Today on the emDocs cast with Brit Long, MD (@long_brit), Manpreet Singh, MD (@MprizzleER), and Rachel Bridwell, MD (@rebridwell)cover three posts: acute acalculous cholecystitis, mastitis and breast abscess, and LV aneurysm ECG findings.
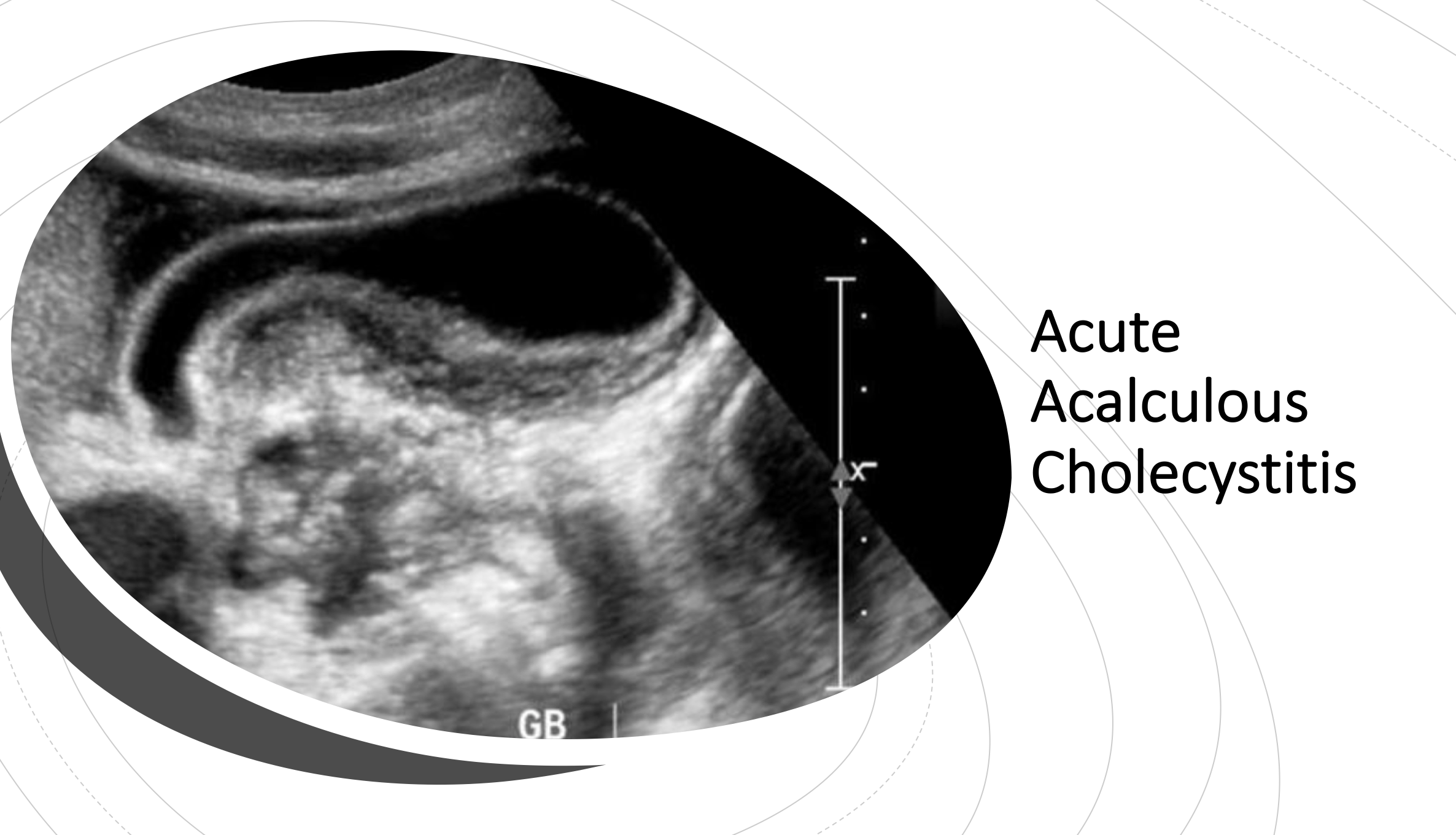
Part 1: Acute Acalculous Cholecystitis in Adults: ED Presentation, Evaluation, and Management
Key Points from the Podcast and Post:
- Acute acalculous cholecystitis (AAC) is due inflammation of the gallbladder without evidence of gallbladder calculi. AAC is commonly associated with critically ill patients in the ICU, i.e. polytrauma patients, massive burns, cardiac surgery, abdominal vascular surgery, immunosuppression, sepsis, prolonged TPN administration.
- AAC may have a higher incidence in outpatients than hospitalized, critically ill patients. Maintain a high index of suspicion in patients who present to the ED with right upper quadrant pain even in the absence of a history of cholelithiasis.
- Men > 60 years old with atherosclerotic cardiovascular disease are the most common outpatient population to develop AAC.
- The most common findings include right upper quadrant pain, fever, and leukocytosis.
- The sensitivity of ultrasound for acute acalculous cholecystitis is not well established. If you have a high clinical suspicion and a negative ultrasound, pursue further diagnostic imaging with HIDA scan +/- CT imaging, followed by admission for diagnostic laparoscopy if all noninvasive testing is negative.
- Acute acalculous cholecystitis follows a more fulminant course than calculous cholecystitis. Broad spectrum antibiotics with gram-negative coverage and fluid resuscitation should be started immediately if the diagnosis is suspected, with an emergent consultation to general surgery.
