Today on the emDOCs cast with Brit Long (@long_brit), we cover Part 1 on EBM updates in acute appendicitis in adults. This part evaluates history and exam findings, laboratory testing, and diagnostic scoring systems.
Episode 138: EBM Acute Appendicitis in Adults Part 1
Introduction:
- Abdominal pain is one of the most common chief complaints in the ED; right lower quadrant (RLQ) pain accounts for up to half of these visits (1-10).
- Appendicitis is the most common abdominal surgical emergency worldwide (3-10).
- Lifetime risk is 9% for males and 7% for females.
- Highest risk between 15-30 years (4,11).
- Perforation occurs in 16-40%; higher rates in pediatric and elderly patients (3,5).
- Mortality rate is less than 1% without perforation; increases up to 8% for perforation (3,8,10-12).
What history and exam findings are most suggestive of appendicitis in adults?
- Classic presentation of appendicitis is periumbilical pain that migrates to the RLQ with nausea, vomiting, and anorexia. Most common presenting symptom is abdominal pain. One study found 99% of adult patients had abdominal pain, followed by nausea (81.7%), anorexia (72.4%), emesis (67.7%), fever (44.9%), and chills (27.3%) (3,4,8,13,14).
- Systematic review: RLQ pain was the most frequent symptom (LR+ 7.31-8.46, LR- 0-0.28); migration of pain (LR+ 3.18, LR- 0.50) and pain prior to vomiting (LR+ 2.76) (14).
- Other findings: anorexia sensitivity 58-91% and specificity 37-40% (3,4,8,13,14), nausea or vomiting sensitivity 40-72% and specificity 45-69% (3,4,8,13,14), diarrhea sensitivity 9-24% and specificity 58-65% (13-17).
- Examination findings classically associated: McBurney’s point tenderness, Rovsing’s sign, Psoas sign, obturator sign.
- McBurney’s point: maximal tenderness 3-5 cm from the anterior superior iliac spine (ASIS) on a line from the ASIS to the umbilicus.
- Sensitivity of 50-96% and specificity 75-86%.
- Rovsing’s sig: RLQ pain with palpation of the left lower quadrant.
- Sensitivity 22-68% and specificity 58-96%
- Psoas sign: RLQ pain with passive right hip extension when the patient is lying on their left side.
- Sensitivity 13-42% and specificity 79-97%
- Obturator sign: flexion of the right hip and knee followed by internal rotation causes RLQ pain if the appendix lies on the right obturator internus.
- sensitivity 8% and specificity 94%
- A meta-analysis found abdominal rigidity (LR+ 3.76, LR- 0.82), rebound tenderness (LR+ 1.10-6.30, LR- 0-0.86), and psoas sign (LR+ 2.38, LR- 0.90) slightly increase the likelihood of appendicitis (14). Fever (LR+ 1.94, LR- 0.58) and guarding (LR+ 1.65-1.78, LR- 0-0.54) were not reliable (14).
- Atypical presentations: pregnant and elderly.
- Pregnancy: appendicitis is the most common non-obstetric surgical emergency during pregnancy.
- As the uterus enlarges during pregnancy, the abdominal wall expands and appendix moves cephalad. Pain may occur in the right flank or right upper quadrant (particularly in the late second or third trimester of pregnancy) (18,19).
- Elderly: appendicitis is more likely to be complicated or present with perforation (20-70%) (12).
- Less likely to present with fever and RLQ pain; may not develop peritonitis with perforation (12,20,21).
- Elderly patients have lower basal thermoregulatory temperature and thermoregulatory response, reduced pain perception with loss of spinal afferent innervation, and decreased abdominal wall musculature (12,20,21).
- Summary: Based on the literature, no one historical or physical examination finding can exclude the diagnosis of appendicitis.
- Presence of pain or tenderness in the RLQ, migrating pain, McBurney’s point tenderness, Rovsing’s sign, psoas sign, and obturator sign are suggestive.
- Pregnant and elderly patients more commonly present with atypical signs and symptoms.
- Pregnant patients may present with right upper quadrant pain, and elderly patients are less likely to have fever and RLQ pain.
