
Authors: Callyn Broyles, MD (EM Resident, University of Missouri-Columbia); Jessica Pelletier, DO, MHPE (APD/Assistant Professor of EM/Attending Physician, University of Missouri-Columbia) // Reviewed by: Sophia Görgens, MD (EM Physician, Yale University, CT); Cassandra Mackey, MD (Assistant Professor of Emergency Medicine, UMass Chan Medical School); Brit Long, MD (@long_brit)
Welcome to EM@3AM, an emDOCs series designed to foster your working knowledge by providing an expedited review of clinical basics. We’ll keep it short, while you keep that EM brain sharp.
A 34-year-old male presents to the ED about 30 minutes after he slipped on ice while shoveling snow at his house. He currently has a superficial abrasion approximately 6 cm by 6 cm to his posterior scalp without any laceration present that could be closed with sutures. The abrasion is profusely bleeding.
What is the next best strategy for managing this patient?
Answer: Topical Hemostatic Agents
Background:1
- Topical hemostatic agents are commonly used to help control bleeding when direct pressure or suturing isn’t sufficient or practical for the site.
- Each agent has unique properties that make it more effective in certain scenarios.
- They can establish hemostasis in different ways, including concentrating coagulation factors, bonding to the hemorrhaging tissues, or delivering procoagulant factors to the site.
- Hemorrhagic shock is the leading cause of mortality during combat and the second most common cause of death in trauma centers.
- Uncontrolled bleeding is a challenge that emergency medicine physicians need to have multiple tools in their arsenal that can be used to control the bleed based on the location and severity of the wound.
Types of Topical Hemostatic Agents:
- 3 main categories of hemostatic agents:2
- Factor concentrators
- Absorb water from blood to help concentrate platelets and clotting factors
- QuikClot Combat Gauze
- Mucoadhesive agents
- Adhere strongly to tissues to physically block blood flow
- HemCon, Surgicel, Surgifoam, Gelfoam, QuikClot
- Procoagulant supplements
- Deliver procoagulant factors to site of hemorrhage
- TXA, QuikClot
Common Hemostatic Agents in Emergency Departments
- Tranexamic acid (TXA)
- Antifibrinolytic –inhibits plasminogen from binding to fibrin to stop it from converting to plasmin, which is a clot-dissolving enzyme3
- Treatment with topical TXA is 3.5 times more likely to achieve bleeding cessation for acute epistaxis after the first application compared to other treatments, including nasal packing or topical vasoconstrictors3
- Lidocaine with epinephrine4
- Lidocaine with epinephrine injected into a wound can help constrict surrounding blood vessels
- The myth about not using lidocaine on fingers, toes, ears, nose, or penis comes from about 50 case reports of digital gangrene in the early 20th century5
- Careful analysis of each case did not support epinephrine as the cause
- The American Academy of Dermatology recommends the addition of epinephrine to local infiltration anesthesia for use on the ear, nose, hand, feet, and digits
- LET gel (4% lidocaine, epinephrine 1:2000, 0.5% tetracaine) also helps constrict blood vessels, but is applied topically
- Apply 1-3 ml directly to the wound (can use Tegaderm over top to hold in place)
- Keep on wound 15-30 min
- Primary benefit is for pain control but also helps bleeding
- LMX (4% lidocaine) and EMLA (2.5% lidocaine and 2.5% prilocaine)
- Topical anesthetic gels, not used for hemostasis, not to be used on broken skin
- The myth about not using lidocaine on fingers, toes, ears, nose, or penis comes from about 50 case reports of digital gangrene in the early 20th century5
- Lidocaine with epinephrine injected into a wound can help constrict surrounding blood vessels
- QuikClot® Combat Gauze6
- Generic: kaolin-impregnated hemostatic dressing
- Kaolin activates factor XII in the clotting process

- HemCon®6
- Generic: chitosan
- The positive charge of chitosan attracts the negatively charged RBCs and platelets helping create a seal over wounds (https://www.youtube.com/watch?v=hy8FtD_t7Ds)
- SURGICEL™6
- Generic: oxidized regenerated cellulose
- Acts as a physical barrier and forms a gel-like clot quickly through vasoconstriction and platelet aggregation (https://www.youtube.com/watch?v=nmXFONGfOlM&t=41s)

- SURGIFOAM™ or Gelfoam2
- Generic: absorbable gelatin sponge
- Similar mechanism to Surgicel
- Forms a physical barrier and soaks up the blood
- XSTAT7
- Generic: expandable hemostatic sponge
- Consists of multiple rapidly expanding cellulose mini-sponges (https://www.youtube.com/shorts/KFOMVZ6Pats)


Potential Uses and Evidence:
| Agent | Potential Uses | Evidence |
| HemCon | Best for relatively small, flat wounds due to its rigidity1 | Achieved hemostasis the quickest in dental bleeds compared to alternatives8 |
| QuikClot (Combat Gauze)6
|
Massive hemorrhage, arterial bleeds | Efficient hemostasis in severe hemorrhage from arteries, significant improvement in survival rates compared to control treatments |
| Surgicel6 | Wound dressings after bleeding is largely controlled | More effective for hemostasis compared to cotton gauze |
| Surgifoam*2 | Similar to Surgicel but available in different forms, like sponges and powder | Most evidence supports their use intraoperatively or postoperatively |
| TXA3 | Epistaxis, mucosal bleeding | Most likely to achieve hemostasis without rebleeding compared to other topical agents |
| XSTAT7 | Penetrating trauma (e.g. GSW, stab wound) | Outperformed gauze for hemorrhage control |
*Surgifoam is more commonly used in the OR rather than the ED.
