
Authors: Haley Sinatro, MD (EM Resident, UTSW); Colin Danko, MD (Assistant Professor, UTSW EM) // Reviewed by: Sophia Görgens, MD (EM Physician, Northwell, NY); Cassandra Mackey, MD (Assistant Professor of Emergency Medicine, UMass Chan Medical School); Alex Koyfman, MD (@EMHighAK); Brit Long, MD (@long_brit)
Welcome to EM@3AM, an emDOCs series designed to foster your working knowledge by providing an expedited review of clinical basics. We’ll keep it short, while you keep that EM brain sharp.
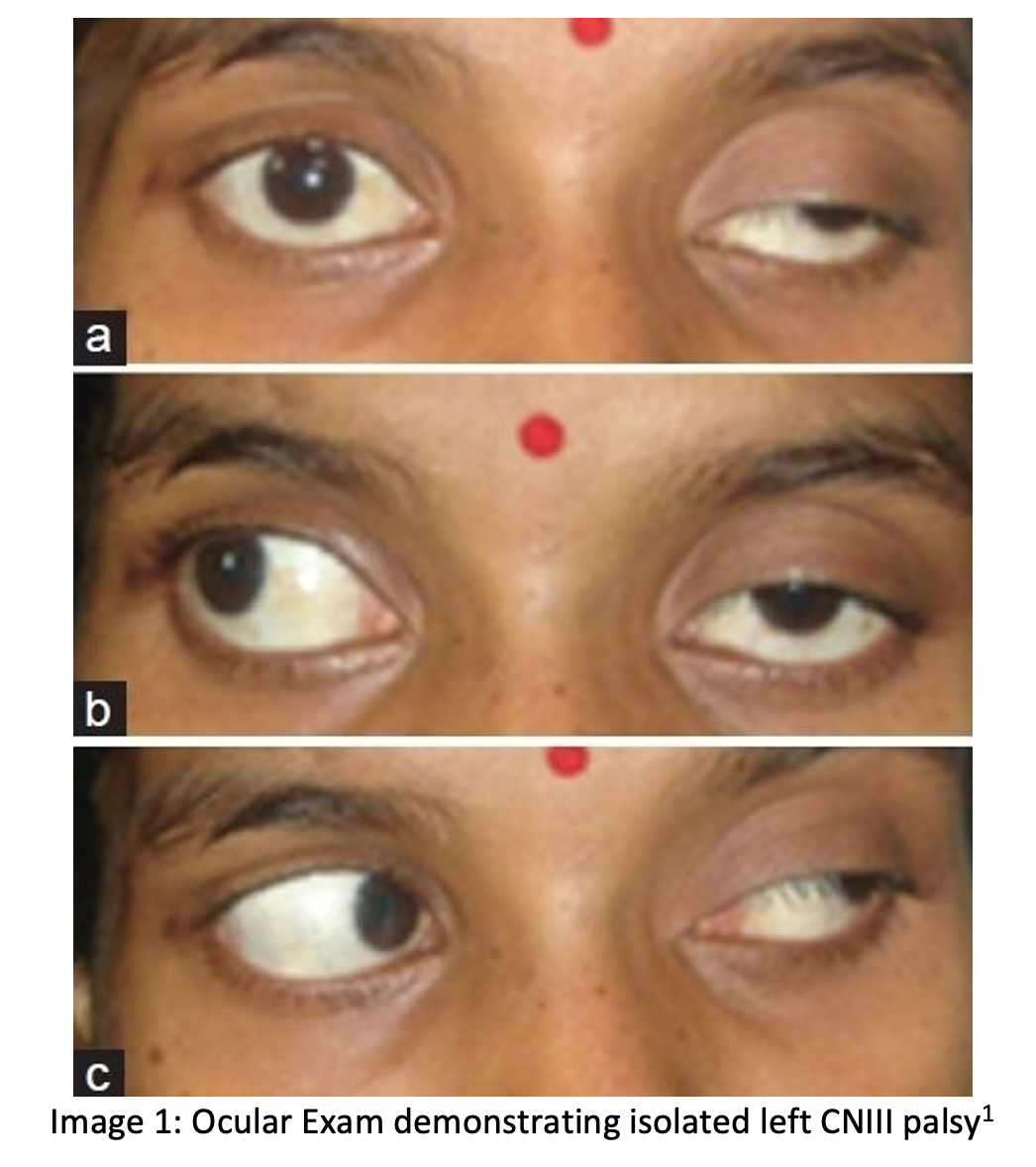
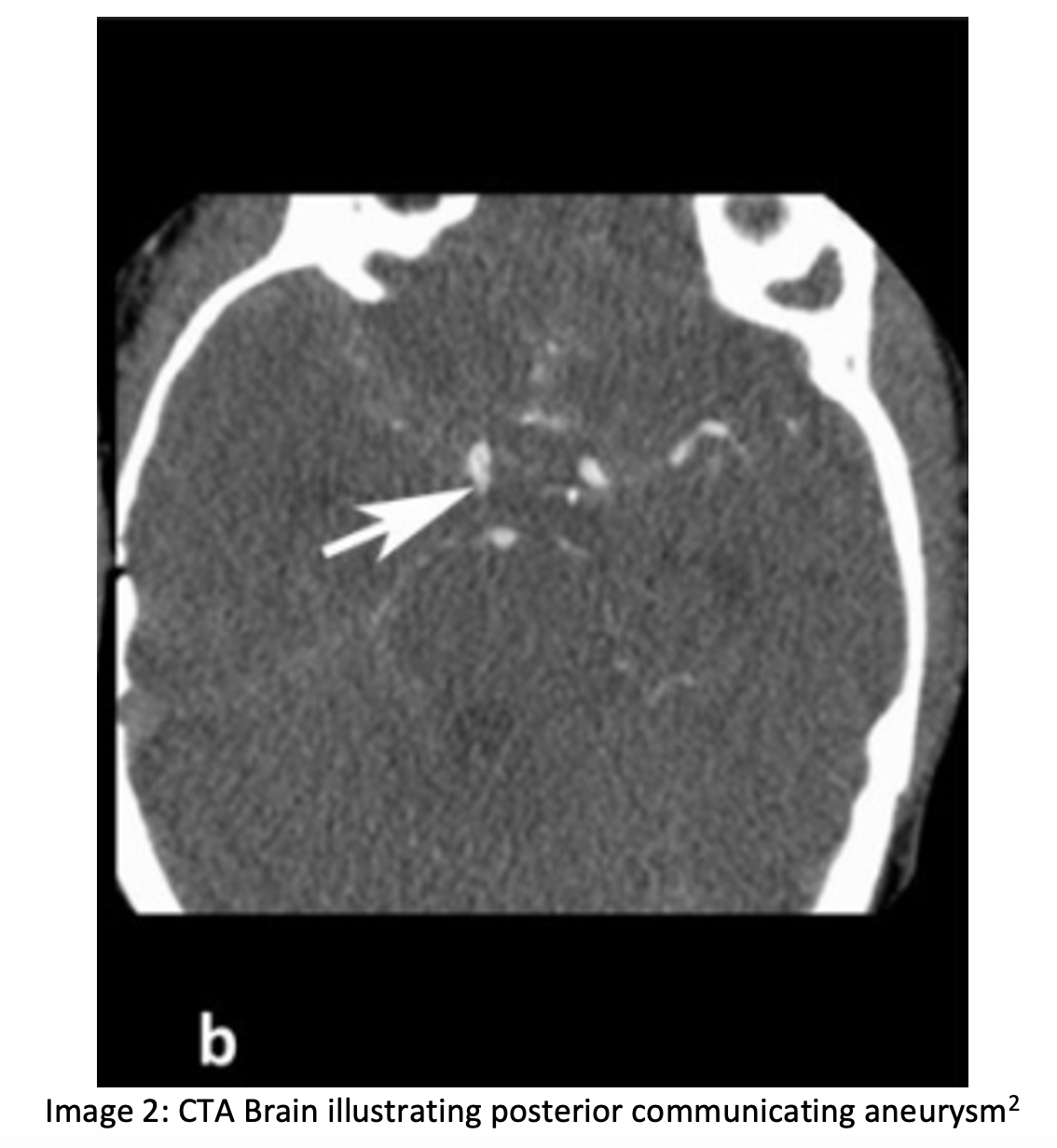
A 50-year-old female with no past medical history presents to the ED with a diffuse, constant headache onset a few weeks. The patient describes droopiness of the left eye and double vision associated with specific directional movements of the eye. On exam, you note ptosis of the left eye with findings as indicated in the photograph below (inability to adduct, ability to abduct). The left pupil is dilated at 5mm and minimally reactive to light; the right pupil is 3mm and reactive. The remaining cranial nerve testing and components of the neurological exam are normal. A CTA Brain cross-section is provided below.
