
Welcome to EM@3AM, an emDOCs series designed to foster your working knowledge by providing an expedited review of clinical basics. We’ll keep it short, while you keep that EM brain sharp.
A 30-year-old otherwise healthy female presents to the ED after sustaining a motorcycle collision at highway speeds. She was wearing protective equipment, including a helmet, gloves, knee and elbow pads, and riding boots. She denies loss of consciousness but reports severe right lower extremity pain rated as 10 out of 10.
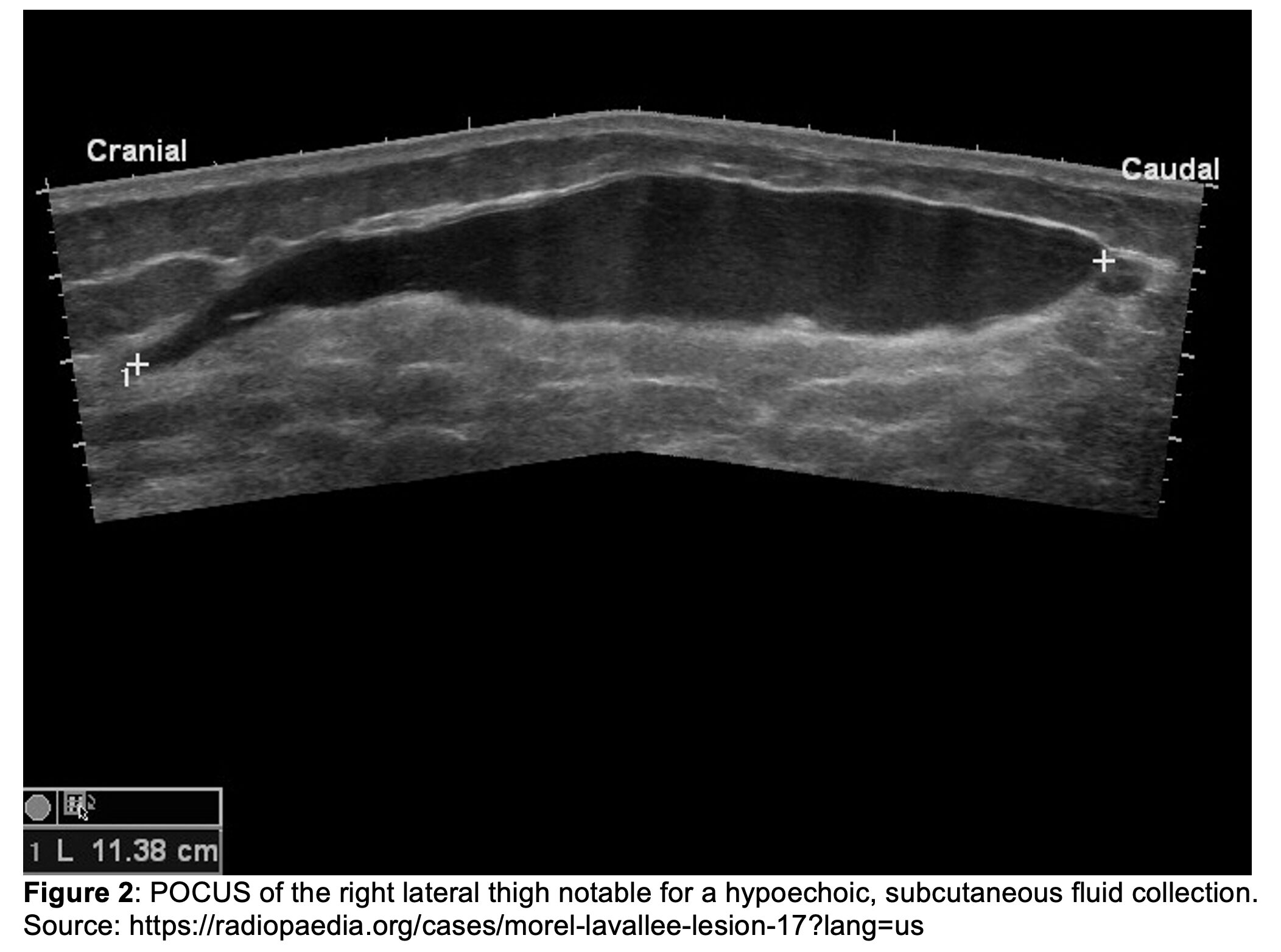
Initial vital signs are notable for BP 93/78 mmHg, HR 122 bpm, T 98.1°F, RR 26/min, and SpO₂ 97% on room air. She is alert with a GCS of 15 but appears in acute distress secondary to pain. Primary trauma survey reveals an intact airway, bilateral breath sounds, and symmetric 1+ distal pulses in all extremities. Bedside imaging of the chest, pelvis, and femur, as well as an eFAST exam, are unremarkable. During the secondary survey, a rapidly expanding mass is noted over the right lateral thigh (Figure 1). The overlying skin is tense and tender to palpation. Point-of-care ultrasound (POCUS) of the region is obtained to further characterize the swelling (Figure 2).

