056
- Han J, Park SY, Lee JY. Nationwide population-based incidence and etiologies of pediatric and adult Horner syndrome. J Neurol. 2021;268(4):1276-1283. doi:10.1007/s00415-020-10270-2
- Soldatos T, Batra K, Blitz AM, Chhabra A. Lower Cranial Nerves. Neuroimaging Clin N Am. 2014;24(1):35-47. doi:10.1016/j.nic.2013.03.022
- Romano N, Federici M, Castaldi A. Imaging of cranial nerves: a pictorial overview. Insights Imaging. 2019;10(1):33. doi:10.1186/s13244-019-0719-5
- ACS Trauma Programs. Best Practices Guidelines The Management Of Traumatic Brain Injury. Published online 2024. https://www.facs.org/media/vgfgjpfk/best-practices-guidelines-traumatic-brain-injury.pdf
- Galvin R, Bråthen G, Ivashynka A, et al. EFNS guidelines for diagnosis, therapy and prevention of Wernicke encephalopathy. Eur J Neurol. 2010;17(12):1408-1418. doi:10.1111/j.1468-1331.2010.03153.x
- Dalrymple SN, Row JH, Gazewood JD. Bell’s Palsy. Prim Care. 2025;52(1):111-121. doi:10.1016/j.pop.2024.09.012
- Allam AK, Sharma H, Larkin MB, Viswanathan A. Trigeminal Neuralgia: Diagnosis and Treatment. Neurol Clin. 2023;41(1):107-121. doi:10.1016/j.ncl.2022.09.001
- Ananthapadmanabhan S, Soodin D, Sritharan N, Sivapathasingam V. Ramsay Hunt syndrome with multiple cranial neuropathy: a literature review. Eur Arch Otorhinolaryngol. 2022;279(5):2239-2244. doi:10.1007/s00405-021-07136-2
- Edlow JA, Carpenter C, Akhter M, et al. Guidelines for reasonable and appropriate care in the emergency department 3 ( GRACE ‐3): Acute dizziness and vertigo in the emergency department. Acad Emerg Med. 2023;30(5):442-486. doi:10.1111/acem.14728
- Basheer N, Varghese JC, Kuruvilla R, Alappat JP, Mathew J. A Prospective Study on the Incidence and Outcome of Cranial Nerve Injuries in Patients with Traumatic Brain Injuries. Indian J Neurotrauma. 2021;18(01):45-50. doi:10.1055/s-0041-1724141
- Akagi T, Miyamoto K, Kashii S, Yoshimura N. Cause and prognosis of neurologically isolated third, fourth, or sixth cranial nerve dysfunction in cases of oculomotor palsy. Jpn J Ophthalmol. 2008;52(1):32-35. doi:10.1007/s10384-007-0489-3
- Shim HJ, Jung H, Park DC, Lee JH, Yeo SG. Ramsay Hunt syndrome with multicranial nerve involvement. Acta Otolaryngol (Stockh). 2011;131(2):210-215. doi:10.3109/00016489.2010.520167