Question: What is the diagnosis?
Answer: Oculomotor Nerve (CNIII) Palsy
Epidemiology
- In adults, acquired CNIII palsy cases are:
- Primarily caused by microvascular etiology
- Most significant risk factors are diabetes, left ventricular hypertrophy, and elevated hematocrit
- hypertension, hypercholesterolemia, heart disease, obesity, tobacco use, prior ocular motor nerve palsy
- Trauma
- Neoplasm
- Post neurosurgery
- Aneurysmal compression3
- Primarily caused by microvascular etiology
- In pediatric patients, 43% of CNIII palsy cases are congenital, with trauma as an additional common cause5
Anatomy
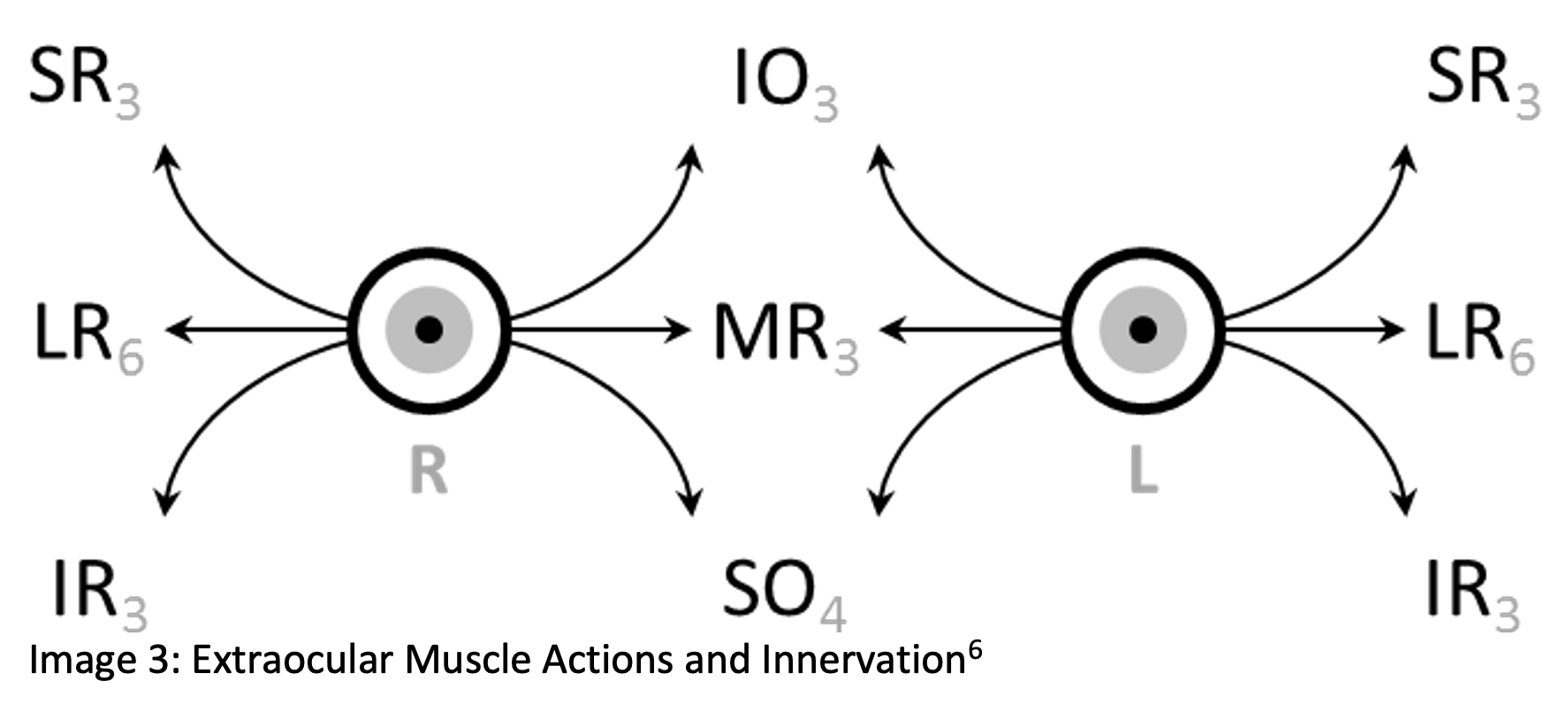
- Oculomotor Nerve Function
- Eyelid muscles
- Medial rectus muscle
- External ocular muscles
- Pupillary constriction
- CNIII carries parasympathetic nerve fibers on its external surface responsible for pupillary constriction
Clinical Presentation
- Headache
- Diplopia
- Exam:
- Ptosis secondary to eyelid muscle dysfunction
- Inability to adduct eye of the affected nerve due to dysfunction of the medial rectus
- May see the inability to infraduct and supraduct due to the dysfunction of the inferior rectus muscle and superior rectus muscle
- Due to the dysfunctional muscles, may see the eye deviated laterally and down
- Pupil exam:
- Dilated and nonreactive: indicates a space-occupying lesion/posterior communicating artery aneurysm compressing CNIII (due to compression of external parasympathetic fibers)
- Spared pupil: indicates ischemic etiology as pupillary fibers run externally on nerve and have more collateral blood supply, making them less susceptible to ischemia than central nerve fibers
Workup
- Important to consider whether this is a space-occupying lesion or other cause (diabetes, ischemic, or inflammatory process)
- Consider diabetes, myasthenia gravis, neurosyphilis, autoimmune vasculitis, giant cell arteritis, thyroid-associated pathology