What is the diagnosis?
Answer: Morel-Lavallée Lesion
Epidemiology
- First described in 1863 as a closed soft-tissue degloving injury caused by high-impact shearing forces1
- Present in up to 8.3% of acetabular fractures1
- True prevalence may be higher, as small-volume lesions are often overlooked2-3
- Occurs more commonly in males than females, likely related to male predominance in polytrauma1,4
Pathophysiology
Mechanism
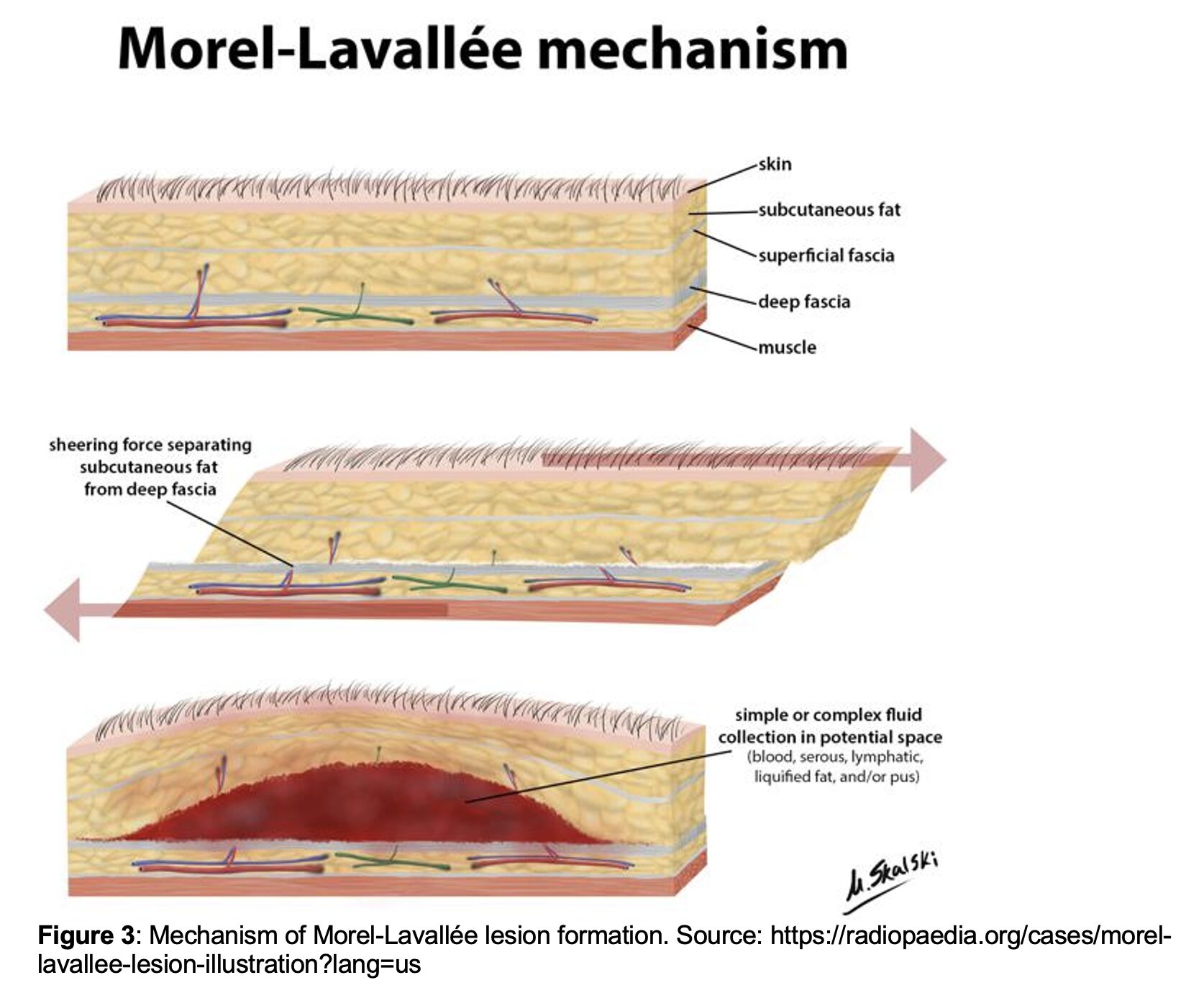
- Typically caused by high-energy shearing forces that separate subcutaneous tissue from the underlying fascia
- Results in vascular and lymphatic disruption with subsequent leakage into the trauma-created space (Figure 3)
Stages of Morel-Lavallée Lesions5
- Acute injury: Subcutaneous layers are separated from the fascia by high-impact shearing forces
- Filling: Injured blood and lymphatic vessels leak into the newly created space
- Coagulation: Hemorrhagic components become replaced by serosanguinous fluid as the lesion enlarges
- Pseudocapsule formation: Ongoing inflammation and clotting lead to fibrous encapsulation, preventing fluid reabsorption
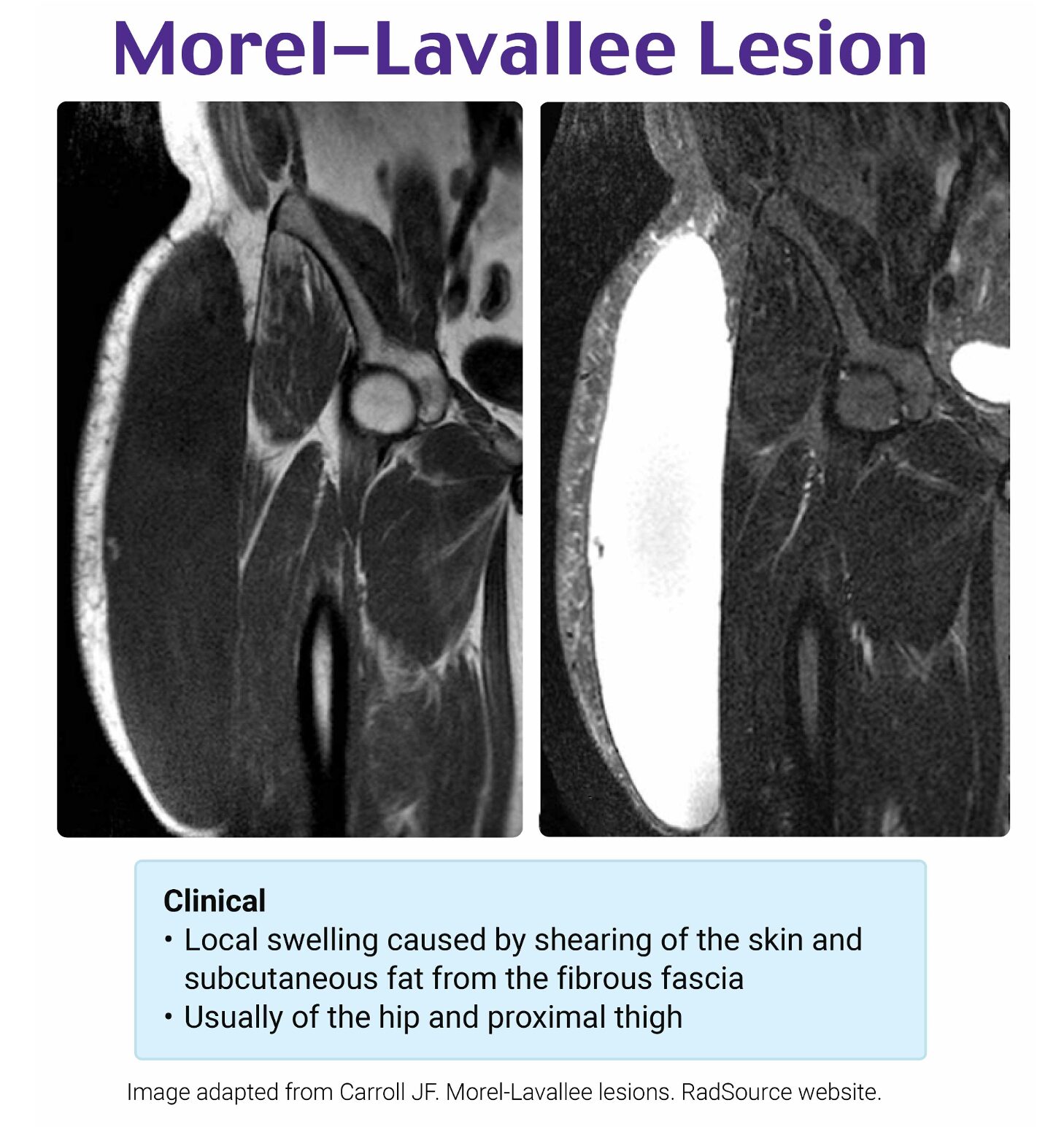
Classification of Morel-Lavallée Lesions6
- Six MRI-based radiographic classes
- Type I: acute seroma
- Type II: subacute hematoma
- Type III: chronic organizing hematoma
- Type IV: closed laceration
- Type V: pseudonodular
- Type VI: infected lesion
- MRI is helpful for accurate classification but not required for the diagnosis of Morel-Lavallée Lesions
Common Anatomical Locations1,7
- Occur most often in areas of skin hypermobility
- Frequently associated with pelvic and femoral fractures
- Prevalence by location (descending order):
- Greater trochanter and hip (60%)
- Pelvis (15%)
- Thigh (10-15%)
- Knee (5-10%)
- Lumbosacral and gluteal regions (5%)
