Today on the emDocs cast with Brit Long, MD (@long_brit) and Manpreet Singh, MD (@MprizzleER) we cover intraosseous access.
Indications
- Intraosseous access uses the medullary cavity within bones as a non-collapsible vein.
- Venous access for infusion of intravenous fluids and drugs, including vasoactive drugs.
- Diagnostic bone marrow aspiration.
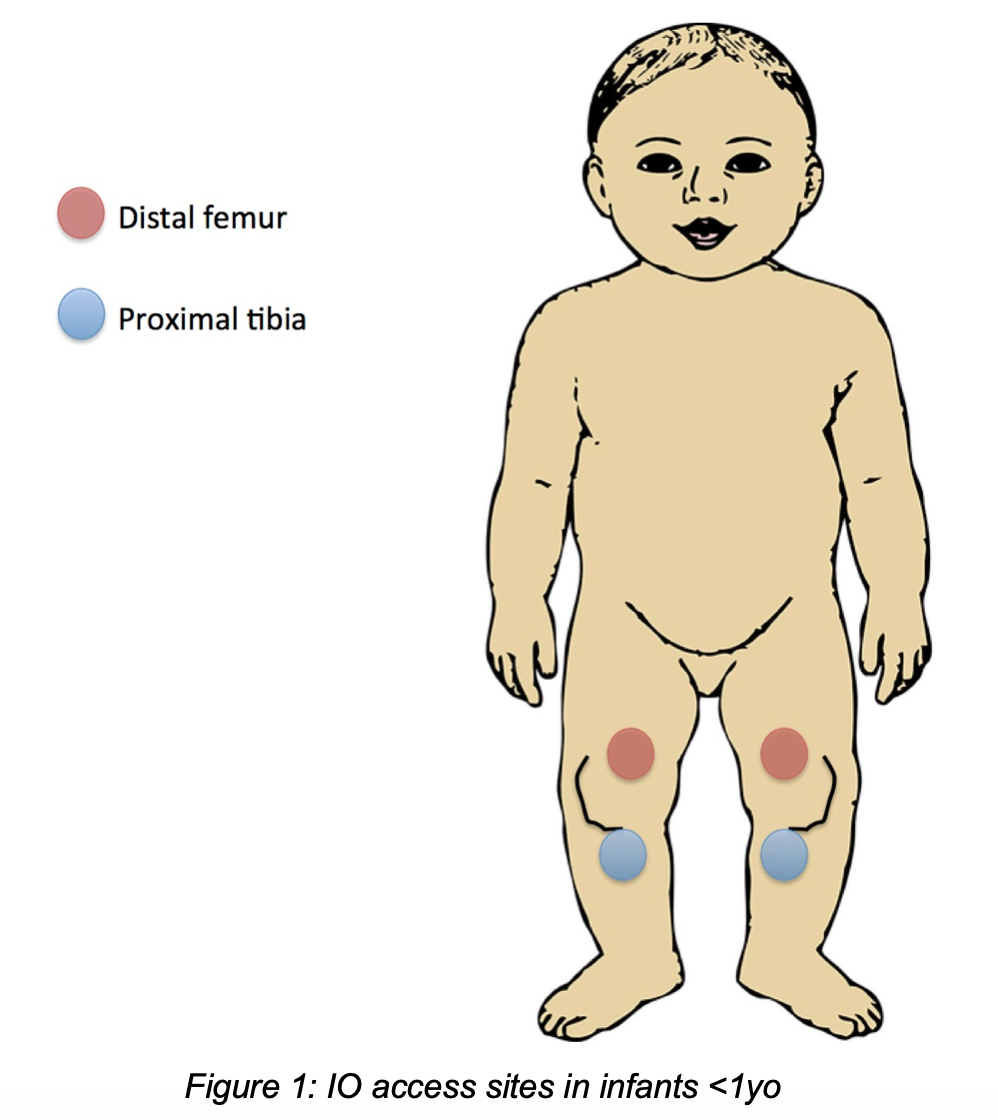
Sites
- Infants and children (<12y): in arrest or severe shock, if no easy IV access, place IO in distal femur (<1y), distal tibia/fibula (>1y), or proximal tibia (all).
- Adolescents and adults (>12yo): in arrest, severe shock, or conditions where IV access is difficult or impossible, place IO in proximal humerus (>18yo), proximal tibia, distal tibia/fibula, or sternum (all).


Rapid Procedure Review
- Position patient and site of interest.
- Palpate landmarks to determine insertion point; mark the skin.
- Don sterile gown and gloves, apply sterile drape, and sterilize site with antiseptic.
- (AWAKE ONLY) Anesthetize insertion tract with 2% lidocaine.
- Insert IO until bone resistance decreases suddenly.
- Remove stylet/trocar.
- Examine for correct placement (upright position + flush), attempt to aspirate bone marrow.
- (AWAKE ONLY) Slowly infuse 2% lidocaine for anesthesia.
- Flush IO with saline; palpate for infiltration; connect IV tubing.
- Secure IO with gauze/tape or dressing.
Pearls and Pitfalls
- Patients come in all shapes and sizes. If your patient has excessive subcutaneous or adipose tissue over your preferred site, you may have to choose an alternative site.
- Position for success! Make sure the extremity or site is visible, angled advantageously, and supported. Use bedrolls/sheets or fellow personnel to assist you with this.
- Avoid needlestick injuries! IO catheters and stylets/trocars are still sharps and can injure the proceduralist. Make sure your hand is not directly behind the insertion site, as a misplaced IO can bypass or completely penetrate the extremity and cause injury.
- It is very easy to forget to secure an IO during a busy resuscitation. Although they don’t slip out as easily as an IV, an IO can fall out, and if it does replacement likely needs to be in a different extremity to avoid infiltration. Tape down your IO securely!
- In a resuscitated patient, make sure that any IO access is clearly indicated and discussed with receiving providers during handoff. When receiving a resuscitated patient, examine carefully for the presence of an IO on the extremities or sternum.
- Anecdotally the proximal humerus is favored by many practitioners because of its theoretical faster infusion rates and utility in cases of abdominopelvic or lower extremity compromise. The proximal tibia is frequently easier to palpate and available in patients of all ages. You should feel comfortable inserting an IO in at least two different sites and should be familiar with all of them.