- If CNIII palsy with ptosis, pupil involvement, and/or other CN involvement, work up for space-occupying lesion/posterior communicating artery aneurysm with CT noncontrast and CTA head
- If CNIII palsy without pupil involvement, work up for ischemic/inflammatory process: labs (CBC, ESR, HgBA1C, TSH, T4, clinical discretion based on suspicion of above etiologies) in addition to CT noncontrast and CTA head to rule out space occupying lesion
- If CNIII palsy in addition to CNIV or CN6, may indicate intraorbital lesion/trauma
- Assess for orbital compartment syndrome, open globe, signs of trauma
Treatment/Disposition
- If aneurysm/mass/space occupying lesion: neurosurgery consult
- If ischemic cause: treat the underlying cause, medical management, ophthalmology follow-up
- If the patient reports diplopia
- Recommend no driving or operating heavy machinery until resolved
- Consider an eye patch for affected eye to improve diplopia
- Consider prism glasses to improve diplopia
- Pediatric Considerations
- For congenital cases, start with occlusion therapy/glasses
- Cases typically proceed to outpatient surgical management to allow for binocular fusion
- Consult ophthalmology in the ED if:
- The patient has any visual field deficit, or visual acuity deficit
- CNIII palsy is the result of orbital trauma
Pearls
- Differential based on neurologic exam and ocular exam (isolated CNIII palsy vs. other nerve involvement)
- Important to rule out vascular causes of CNIII palsy in patients with ptosis, mydriasis, ophthalmoplegia
- Educate patients on safe practices related to driving/operating machinery prior to discharge

A 60-year-old man presents to the emergency department with painless atraumatic diplopia. He has no known medical history and has never been to the doctor. The left eye is deviated inferiorly and laterally during frontward gaze. His pupillary exam is normal, and he has no extremity weakness. Which of the following is most likely to determine the etiology of his diplopia?
