Authors: Andrew Lin, MD (Emergency Medicine Resident, Johns Hopkins Emergency Medicine) and Drew Clare, MD (Attending Physician, Johns Hopkins Emergency Medicine) // Edited by: Alex Koyfman, MD (@EMHighAK) and Brit Long, MD (@long_brit)
Case
Picture this: you’re in the Emergency Department, nearing the end of your shift, when you’re called to see an eye complaint. It sounds like a typical low-acuity eye complaint: this 57-year-old patient presents with a vague chief complaint of having difficulty focusing on distant objects. She notices it has been present for a number of days and notes no other pertinent complaints. She has a history of hypertension and diabetes and has otherwise had no health issues. She sees her doctor regularly. You do your due diligence and perform a thorough review of systems – asking about headache, weakness, and hearing loss. You ask about diplopia, and to your surprise, the patient mentions that she has noticed that she does intermittently see double – especially when she is looking in certain directions.
Now what?
Diplopia is most often taught as a red flag during the comprehensive workup of many of our most common chief complaints – generalized weakness, headache, and almost any kind of visual complaint. This is with good reason, as diplopia can often be the herald symptom for many debilitating conditions that we are tasked with diagnosing in the emergency department. It is critical for the emergency physician to evaluate this finding thoughtfully and thoroughly to rule out serious pathology. A straightforward way to break down the etiology of diplopia is to first characterize the finding into either monocular diplopia or binocular diplopia, which is the first step in your evaluation. This is determined by having the patient cover each individual eye to see if the diplopia persists. If the diplopia persists when only the unaffected eye is covered, but resolves when only the affected eye is covered, this is monocular diplopia. If the diplopia resolves when either eye is covered, this is binocular diplopia. Monocular diplopia often occurs because of an abnormality in the affected eye itself. This is often due to refractive error, though CNS pathology and retinal disease are also possibilities. [1] Binocular diplopia, on the other hand, is often due to neuromuscular dysfunction causing misalignment of visual fields. Causes commonly include cranial nerve palsy, ocular muscle dysfunction, or brainstem pathology. Ergo, monocular diplopia can be appropriately managed with an ophthalmological referral and typically does not require neuroimaging. Binocular diplopia, on the other hand, requires further evaluation in the emergency department to rule out acute neurological insult.
Your next step is to determine if the diplopia is isolated or associated with neurologic signs/symptoms. In better building our differential and subsequent workup, the most important part of evaluation is thus a comprehensive neurological exam. The presence or absence of additional neurological symptoms and/or findings in addition to diplopia (vertigo, ataxia, motor or sensory deficits, or bulbar symptoms such as dysphagia or dysarthria) should prompt expedited neuroimaging and consultation with neurology for evaluation for stroke [2]. For example, if the patient presents with diplopia and a thorough neurological exam suggests anything beyond an isolated nerve palsy (of the extraocular muscles – 3, 4, and 6), activation of the stroke protocol should be the first step. Neuroimaging is needed, preferably MRI to evaluate for early signs of stroke and investigate the posterior circulation.