How to Apply:
- Always start with direct, focal pressure for severe bleeding.
- Apply each directly to the wound and hold direct pressure for 3-5 minutes unless otherwise mentioned
- HemCon => 2×2 and 4×4 wafers6
- How to apply: chrome-extension://efaidnbmnnnibpcajpcglclefindmkaj/https://www.mermaidmedical.com/media/gcedavoo/mm-02-6000-04-eng-rev-03_hemcon.pdf
- Lidocaine with epinephrine4
- Can inject directly into wound
- LET gel (lidocaine, epinephrine, tetracaine)
- Apply to bleeding wound and cover with Tegaderm to ensure it stays in place
- Anesthetic effect will begin to work after about 20-30 minutes
- Also has a vasoconstrictive effect
- LMX (4% lidocaine)
- Also apply with Tegaderm to the area
- For non-disrupted skin
- QuikClot => many forms (4x4s, trauma pads, rolled dressings, Z-folded dressings)9
- How to apply: https://www.youtube.com/watch?v=KyJ5IEOffVQ&t=51s
- Surgicel => sizes from 0.5×2 to 4×8 cm6
- Surgifoam => sponges need cut to size of wound, can apply wet or dry2
- Can also make a slurry: https://www.youtube.com/watch?v=JQohHz_KH1Q
- TXA => soak gauze in TXA, then pack the bleeding area3
- Let sit for 20-30 minutes
- How to apply this for epistaxis: https://www.youtube.com/watch?v=ekGsM9CZSpY
- TXA may also be nebulized
- XSTAT => mini sponge dressing inserted into wounds where it expands to apply internal pressure to the source of bleeding9
- How to apply: https://www.youtube.com/watch?v=N3RM844Ezo4
Practical Tip:
- Most EDs carry topical TXA, QuikClot, Surgicel, and both injectable and topical lidocaine
- Check if your operating room carries the other topical hemostatic agents mentioned above!
- Apply direct pressure first with gauze while waiting for hemostatic material.
Pearls:
- If struggling to control bleeding from a site after direct pressure didn’t work, where you can’t apply a tourniquet or suture, consider topical hemostatic agents.
- Lidocaine with epinephrine and TXA-soaked gauze are good initial options for smaller bleeds.
- Use QuikClot first for massive
- Use TXA for mucosal bleeding as it’s biocompatible and adheres well to moist surfaces.
- Surgicel and Surgifoam are better used for localized, controlled bleeding.
- XSTAT can be helpful for bleeding due to gunshot wounds or stab wounds.

A 75-year-old woman with a history of pulmonary embolism on rivaroxaban therapy presents to the ED for persistent epistaxis for 6 hours. She reports no lightheadedness, palpitations, syncope, facial trauma, or recent procedures. Examination reveals bleeding from the Keisselbach plexus on the right. According to Hosseinialhashemi et al., if she is treated with topical tranexamic acid, which of the following is she less likely to experience?
