
Author: Vivek Medepalli, MD (EM Resident Physician, UTSW / Parkland Memorial Hospital) and Christine Kulstad (EM Attending Physician, UTSW / Parkland Memorial Hospital) // Reviewed by: Brit Long, MD (@long_brit, EM Attending Physician, San Antonio, TX); Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UTSW / Parkland Memorial Hospital); Sophia Görgens, MD (EM Resident Physician, Zucker-Northwell NS/LIJ, NY); Cassandra Mackey, MD (Assistant Professor of Emergency Medicine, UMass Chan Medical School)
Welcome to EM@3AM, an emDOCs series designed to foster your working knowledge by providing an expedited review of clinical basics. We’ll keep it short, while you keep that EM brain sharp.
A 59-year-old male presents to the ED with abdominal pain, hematuria, and rectal bleeding for the 5 days. His symptoms have been associated with unintentional weight loss, intermittent fevers, skin rash, and fatigue over the past 3 months. He has a past history of hepatitis B, hypertension, diabetes, and hyperlipidemia. Vital signs include blood pressure 162/103 mm Hg (last measured 118/82 5 months ago, per records), HR 101, RR 18, SpO2 98% on room air. Exam is notable for generalized abdominal tenderness, guaiac positive stool, and generalized purpuric rash over bilateral lower extremities. Labs demonstrate Cr 2.9 (baseline 1.1) and elevated ESR and CRP.
What is the most likely diagnosis, and what are the next steps in management?
Answer: Polyarteritis Nodosa (PAN)
Epidemiology and Etiology:
- Median age of diagnosis within sixth decade of life [1]
- Males more commonly affected than females (1.5:1 predominance)
- Incidence: 4.4-9.7 per million
- Prevalence: 2-33 per million
- Primarily associated with hepatitis B and hepatitis C virus
- Incidence has decreased with widespread hepatitis B vaccination [2]
- Rarely, polyarteritis nodosa can be seen in children due to loss of function mutations in adenosine deaminase 2 (ADA2) [2]
Pathophysiology:
- Medium-vessel systemic necrotizing vasculitis defined by intimal proliferation, leading to narrowing and decreased flow in affected vasculature
- Medium-vessel primarily refers to renal and visceral arteries/arterioles.
- Affected vasculature is prone to thrombosis and aneurysm [3]
- Mechanism of pathogenesis is unknown; thought to be driven by circulating immune complexes
- Kidney is the most commonly affected organ; however, multi-system involvement, most commonly affecting skin, cardiac, gastrointestinal, and neurologic vasculature
Clinical Features and Disease Course:
- Renal insufficiency
- Hypertension
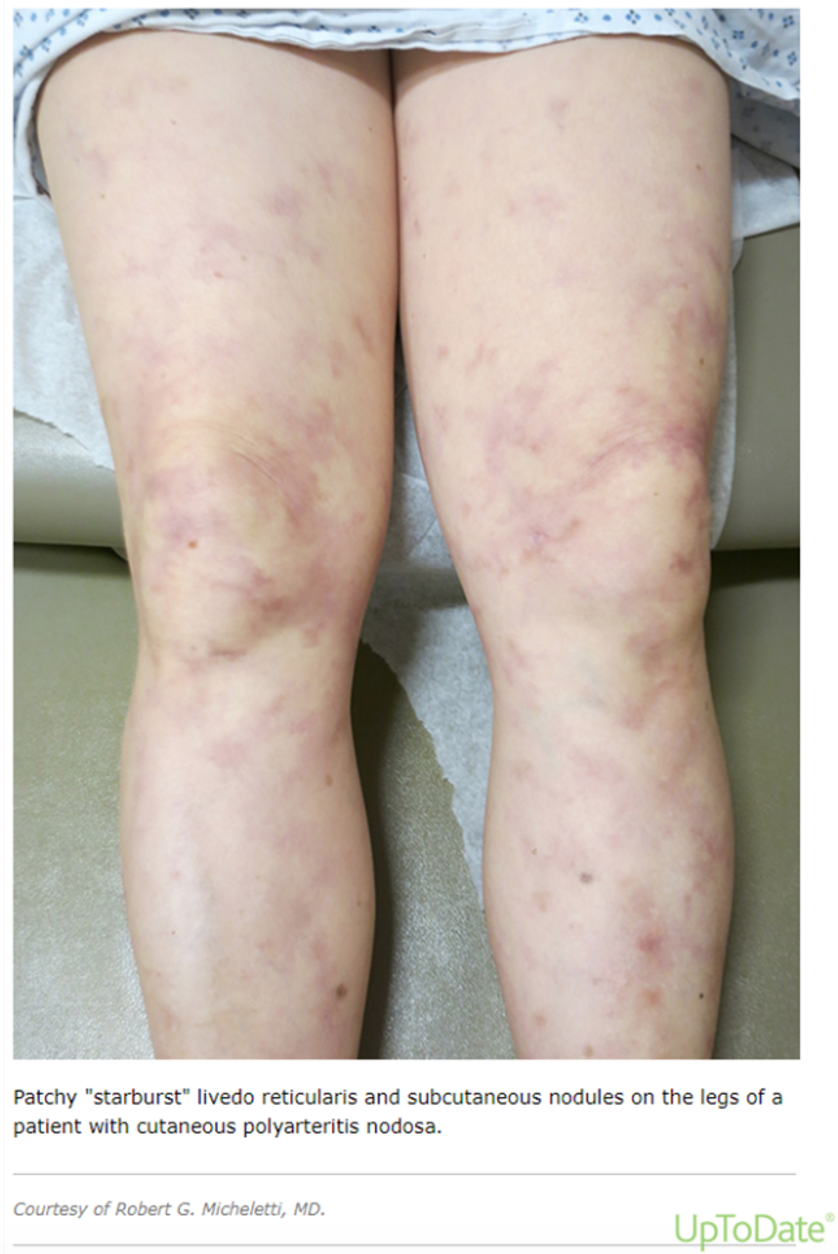
- Cutaneous involvement: subcutaneous nodules, livedo reticularis, purpura, digital infarction, necrosis
- Abdominal pain (common in early part of disease process) [3]
- “Intestinal angina”
- More prone to mesenteric ischemia and bowel infarction
- Most common neurologic finding: mononeuritis multiplex
- Occurs in nearly 70% of patients with the disease with PAN
- Asynchronous motor and sensory peripheral neuropathy occurring in at least two separate nerve areas [4]
- Patients often present with progressive numbness or weakness of >2 different areas (ex. Right foot drop, weakness with left shoulder abduction, and right second finger numbness)
- Given nonspecific symptoms, diagnosis in the emergency department is difficult
- Consider PAN in patients with history of hepatitis B and new onset renal insufficiency with associated skin findings and peripheral neurologic changes

Evaluation and Laboratory Findings:
- Primarily a clinical diagnosis; laboratory tests can be used to assess individual organ involvement
- Renal involvement:
- BUN/Serum Cr
- Will be elevated in PAN
- Creatine Kinase
- Often elevated in PAN
- BUN/Serum Cr
- Liver function tests (LFTs): AST, ALT, alkaline phosphatase, bilirubin
- Rheumatologic markers are useful to rule out other pathology, but are not specific for PAN