Beyond this crucial branch path in our evaluation of diplopia, our next task lies with localizing the lesion that best explains the diplopia and evaluating for obvious abnormality in ocular motility. Careful evaluation of 3rd and 6th nerve palsies is necessary. Testing the extraocular muscles is a critical step in evaluating where the problem may lie; the physician can often reproduce the diplopia by asking the patient to look in both vertical and horizontal directions. This can help you identify which nerve (or extraocular muscle) is abnormal and serves as the basis of the rest of our workup. In addition to extraocular movements, attention should also be paid to the eye itself, particularly the pupils. A schematic below reviews stereotypical findings for extraocular palsies [3]:
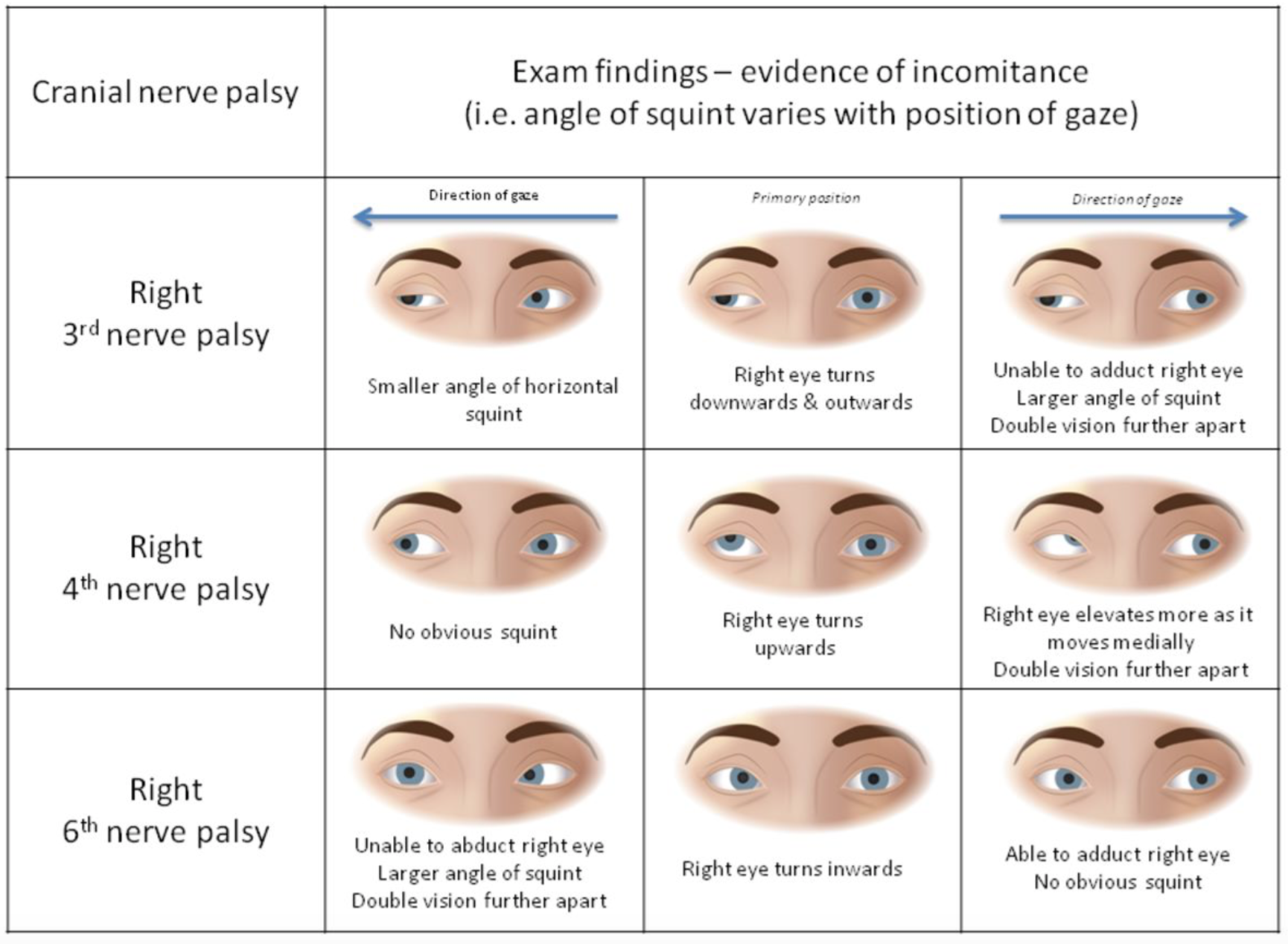
Physical exam findings of various palsies; image courtesy of the BMJ
At this point, one has identified exactly what neurological deficits our patient has, paying close attention to cranial nerves 3 and 6. This will guide further management.