A) ED length of stay > 2 hours
B) Need for intranasal phenylephrine
C) Rebleeding in 1–7 days
D) Tachycardia at discharge
Answer: A
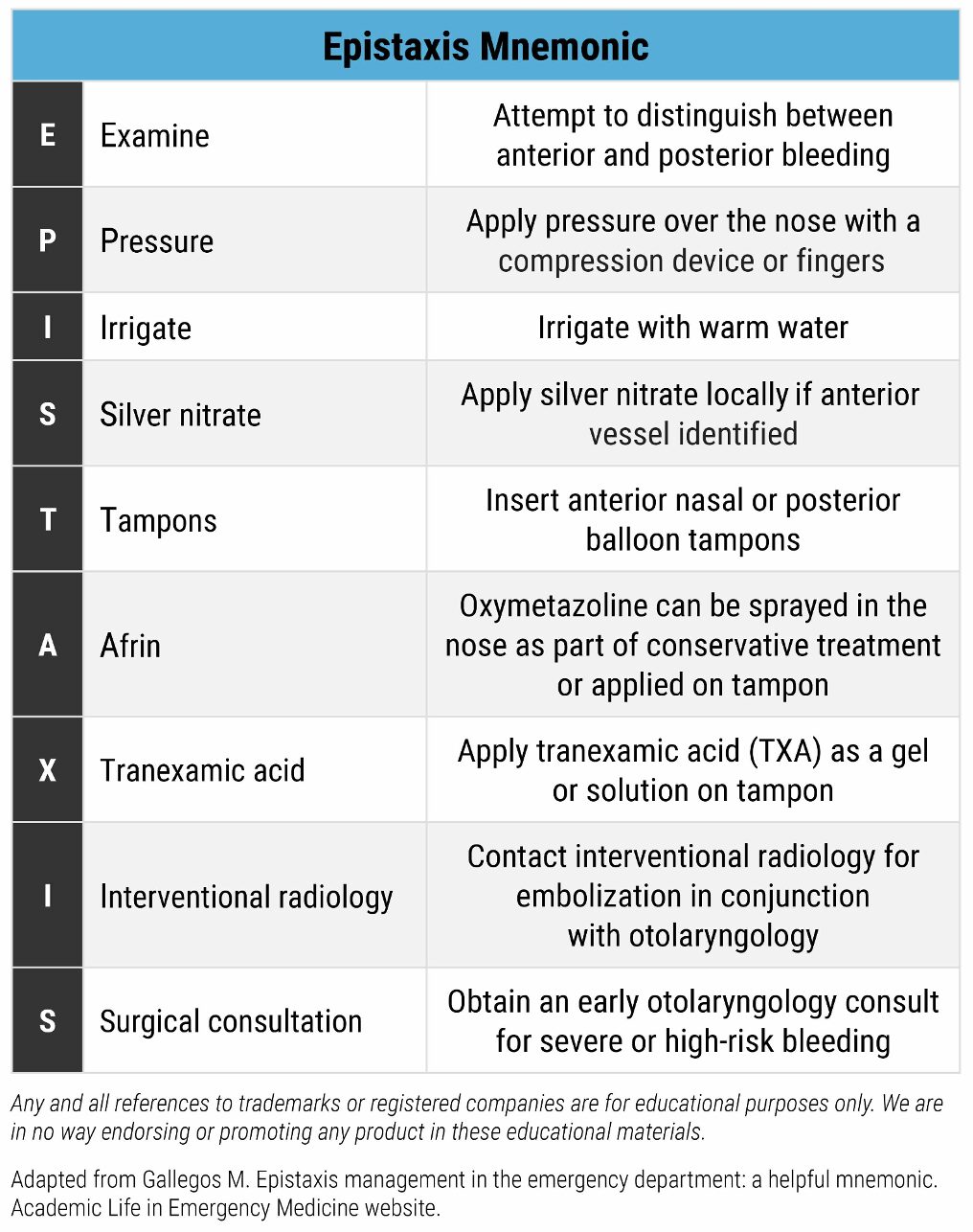
For anyone following the medical literature on topical tranexamic acid (TXA) for the treatment of epistaxis, the evidence can feel inconsistent, with studies showing mixed results over time. Epistaxis remains a common and sometimes challenging condition to manage, particularly without a structured approach or appropriate tools.
Most studies on topical TXA have focused on anterior epistaxis arising from the Kiesselbach plexus (Little’s area). Typical protocols involve applying TXA-soaked pledgets, though dosing has varied across trials, generally ranging from about 100 mg to 500 mg, with some studies using higher amounts.