- Other sites such as the abdomen, calf and lower leg, and scalp reported but less common (<5%)
Clinical Presentation
Subjective Findings
- Pain at the site
- Local edema
- Ecchymosis
- Possible skin breakdown
Timing
- Up to ⅓ may present weeks after the initial injury8
Objective Findings1,7-8
Vital Signs
- May be normal
- Can reflect hemorrhagic shock (e.g., tachycardia, hypotension)
Cardiovascular
- Pulses usually normal but may be diminished or absent
Musculoskeletal
- Obvious deformities suggesting concomitant injuries
Neurological
- Motor: typically intact if injury is superficial
- Sensation: may be decreased due to cutaneous nerve disruption
Dermatological
- Overlying abrasions, lacerations, or ecchymosis
- Hypermobile skin
- Subcutaneous fluctuance
Differential Diagnoses
- Fracture, dislocation, hematoma, seroma, bursitis, lipoma, hernia, abscess, necrotizing soft tissue infection
Evaluation
Labs
- Traumatic / Hemorrhagic Workup
- CBC, CMP, lactate, coagulation panel (PT, PTT/INR, TEG)
- Infectious workup
- Consider in subacute and chronic cases with systemic illness or concerning skin changes
- Lactate
- Blood cultures
- Needle aspiration/culture (per surgical consultant)
Imaging
- POCUS9-10
- Useful as an initial diagnostic tool
- Color Doppler may show active bleeding
- CT ± Angiography11
- Helps map lesion size for operative planning
- Contrast extravasation may indicate active bleeding
- MRI6-10
- Not required for diagnosis
- Helpful for lesion classification and treatment planning
Complications
Missed Diagnosis
- Morel-Lavallée lesions can be easily overlooked, leading to significant downstream complications12
Hemorrhage13-14
- Rare but reported cases of hemorrhagic shock and death
Compressive Dermonecrosis and Myonecrosis1,15
- May require debridement and skin grafting
- Supportive management until definitive surgical intervention