Isolated nerve palsies are the most common cause of diplopia and are typically caused by microvascular insult. This ischemia leads to dysfunction of the extraocular muscles, which causes a gaze palsy. These patients often have many risk factors for vascular disease and require further risk factor modification, but they typically do not require acute therapeutic or imaging. However, the diagnosis of binocular diplopia secondary to microvascular pathology is one of exclusion: there are a myriad of conditions the emergency physician needs to consider. Ultimately, the need for neuroimaging in diplopia will depend on the palsy in question as well as the presence of other abnormalities in the exam or history.
First and foremost, if there is any suspicion of trauma in the history, imaging should be ordered for further evaluation. Direct trauma to the orbit (including the surrounding muscles and nerves) or involvement of the orbital apex (a space posterior to the orbit where CN 3, 4, 6 pass) is worrisome. An orbital floor fracture causing entrapment of extraocular muscles or a retrobulbar hematoma are also possibilities that warrant further imaging. A CT of the head and orbits is appropriate in this setting to rule out structural abnormalities. Contrast should be included if infection is suspected.
Second, an isolated third nerve palsy should always be further imaged with a non-contrast head CT as well as a CTA. While third nerve palsies are often caused by ischemia, approximately 6% of third nerve palsies are caused by a compressive aneurysm. This is often at the junction of the posterior communicating artery and internal carotid artery [3]. Traditionally it was thought that clinical exam could distinguish between a compressive and ischemic etiology. The fibers responsible for constriction of the pupil run on the outer portion of the nerve. An ischemic insult, affecting the central portion of the nerve, would therefore spare pupil constriction. External compression from an aneurysm on the other hand directly impacts the peripheral portion of the nerve, which is responsible for pupillary constriction. Clinical exam is not sufficient, however, as a large population study found that almost 36% of compressive third nerve palsies were found to be pupil-sparing. This supports the need for CT and CTA of the head in any presentation of third nerve palsy [4]. Palsies of the 4th and 6th cranial nerves, in the absence of any other additional concerning findings (especially focal neurological deficits), can be referred to neurology without further imaging. Both 4th and 6th nerve palsies are largely micro-vascular in etiology, which support no need for further evaluation. A few caveats: 6th nerve palsies, by virtue of their anatomic location, have a tendency to be associated with increased intracranial pressure, necessitating a good funduscopic exam to evaluate for papilledema. Additionally, the prevalence of malignancy over microvascular disease in children suggest that even in isolated 6th nerve palsies, children should always receive emergent imaging [5].