A) CT angiogram
B) Orbital CT
C) Serum glucose
D) Tonometry
Answer: C
The patient is exhibiting an oculomotor nerve (cranial nerve III) palsy. The oculomotor nerve innervates the levator palpebrae, superior rectus, medial rectus, and inferior rectus muscles that control the upper lid and extraocular movements. When an oculomotor nerve palsy exists, patients often present with ptosis and the classic “down and out” finding on examination, meaning the affected eye deviates inferiorly and laterally during normal frontward gaze. It is important to assess pupillary response, a differentiating feature when determining the etiology of oculomotor nerve palsy. A dilated pupil in the setting of an oculomotor palsy is a posterior communicating artery aneurysm until proven otherwise. On the other hand, if the pupil is spared and is reactive, the most likely cause is diabetes-related cranial nerve III mononeuropathy. Diabetes mellitus causes peripheral neuropathy due to nonenzymatic glycosylation of the nerves and vascular damage to the pupillomotor fibers within the nerve bundle. The oculomotor nerve is the most commonly affected cranial nerve from long-standing hyperglycemia. Therefore, in this patient with a normal pupillary exam, a serum glucose is most likely to determine the etiology of the palsy.

While a CT angiogram (A) is indicated in patients presenting with a new cranial nerve III palsy, a normal pupillary exam makes an aneurysm less likely in this patient. An orbital CT (B) is of little utility in the evaluation of cranial nerve III palsy in the absence of trauma. Increased intraocular pressure may be a cause of ophthalmoplegia. Conditions that lead to oculomotor palsies in the setting of raised intraocular pressure, such as retrobulbar hematoma, orbital cellulitis, or acute angle closure glaucoma, often present with pain. Because this patient is pain-free, tonometry (D) is not likely to be diagnostic in this case.
FOAM Reading
- https://wikem.org/wiki/Third_nerve_palsy
- https://eyewiki.aao.org/Acquired_Oculomotor_Nerve_Palsy#Disease_Entity
- https://litfl.com/third-cranial-nerve-lesions/
References:
- Diyora B, Kukreja S, Nayak N, Kamble H, Sharma A. Complete third nerve palsy: Only presenting sign of extradural hematoma in an awake patient. Oman J Ophthalmol. 2014 May;7(2):103-4. doi: 10.4103/0974-620X.137177. PMID: 25136243; PMCID: PMC4134542.
- Kelliny, M., Maeder, P., Binaghi, S. et al.Cerebral aneurysm exclusion by CT angiography based on subarachnoid hemorrhage pattern: a retrospective study. BMC Neurol 11, 8 (2011). https://doi.org/10.1186/1471-2377-11-8
- Fang C, Leavitt JA, Hodge DO, Holmes JM, Mohney BG, Chen JJ. Incidence and Etiologies of Acquired Third Nerve Palsy Using a Population-Based Method. JAMA Ophthalmol. 2017 Jan 1;135(1):23-28. doi: 10.1001/jamaophthalmol.2016.4456. PMID: 27893002; PMCID: PMC5462106.
- Jacobson DM, McCanna TD, Layde PM. Risk factors for ischemic ocular motor nerve palsies. Arch Ophthalmol. 1994 Jul;112(7):961-6. doi: 10.1001/archopht.1994.01090190109029. PMID: 8031277
- Modi P, Arsiwalla T. Cranial Nerve III Palsy. [Updated 2022 Jul 4]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK526112/
- yousef, CC BY-SA 4.0 <https://creativecommons.org/licenses/by-sa/4.0>, via Wikimedia Commons