- Pregnancy: appendicitis is the most common non-obstetric surgical emergency during pregnancy.
- McBurney’s point: maximal tenderness 3-5 cm from the anterior superior iliac spine (ASIS) on a line from the ASIS to the umbilicus.
What laboratory testing is recommended?
- Most guidelines recommend CBC and serum chemistry testing (pregnancy test in reproductive-aged females) (3,9,10).
- Over 70% have leukocytosis with neutrophil predominance.
- Leukocytosis usually occurs in the first 12 hours of symptom development Leukocytosis sensitivity over 83%; neutrophil predominance sensitivity over 85% (16,22-26).
- WBC (> 15 x 109/L) and neutrophilic predominance are more common in the setting of perforation (22-26).
- C-reactive protein (CRP) sensitivity for appendicitis over 75% using a threshold of 1.7 mg/dL (22).
- CRP elevates within 12-24 hours and peaks within 48 hours (3,4,23,24,27).
- Potential issue: specificities for WBC, neutrophil predominance, and CRP range between 25-63% (23,24).
- 2006 study found that elevated WBC had a specificity of 31.9%, elevated neutrophil percentage a specificity of 33.1%, and elevated CRP a specificity of 26.1% (23).
- Combining WBC, neutrophil predominance, and CRP elevation has sensitivity 95% when all three are elevated (4,23,24,27.
- There is currently no clearly defined CRP threshold that may be used to definitively diagnose or exclude appendicitis.
- Don’t be fooled by the urinalysis (UA). Up to 40% of patients with appendicitis have leukocytes on UA (28). Incorporate history and exam with the UA.
- Summary: WBC and inflammatory markers in isolation should not be used to exclude the diagnosis. Combination of normal WBC, normal neutrophil distribution, and normal CRP suggest appendicitis is less likely.
What diagnostic scoring systems are available in adults?
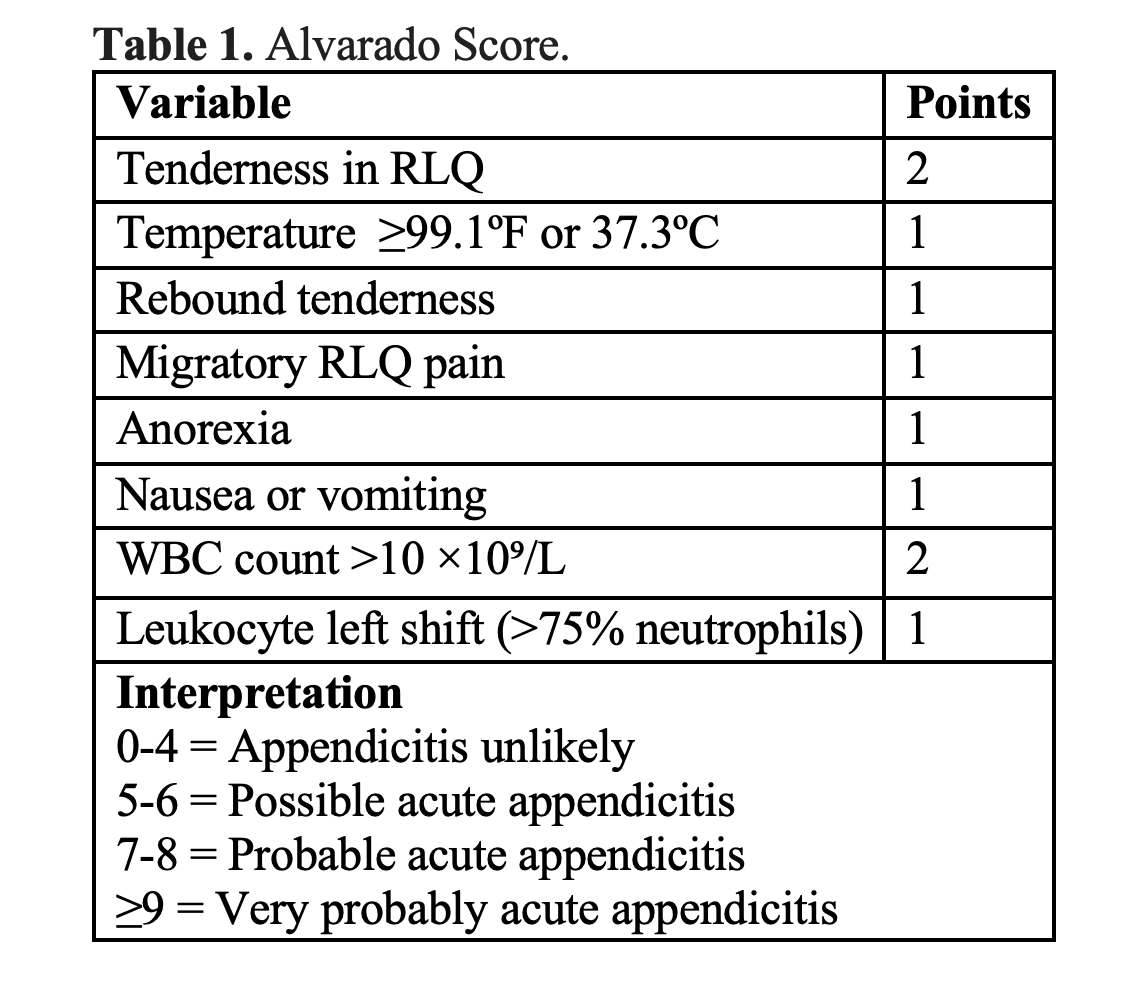
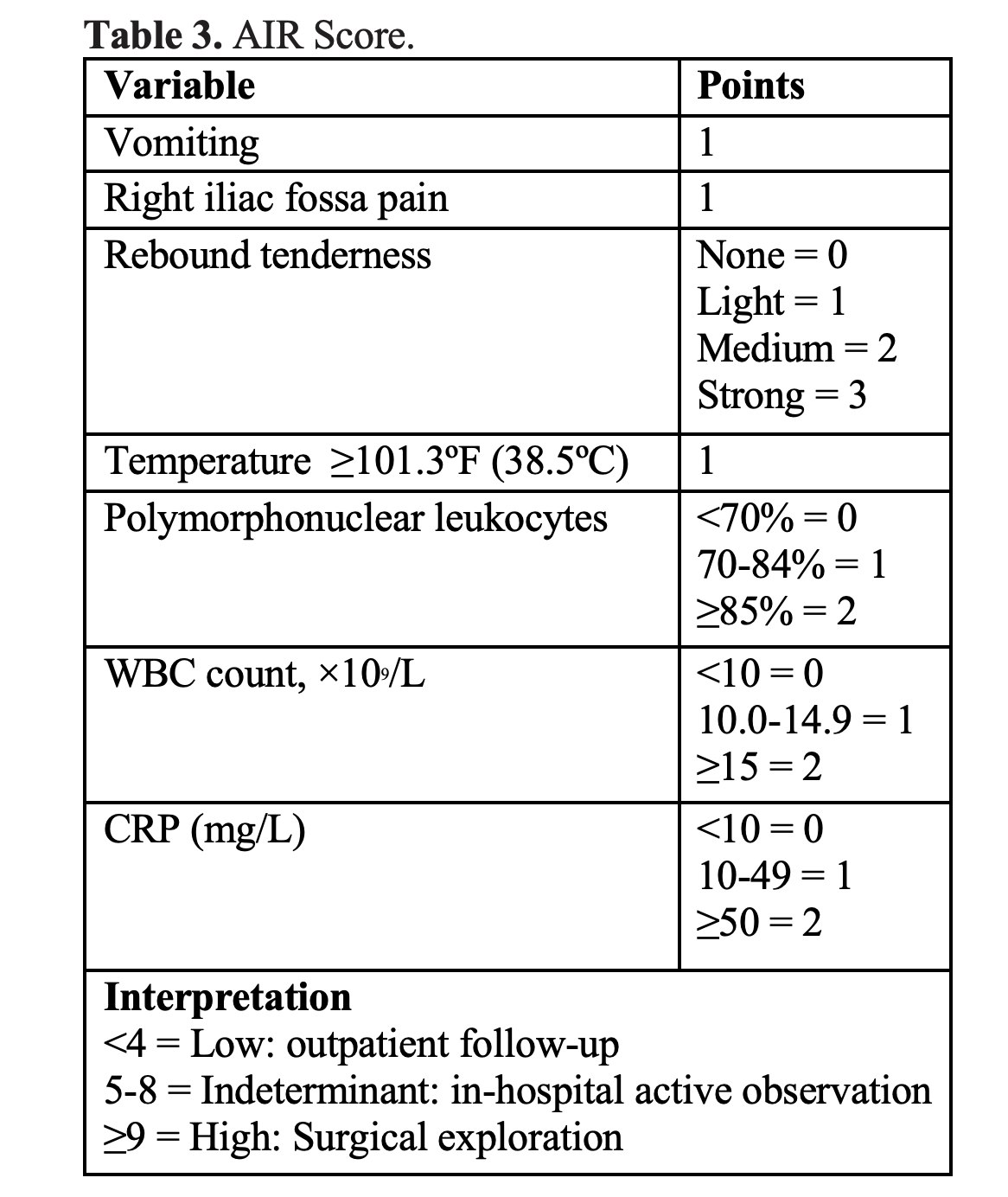
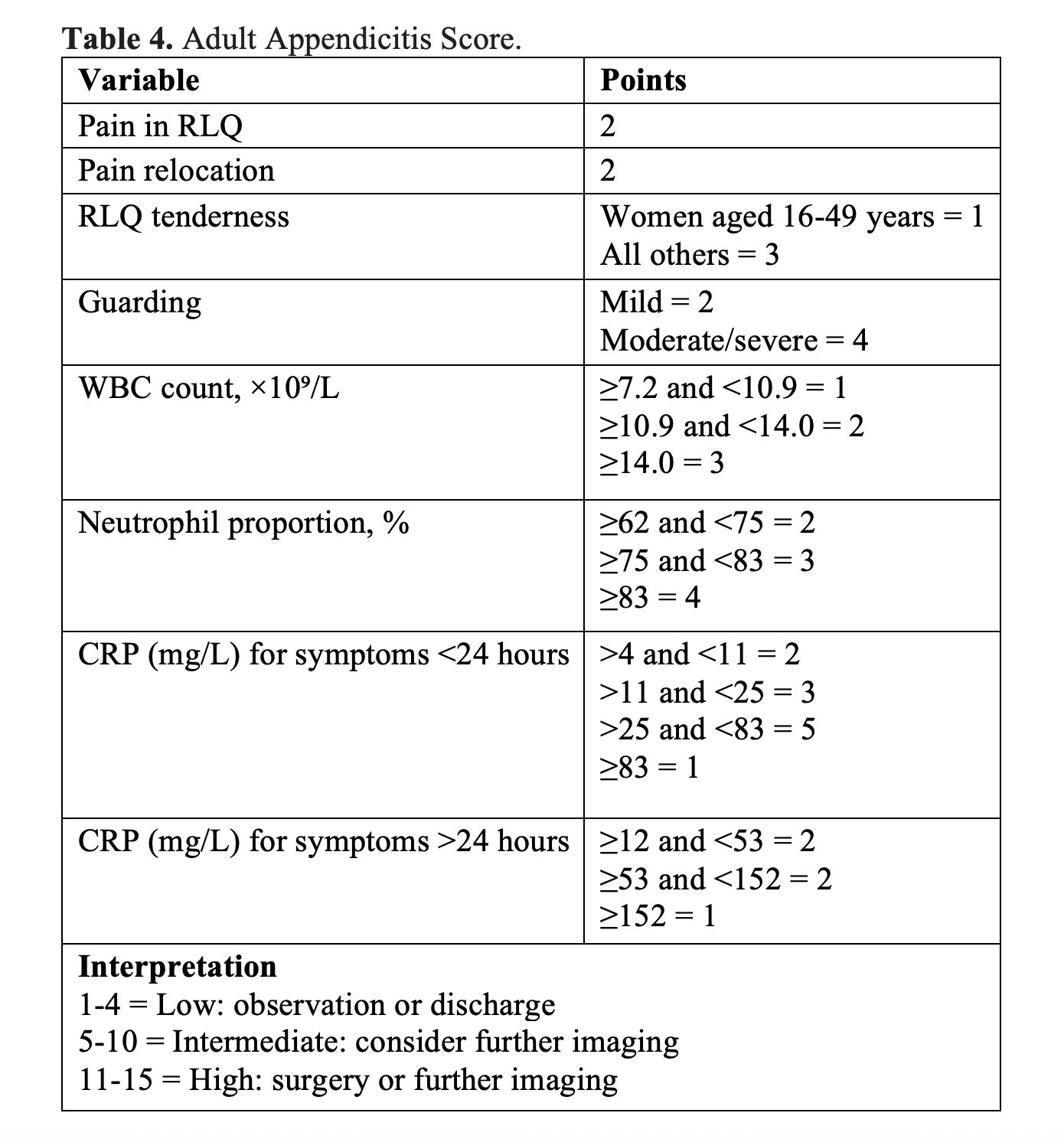
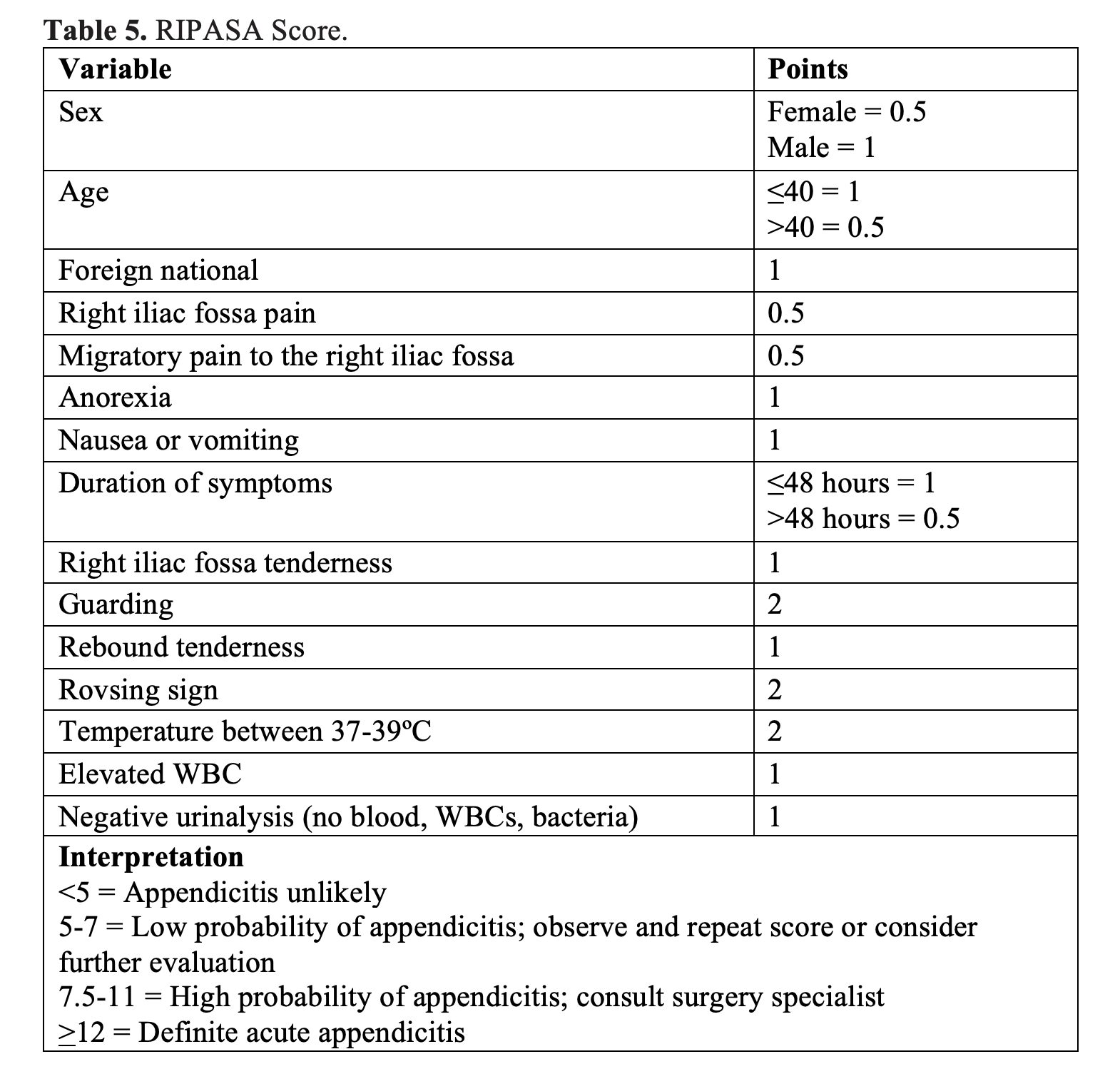