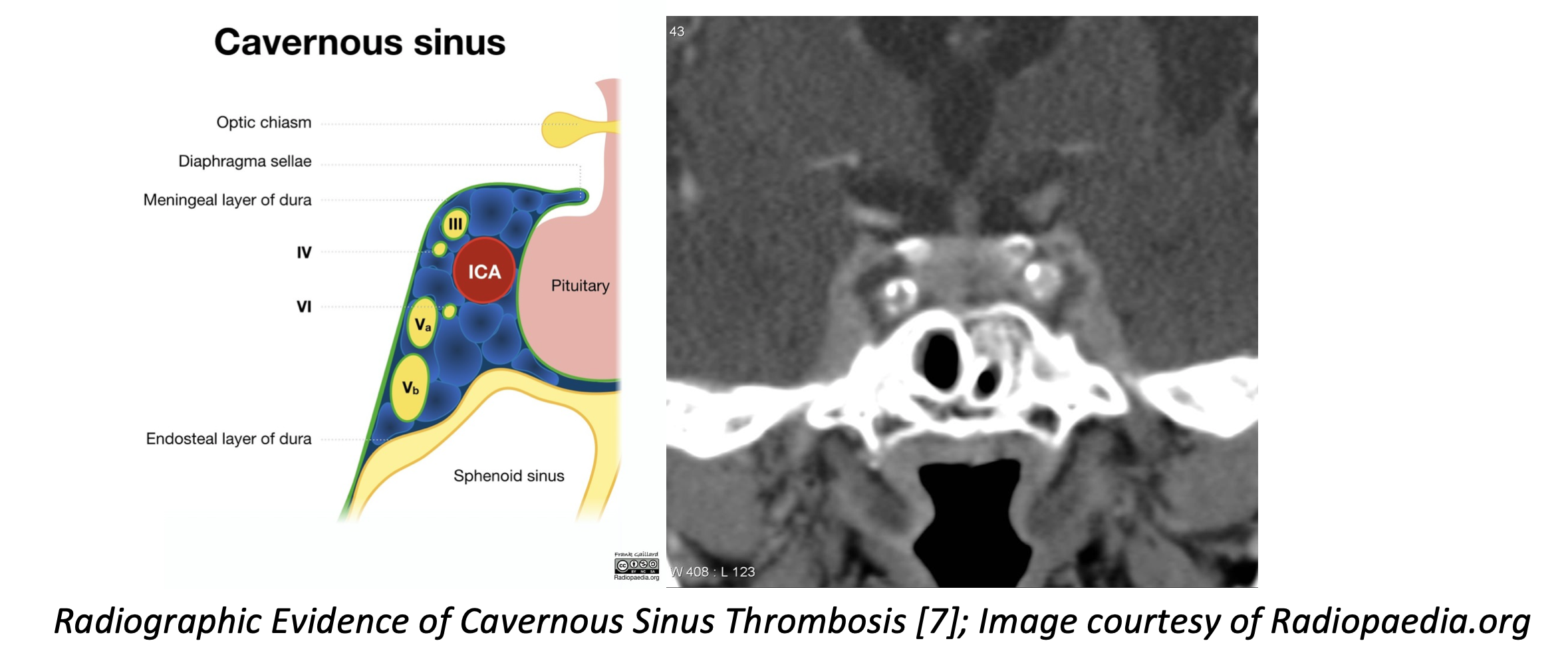
Finally, there are a few additional conditions that require additional workup in the Emergency Department. Cavernous sinus thrombosis is a veno-occlusive episode of the cavernous sinus, which houses many cranial nerves, most importantly 3, 4, and 6 [6]. These patients often present acutely ill, with swelling and pain in the affected eye (the impetus of the infection), possible visual acuity deficits, headache, and multiple risk factors for thromboembolic disease. These patients should obtain CT venogram immediately, along with broad spectrum antibiotics, and blood cultures. CT venogram is very specific, however, it is not sensitive enough to exclude the diagnosis. If the CT venogram is negative, emergent MRV is warranted. Other pathologies that uncommonly present with palsy are thyroid eye disease and Giant Cell Arteritis. Thyroid disease can lead to enlargement and fibrosis of the extraocular musculature, while Giant Cell Arteritis can cause microvascular ischemia from vasculitis. These conditions typically present with typical associated symptoms of their disease process (i.e., you would also expect to see systemic signs of thyroid disease, or unilateral headache in vasculitis). If these conditions are suspected, a TSH or ESR/CRP, respectively, is appropriate. Patients over 50 should have inflammatory markers sent. Myasthenia Gravis is another condition that can present with diplopia, though these patients often present with other symptoms (proximal muscle weakness, respiratory issues), and the diplopia may be intermittent and likely fatigable rather than persistent.
Once the aforementioned acute pathologies have been ruled out, an urgent referral to an ophthalmologist or neurologist is usually warranted; many lesions require further evaluation with non-emergent MRI or advanced ophthalmological techniques. This is especially the case in the setting of complex motility disorders: these are eye movement disorders that present with neurologic findings not localizable to a single cranial nerve. These often require specialty evaluation and imaging to better characterize the deficit involved.
In summary, the general approach to diplopia in the emergency department is as follows:
- Delineate if the diplopia is Monocular or Binocular; the latter requires further evaluation in the emergency department. The former can be referred to ophthalmology.