- ANA
- Nonspecific, can be used to rule out inflammatory etiology of patient’s condition
- ANCA
- Positive p-ANCA argues against PAN; this maker is commonly seen in microscopic polyangiitis
- Anti-CCP
- Specific for rheumatoid arthritis
- Complement levels
- SPEP/UPEP
- Rheumatoid factor
- ANA
- Renal involvement:
- Hepatitis serologies and HIV testing
- Hepatitis B commonly associated with PAN
- American College of Rheumatology Criteria (3/10 needed, 82% sensitivity, 87% specificity)
- Unexplained weight loss (> 4kg)
- Livedo reticularis
- Testicular pain/tenderness
- Myalgias
- Mono/polyneuropathy
- New onset DBP > 90mmHg
- Elevated BUN (> 40 mg/dL) or Cr (> 1.5 mg/dL)
- History of HBV infection
- Biopsy of small- or medium-sized arteries containing polymorphonuclear cells
Differential Diagnosis:[5]
- Large vessel vasculitis:
- Giant cell arteritis
- Takayasu arteritis
- Medium vessel vasculitis:
- Kawasaki disease
- Small vessel vasculitis:
- Eosinophilic granulomatosis with polyangiitis (Churg-Strauss)
- Granulomatosis with polyangiitis
- IgA-associated vasculitis
- Microscopic polyangiitis
- Endocarditis
- HIV
Complications:
- Renal injury/hypertension
- Involvement of the renal artery seen in approximately one-third of cases
- Ischemia/infarction (mesenteric, renal, cerebral, myocardial)
- Seen in virtually all patients within 5-10 years without treatment
Prognosis:
- Without treatment, 5-year survival rate is less than 15% [5]
- With treatment, 5-year survival close to 80%
- Better prognosis with sole cutaneous involvement [6]
- Poor prognostic factors include renal, gastrointestinal, or neurologic involvement
Treatment:
- PAN often presents with vague symptoms and is difficult to diagnose in the ED setting
- These patients are often admitted based on sequelae of the disease (AKI, intractable pain, neurologic symptoms) and diagnosis is made during admission
- Specialist consultations:
- Rheumatology consultation to guide medication therapy
- Gastroenterology if GI involvement present
- Nephrology if renal involvement present
- Surgery if there is evidence of bowel ischemia/infarction
- Mild PAN (cutaneous involvement only): Prednisone 1mg/kg QD [7]
- Moderate-to-Severe PAN: Prednisone 1mg/kg + Cyclophosphamide 2mg/kg daily
- Continue cyclophosphamide for over 4 months (until remission)
- DMARDs (azathioprine, methotrexate, mycophenolate) can be used in resistant disease
Disposition:
- Unknown diagnosis/suspected diagnosis: Rheumatology consultation, admission for further workup
- Known diagnosis of PAN:
- Mild PAN: Discharge, outpatient follow up
- Moderate-to-Severe PAN with organ injury (ex. Elevated Cr) or off of medication: Admit for initiation of immunosuppressive
Summary and Pearls
- Polyarteritis nodosa is a systemic vasculitis affecting medium-sized arteries
- Affects various organ systems including skin, kidneys, nerves, GI tract
- PAN is associated with hepatitis B and C
- Cutaneous-only involvement is associated with a better prognosis; multi-organ involvement is associated with poorer prognosis
- Treatment includes specialist consultation and corticosteroids alone or in conjunction with cyclophosphamide/DMARDs

A 57-year-old man presents with left testicular tenderness and swelling for 2 days. He also notes that he has had fatigue, muscle pains, and weight loss for several months. He is not sexually active but reports intravenous drug use. His blood pressure is 190/92 mm Hg, his heart rate is 80 bpm, and his temperature is 99.9°F (37.7°C). His physical exam reveals testicular swelling and tenderness. He also has lacy purple discoloration in his legs with palpable purpura and tender skin nodules on the anterior right lower leg. Ultrasound of his testicle shows increased blood flow and inflammation to the left testicle. Which of the following is the most effective management?