Infection
- Morel-Lavallée lesions can serve as a medium for bacterial growth
- Secondary infection reported in 46% of patients in one study2
- Independently associated with post-operative pelvic ORIF infections16
Recurrence1
- Occurs in up to 75% of evacuated Morel-Lavallée lesions
- Recurrence may require repeat treatment depending on presentation
Treatment
Active Hemorrhage
- ABCs and resuscitation if hemodynamically unstable
- IV fluids and blood products
- Small MLLs may distract from other major bleeding sources
- Direct pressure and pressure dressing
- Reversal agents for antiplatelets or anticoagulants if life-threatening hemorrhage
- Operative management for hematoma evacuation and vessel ligation
Secondary Infection
- Obtain labs, lactate, and blood cultures
- Discuss aspirate cultures with surgical specialists (usually either orthopedics or trauma)
- Infections can be polymicrobial, to include Gram-positive, Gram-negative, and anaerobic organisms2,12
- Administer empiric broad-spectrum antibiotics (e.g., vancomycin + piperacillin-tazobactam)
Analgesia
- Acute: multimodal pain control including opioids
- Chronic/stable: supportive care with multimodal analgesia (acetaminophen, NSAIDs, gabapentin, topical anesthetics); avoid prolonged opioids
Dermonecrosis and Myonecrosis
- Consult surgery for operative management (e.g., debridement and skin grafting)
Subacute and Chronic Lesions
- Small, nonoperative lesions may take weeks to heal
- Conservative Management17
- Small lesions (<50 mL) may be discharged with compression bandage and close follow-up
Surgical Interventions
- Dependent on lesion size, severity, and proximity to incision site for coexisting injuries8
- Mixed data on indications/outcomes; consult surgery for potential interventions:
- Needle aspiration18
- Incision and drainage19
- Debridement with capsule resection20