- Once Binocular Diplopia has been established, if there are any other focal neurologic findings outside of Diplopia, CVA should be heavily considered and the patient should be evaluated for stroke.
- Perform an extraocular exam to ascertain which cranial nerves in question are malfunctioning.
- Isolated 4th nerve palsies and 6th nerve palsies can be referred to a specialist for evaluation and do not require imaging in the ED.
- The presence of 3rd nerve palsy, multiple concomitant palsies, evidence of papilledema, infection, trauma, or cavernous sinus thrombosis require urgent imaging in the ED.
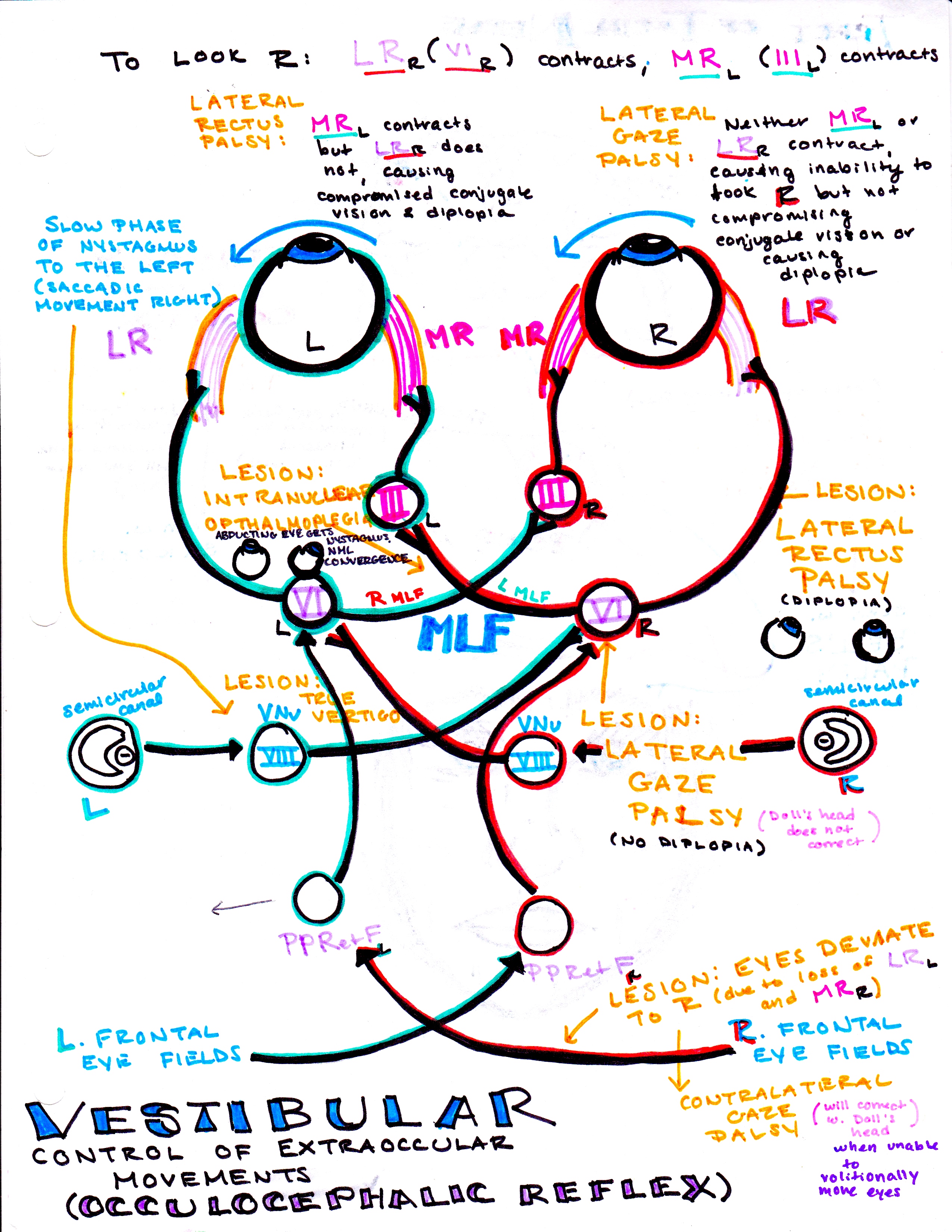
From Dr. Katelyn Hanson and Hanson’s Anatomy:
Case Conclusion
To conclude the opening case, the patient in question had an impressive sixth nerve palsy; her diplopia was easily reproduced on lateral gaze to the right. However, on physical exam, she demonstrated some difficulty with alternating movements on the right side. In light of these additional neurologic findings, she was sent for a CT followed by an MR/MRA, which demonstrated a left non-hemorrhagic pontine infarct.