A) Ceftriaxone and doxycycline
B) Detorsion and surgical fixation
C) Observation and supportive care
D) Prednisone and cyclophosphamide
Answer: D
Polyarteritis nodosa is a systemic necrotizing vasculitis that affects medium-sized muscular arteries and sometimes small arteries. The age of onset for polyarteritis nodosa is typically > 50 years old. It is sometimes associated with recent hepatitis B or C infection, so intravenous drug use is a risk factor. Symptoms may be systemic (e.g., fatigue, myalgias, weight loss, malaise, fever) or related to vasculitis of the various systems. For example, cardiac manifestations include an increased risk of acute coronary syndrome, myocardial infarction, pericarditis, peripheral artery ischemia, and heart failure. In the nephric system, manifestations include renal artery aneurysm, malignant hypertension, and kidney insufficiency. Another common site of vasculitis is the skin, resulting in tender nodular skin lesions, palpable purpura, ulcerations, and livedo reticularis—a lacy purple discoloration of the skin. Neurological involvement can cause peripheral mononeuropathy with motor and sensory symptoms and acute ischemic or hemorrhagic stroke. Other common systems affected include ophthalmic (e.g., central retinal artery occlusion, optic neuropathy) and gastrointestinal (e.g., abdominal pain, mesenteric ischemia, GI bleeding, bowel perforation, acute pancreatitis).Orchitis is another possible manifestation of polyarteritis nodosa. As in other etiologies of orchitis, ultrasound shows increased blood flow and inflammation of the testicle. Pulmonary manifestations are not common in polyarteritis nodosa. Glucocorticoids, such as prednisone, are a first-line treatment for mild polyarteritis nodosa. More severe cases require immunosuppressive drugs such as cyclophosphamide. In patients with risk factors and findings concerning for viral hepatitis, antivirals are the first-line therapy and are recommended prior to immunosuppressive drugs.
Ceftriaxone and doxycycline (A) is the treatment recommended for orchitis suspected to be due to a sexually transmitted infection, such as gonorrhea or chlamydia. Detorsion and surgical fixation (B) is the management of testicular torsion. In testicular torsion, the ultrasound shows a lack of blood flow to the testicle. Observation and supportive care (C) is the management for orchitis due to a self-limited cause, such as mumps. Mumps may cause orchitis but is more commonly associated with parotitis. Mumps may have a rash, but it is not palpable. Mumps is typically diagnosed in someone who has had an exposure.
Further Reading
References
- “UpToDate.” com, 2022, www.uptodate.com/contents/clinical-manifestations-and-diagnosis-of-polyarteritis-nodosa-in-adults?search=polyarteritis%20nodosa&source=search_result&selectedTitle=1~150&usage_type=default&display_rank=1. Accessed 21 July 2022.
- Ellen C. Ebert, Klaus D. Hagspiel, Michael Nagar, Naomi Schlesinger. Gastrointestinal Involvement in Polyarteritis Nodosa. Clinical Gastroenterology and Hepatology. 2008.
- Stanton M, Tiwari V. Polyarteritis Nodosa. [Updated 2022 May 1]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK482157/\
- https://rarediseases.info.nih.gov/diseases/7056/mononeuritis-multiplex
- https://www.msdmanuals.com/professional/musculoskeletal-and-connective-tissue-disorders/vasculitis/polyarteritis-nodosa-pan
- Pagnoux C, Seror R, Henegar C, Mahr A, Cohen P, Le Guern V, Bienvenu B, Mouthon L, Guillevin L., French Vasculitis Study Group. Clinical features and outcomes in 348 patients with polyarteritis nodosa: a systematic retrospective study of patients diagnosed between 1963 and 2005 and entered into the French Vasculitis Study Group Database. Arthritis Rheum. 2010 Feb;62(2):616-26
- https://www.uptodate.com/contents/treatment-and-prognosis-of-polyarteritis-nodosa?search=polyarteritis%20nodosa&source=search_result&selectedTitle=2~150&usage_type=default&display_rank=2#H1147024