- Sclerodesis4
- Irrigation with caustic antibiotics or alcohol to promote subdermal adhesion/scarring
Disposition1,8,17,19-20
Unstable
- Prioritize resuscitation
- Consult general or orthopedic surgery for operative management
Acute
- Obtain surgical consultation for initial recommendations
Subacute
- Surgical consultation for further guidance, especially if symptomatic changes occur
Chronic and Stable
- Compression wrapping
- Outpatient follow-up with surgery
Case Follow-Up
The patient received 2 units of whole blood, 2 g TXA, 3 g calcium gluconate, and a tetanus booster in the trauma bay, resulting in improved hemodynamics. She was given 100 mcg of fentanyl. A CT angiogram of her lower extremity showed active contrast extravasation into the lesion. She was taken to the OR for operative management, where an arteriole was ligated, resolving her hemorrhage. The remaining hematoma was evacuated. She was eventually discharged with compression bandaging over the site.
Pearls
- Morel-Lavallée lesions are soft tissue shearing injuries between subcutaneous fat and fascia, leading to serosanguinous fluid accumulation
- Often missed due to subtlety and presence of other significant injuries
- Associated with high risk of infection and/or tissue necrosis
- Early trauma or orthopedic surgical consultation is critical to guide treatment and disposition

A 32-year-old man presents to the ED after a motorcycle collision. He reports localized pain and swelling over his right greater trochanter. On examination, there is a fluctuant, soft, and tender area over the lateral thigh without overlying skin discoloration. Plain radiographs are negative for fracture. Point-of-care ultrasound reveals an anechoic fluid collection superficial to the fascia lata. What best describes the pathophysiology of this patient’s most likely condition?