A 2017 study by Zahed et al. compared topical TXA with standard anterior nasal packing using epinephrine and lidocaine. Patients receiving TXA had faster control of bleeding at 10 minutes, shorter ED stays, less rebleeding at 1 week, and higher satisfaction.
In contrast, the NoPAC trial (2017–2019, published 2021) found no significant difference between topical TXA and placebo for the primary outcome of need for nasal packing at discharge. Several factors may explain this discrepancy, including lower TXA dosing (around 200 mg), inclusion of posterior epistaxis, and enrollment of patients on anticoagulation, all of which may affect generalizability and outcomes.
A more recent trial by Hosseinialhashemi et al. (published 2022) used topical TXA at 100 mg/mL (1 mL applied) in combination with phenylephrine and lidocaine in a specialized ear, nose, and throat ED. This study showed reduced need for anterior nasal packing, shorter stays, and less rebleeding at 24 hours. However, anticoagulated patients were excluded, and many participants underwent cauterization, which may limit applicability to general emergency settings.
Overall, despite variability across studies, topical TXA remains a safe, inexpensive, and minimally invasive option for managing atraumatic anterior epistaxis in the ED, with evidence suggesting benefit in selected patient populations.
Need for intranasal phenylephrine (B) was not a measured outcome. Both groups in the study received phenylephrine as part of the treatment protocol (the control group received phenylephrine + lidocaine; the intervention group received tranexamic acid + phenylephrine + lidocaine).
Rebleeding in 1–7 days (C) was not measured. The benefit is shown mainly at 24 hours, not in the longer term.
Tachycardia at discharge (D) was not an outcome measure in the Hosseinialhashemi et al. study.
Further Reading
Further FOAMed:
- https://wikem.org/wiki/Hemostatic_agents
- https://www.nuemblog.com/blog/topical-hemostatics
- https://www.acep.org/siteassets/uploads/uploaded-files/acep/membership/sections-of-membership/tact/presentations/hemostaticagents.pdf
- https://www.emdocs.net/em3am-dental-bleeding
- https://www.tamingthesru.com/blog/2020/2/2/minor-care-series-management-of-epistaxis
References:
- Khoshmohabat H, Paydar S, Kazemi HM, Dalfardi B. Overview of Agents Used for Emergency Hemostasis. Trauma Mon. 2016;21(1). doi:10.5812/traumamon.26023
- Grissom TE, Fang R. Topical hemostatic agents and dressings in the prehospital setting. Curr Opin Anaesthesiol. 2015;28(2):210-216. doi:10.1097/ACO.0000000000000166
- Janapala RN, Tran QK, Patel J, Mehta E, Pourmand A. Efficacy of topical tranexamic acid in epistaxis: A systematic review and meta-analysis. Am J Emerg Med. 2022;51:169-175. doi:10.1016/j.ajem.2021.10.043
- Kundu S, Achar S. Principles of Office Anesthesia: Part II. Topical Anesthesia.
- Kouba DJ, LoPiccolo MC, Alam M, et al. Guidelines for the use of local anesthesia in office-based dermatologic surgery. J Am Acad Dermatol. 2016;74(6):1201-1219. doi:10.1016/j.jaad.2016.01.022
- Simpson A, Shukla A, Brown AC. Biomaterials for Hemostasis. Annu Rev Biomed Eng. 2022;24(1):111-135. doi:10.1146/annurev-bioeng-012521-101942
- Kragh JF, Aden JK, Steinbaugh J, Bullard M, Dubick MA. Gauze vs XSTAT in wound packing for hemorrhage control. Am J Emerg Med. 2015;33(7):974-976. doi:10.1016/j.ajem.2015.03.048
- Kale TP, Singh AK, Kotrashetti SM, Kapoor A. Effectiveness of Hemcon Dental Dressing versus Conventional Method of Haemostasis in 40 Patients on Oral Antiplatelet Drugs. Sultan Qaboos Univ Med J. 2012;12(3):330-335. doi:10.18295/2075-0528.1384
- Bennett BL. Bleeding Control Using Hemostatic Dressings: Lessons Learned. Wilderness Environ Med. 2017;28(2_suppl):S39-S49. doi:10.1016/j.wem.2016.12.005 https://www.jaad.org/article/S0190-9622%2816%2900074-8/fulltext