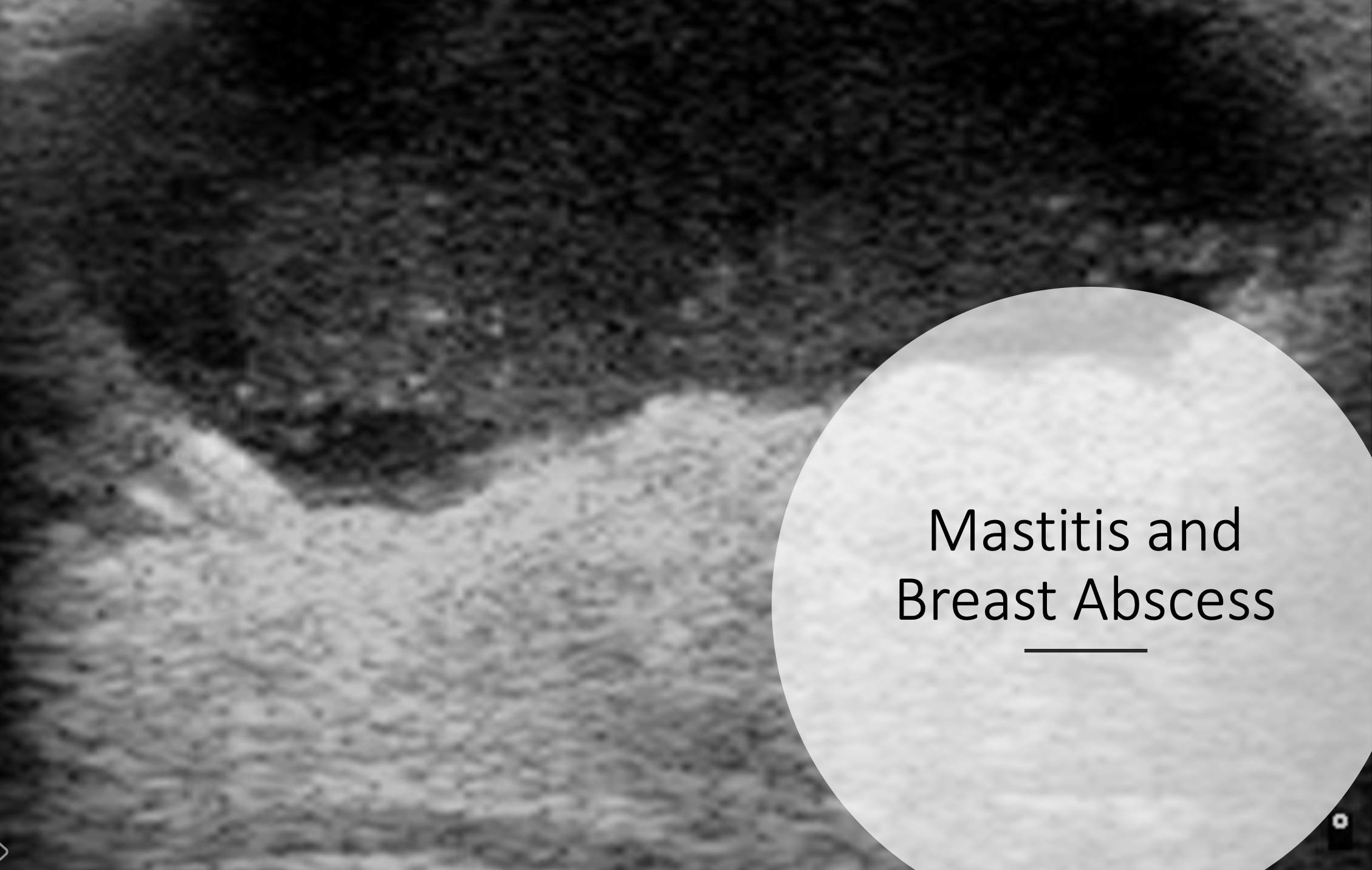
Part 2: Mastitis and Breast Abscess
Key Points from the Podcast and Post:
- Mastitis refers to erythema and edema of breast tissue PLUS systemic signs and symptoms.
- Mastitis can be categorized as puerperal (breastfeeding) vs. non-puerperal (not breast feeding).
- In patients that have non-puerperal mastitis, it is imperative to consider inflammatory breast cancer as a possibility.
- If patient has fever and responds to antibiotics, this is less likely.
- However, from the ED refer to breast surgery or breast radiology to ensure appropriate follow up if patient doesn’t respond to antibiotics.
- In the puerperal patient there is a spectrum from a plugged breast duct developing into mastitis developing into breast abscess.
- Early mastitis (<24 hours) counseling on effective milk drainage (increased feedings by infant in addition to pumping) can be considered prior to starting antibiotics.
- For either puerperal or non-puerperal mastitis.
- Antibiotics covering S. aureus should be initiated, such as dicloxacillin.
- If the patient has developed an abscess, general surgery and/or breast radiology should be consulted for drainage if these resources are available. If not and the abscess is uncomplicated, small and superficial the emergency physician can consider performing ultrasound guided needle aspiration.
- If the patient is hemodynamically stable with a breast abscess, she is safe for discharge with outpatient follow up with breast surgery or breast radiology for drainage but should be started on antibiotics from the ED.
Part 3: ECG Pointers –Post Myocardial Infarction Complications – LV Aneurysm
Key Points from the Podcast and Post:
- Acquiring an old ECG is key to differentiating LV aneurysm from anterior STEMI, with a T-wave amplitude:QRS amplitude assisting in differentiation.
- STEMI can be superimposed on LV aneurysm, and in this case the T-wave again becomes upright with higher amplitude.
- LV aneurysm patients are at very high risk of dysrhythmias and thromboembolic events.