A) Disruption of myotendinous fibers with intramuscular hematoma formation
B) Hemarthrosis due to intra-articular capsule rupture
C) Local abscess formation within the deep soft tissues
D) Lymphatic leakage from disruption of superficial lymphatic channels
C) Separation of subcutaneous tissue from underlying fascia with fluid accumulation
Correct answer: E
Morel-Lavallée syndrome is a closed soft tissue degloving injury resulting from shearing forces that separate the subcutaneous tissue from the underlying fascia. This separation creates a potential space that fills with hemolymphatic fluid, necrotic fat, and sometimes blood. The most common mechanism is high-energy trauma, such as a motor vehicle or motorcycle collision, that causes tangential or crush forces. Although classically associated with the greater trochanter and lateral thigh, lesions can occur over the sacrum, lumbar spine, or scapula.
Clinically, patients often present with a fluctuant, soft, and sometimes painful mass that may enlarge over time. Skin over the lesion may appear normal or ecchymotic, but is usually intact. In the acute setting, plain radiographs are often unrevealing. Point-of-care ultrasound can detect a hypoechoic or anechoic collection superficial to the muscle fascia. MRI is the gold standard for diagnosis, particularly when the lesion is chronic or organizing, as it can help distinguish it from abscess, hematoma, and soft-tissue tumor.
ED management focuses on confirming the diagnosis, excluding more serious injuries (e.g., fracture, open injury, vascular compromise), and initiating appropriate wound care. Acute lesions can often be treated with compression and aspiration, depending on lesion size, whereas chronic or recurrent collections may require surgical debridement. Complications include infection, encapsulation, chronic fluid collections, and skin necrosis.
While muscle contusions or strains can cause hematoma (A) within the muscle belly, they are typically deep and intramuscular rather than superficial and subcutaneous. This patient’s ultrasound showed an anechoic fluid collection superficial to the fascia lata, which is inconsistent with a myotendinous injury. Furthermore, muscle injuries often present with a limited range of motion and localized deep tenderness rather than a fluctuant mass.
Hemarthrosis (B) would manifest with joint swelling, decreased range of motion, and pain localized to the joint itself. In this case, the fluctuant mass is over the lateral thigh and not within a joint capsule. Additionally, the absence of joint effusion on examination and the ultrasound findings make an intra-articular process less likely.
Abscesses (C) typically present with signs of infection, including warmth, erythema, fluctuance, and systemic symptoms such as fever. This patient has no constitutional symptoms and no overlying skin changes to suggest infection. Additionally, the context of acute trauma and the ultrasound showing an anechoic rather than heterogeneous or loculated collection makes abscess unlikely.
Lymphatic leakage (D) might occur in traumatic or postoperative settings, but isolated lymphatic disruption without fascial separation does not account for the described lesion. Morel-Lavallée lesions involve a traumatic cleavage plane between the subcutaneous tissue and deep fascia, not just superficial lymphatic injury. The typical presentation and anatomic location strongly favor a degloving injury over isolated lymphatic damage.