Summary
In summary, diplopia is a complaint we see infrequently in the emergency department, but one that requires a thorough neurologic and ophthalmologic assessment to rule out debilitating neurological disease. The patient that presents with diplopia should not be imaged routinely, unless a specific underlying etiology is suspected.
Take Home points
- Diplopia is best characterized as monocular or binocular; the latter is generally more concerning and warrants further workup in the ED.
- Diplopia, in addition to any other neurologic deficit, is grounds for a stroke activation and assessment.
- Diplopia does not always require imaging; however certain associated findings warrant specific evaluation:
- 3rdcranial nerve involvement: CTA
- Increased ICP: CT head
- Associated neuro deficits/complex motility disorders: CT head, preferably MRI
- Suspected infection: CT head/orbits with contrast
- Suspected Cavernous Sinus Thrombosis: CTV, followed by MRV if CTV negative
- Patients over age 50 with diplopia should have inflammatory markers ordered.
- Diplopia merits urgent referral to an ophthalmologist or neurologist once immediate, intervenable causes have been ruled out.
References/Further Reading
[1] Gerstenblith, Adam T.; Rabinowitz, Michael P., May 27, 2012, Wills Eye Manual: Office and Emergency Room Diagnosis and Treatment of Eye Disease Wolters Kluwer Health, Philadelphia, ISBN: 9781451186024
[2] Nazerian P, Vanni S, Tarocchi C, Portaccio E, Vannucci N, Para O, Giannazzo G, Gigli C, Grifoni S. Causes of diplopia in the emergency department: diagnostic accuracy of clinical assessment and of head computed tomography. Eur J Emerg Med 2014;21:118–124
[3] Low Liying, Shah Waqaar, MacEwen Caroline J. Double vision BMJ 2015; 351:h5385
[4] Danchaivijitr C, Kennard C. Diplopia and eye movement disorders. J Neurol Neurosurg Psychiatry. 2004;75 Suppl 4(Suppl 4):iv24–iv31. doi:10.1136/jnnp.2004.053413
[5] Dotan G, Rosenfeld E, Stolovitch C, Kesler A: The role of neuroimaging in the evaluation process of children with isolated sixth nerve palsy: Child’s nervous system. Childs Nerve Syst 2013;29:1:89-92.
[6] O’Colmain U, Gilmour C, MacEwen CJ. Acute-onset diplopia. Acta Ophthalmol. 2014;92:382-6
[7] Case courtesy of A.Prof Frank Gaillard, <a href=”https://radiopaedia.org/”>Radiopaedia.org</a>. From the case <a href=”https://radiopaedia.org/cases/5025″>rID: 5025</a>
[8] Margolin E, Lam CT. Approach to a Patient with Diplopia in the Emergency Department. The Journal of Emergency Medicine. 2018;54(6):799-806. doi:10.1016/j.jemermed.2017.12.045.






2 thoughts on “Diplopia Evaluation and Management”
Pingback: July FOAMed - FRCEM Success
Pingback: Länkar v31-34 | Internmedicin