References
- Yang Y, Tang TT. The Morel-Lavallée Lesion: Review and Update on Diagnosis and Management. Orthop Surg. 2023;15(10):2485-2491. doi:10.1111/os.13826
- Hak DJ, Olson SA, Matta JM. Diagnosis and management of closed internal degloving injuries associated with pelvic and acetabular fractures: the Morel-Lavallée lesion. J Trauma. 1997;42(6):1046-1051. doi:10.1097/00005373-199706000-00010
- Hudson DA. Missed closed degloving injuries: late presentation as a contour deformity. Plast Reconstr Surg. 1996;98(2):334-337. doi:10.1097/00006534-199608000-00020
- Shen C, Peng JP, Chen XD. Efficacy of treatment in peri-pelvic Morel-Lavallee lesion: a systematic review of the literature. Arch Orthop Trauma Surg. 2013;133(5):635-640. doi:10.1007/s00402-013-1703-z
- Morel-Lavallee Lesion – Trauma – Orthobullets. Accessed November 19, 2025. https://www.orthobullets.com/trauma/422820/morel-lavallee-lesion
- Mellado JM, Bencardino JT. Morel-Lavallée lesion: review with emphasis on MR imaging. Magn Reson Imaging Clin N Am. 2005;13(4):775-782. doi:10.1016/j.mric.2005.08.006
- Vanhegan IS, Dala-Ali B, Verhelst L, Mallucci P, Haddad FS. The morel-lavallée lesion as a rare differential diagnosis for recalcitrant bursitis of the knee: case report and literature review. Case Rep Orthop. 2012;2012:593193. doi:10.1155/2012/593193
- Scolaro JA, Chao T, Zamorano DP. The Morel-Lavallée Lesion: Diagnosis and Management. J Am Acad Orthop Surg. 2016;24(10):667-672. doi:10.5435/JAAOS-D-15-00181
- Neal C, Jacobson JA, Brandon C, Kalume-Brigido M, Morag Y, Girish G. Sonography of Morel-Lavallee lesions. J Ultrasound Med. 2008;27(7):1077-1081. doi:10.7863/jum.2008.27.7.1077
- De Coninck T, Vanhoenacker F, Verstraete K. Imaging Features of Morel-Lavallée Lesions. J Belg Soc Radiol. 2017;101(Suppl 2):15. Published 2017 Dec 16. doi:10.5334/jbr-btr.1401
- McKenzie GA, Niederhauser BD, Collins MS, Howe BM. CT characteristics of Morel-Lavallée lesions: an under-recognized but significant finding in acute trauma imaging. Skeletal Radiol. 2016;45(8):1053-1060. doi:10.1007/s00256-016-2374-y
- AlJuwied H, AlNajadah D, Mostafa Z, Ashraf A, Jarragh A, Lari A. Missed and mismanaged: severe consequences of Morel Lavallee lesions-a case series. J Surg Case Rep. 2025;2025(9):rjaf731. Published 2025 Sep 14. doi:10.1093/jscr/rjaf731
- Claassen L, Franssen MA, de Loos ER. A Rare Case of Hemorrhagic Shock: Morel-Lavallée Lesion. Clin Pract Cases Emerg Med. 2019;3(4):417-420. Published 2019 Oct 21. doi:10.5811/cpcem.2019.9.43674
- Daghmouri MA, Ben Ismail I, Ouesleti M, et al. Morel-Lavallée lesion as an unusual cause of hemorrhagic shock: Case report and review of literature. Int J Surg Case Rep. 2020;77:759-761. doi:10.1016/j.ijscr.2020.11.108
- Molina BJ, Ghazoul EN, Janis JE. Practical Review of the Comprehensive Management of Morel-Lavallée Lesions. Plast Reconstr Surg Glob Open. 2021;9(10):e3850. Published 2021 Oct 7. doi:10.1097/GOX.0000000000003850
- Lai CY, Lai PJ, Tseng IC, et al. Morel-Lavallee lesions and number of surgeries for associated injuries predict surgical site infection risk following pelvic ring injury osteosynthesis. Sci Rep. 2023;13(1):8208. Published 2023 May 22. doi:10.1038/s41598-023-35488-8
- Rodríguez-Roiz JM, Burillo JM, Díaz JSS. Morel-Lavallee lesions. Size matters? Treatment and time of disability. Injury. 2023;54(1):150-153. doi:10.1016/j.injury.2022.10.023
- Tejwani SG, Cohen SB, Bradley JP. Management of Morel-Lavallee lesion of the knee: twenty-seven cases in the national football league. Am J Sports Med. 2007;35(7):1162-1167. doi:10.1177/0363546507299448
- Nickerson TP, Zielinski MD, Jenkins DH, Schiller HJ. The Mayo Clinic experience with Morel-Lavallée lesions: establishment of a practice management guideline. J Trauma Acute Care Surg. 2014;76(2):493-497. doi:10.1097/TA.0000000000000111
- Singh R, Rymer B, Youssef B, Lim J. The Morel-Lavallée lesion and its management: A review of the literature. J Orthop. 2018;15(4):917-921. Published 2018 Aug 28. doi:10.1016/j.jor.2018.08.032