- Variety of diagnostic scoring systems available: Original and modified Alvarado score (Tables 1 and 2), the Appendicitis Inflammatory Response (AIR) score (Table 3), the Adult Appendicitis Score (AAS) (Table 4), and the Raja Isteri Pengiran Anak Saleha Appendicitis (RIPASA) score (Table 5) (3,9,25,26,29-36).
- Scores incorporate components of the history, physical examination, and laboratory testing to determine patients in whom imaging is recommended.

- Multiple studies have evaluated these scores.
- 2025 meta-analysis with 26 studies (15,699 participants) found the AIR score was more accurate than the Alvarado score; AIR AUROC curve 0.86 (95% CI 0.83 to 0.88) for all patients with appendicitis and 0.93 (95% CI 0.91 to 0.96) for complicated appendicitis. Alvarado score AUROC 0.79 (95% CI 0.76 to 0.81) for all patients and 0.88 (95% CI 0.82 to 0.95) for advanced cases (26). At > 3 points, sensitivity of AIR score was 0.95 (95% CI 0.90 to 0.97) for all patients with appendicitis and 0.99 (95% 0.97 to 0.99) for advanced appendicitis. At > 8 points, the specificity of the AIR score was 0.98 (95% CI 0.97 to 0.99) for all patients with appendicitis and 0.99 (95% CI 0.97 to 0.99) for advanced appendicitis (26).
- Meta-analysis of 33 articles comparing the Alvarado score and RIPASA score found the hierarchical summary receiver operating curve (HSROC) model for the Alvarado score had a summary sensitivity of 0.72 (95% CI 0.66 to 0.77) and summary specificity of 0.77 (95% CI 0.70 to 0.82) (34). For the RIPASA score, the HSROC model demonstrated a summary sensitivity of 0.95 (95% CI 0.92 to 0.97) and summary specificity of 0.71 (95% CI 0.60 to 0.80) (43).
- Guidelines incorporate these diagnostic scores.
- The Journal of Trauma and Acute Care Surgery Emergency General Surgery Algorithms Work Group states that the Alvarado score may be used to determine the need for confirmatory imaging, and the AIR score demonstrates the highest sensitivity and specificity (9).
- The World Society of Emergency Surgery (WSES) recommends using clinical scores to exclude acute appendicitis and identify intermediate-risk patients needing imaging (3).
- These guidelines recommend against using the Alvarado score to confirm the diagnosis, due to low specificity to diagnose acute appendicitis. It is also unreliable in differentiating uncomplicated from complicated appendicitis in elderly patients, and the score is less sensitive in patients with HIV (3).
- The WSES guidelines recommend using either the AIR or AAS score as clinical predictors of appendicitis, as they demonstrate the best clinical performance with the highest discriminating power in adults with suspected acute appendicitis (3). The AIR and AAS scores reduce negative appendectomy rates in low-risk patients and reduce the need for imaging and admission in low- and intermediate-risk patients (3).
- The WSES states that patients less than 40 years with high risk of appendicitis based on these scores warrant surgical consultation, and imaging may be avoided prior to diagnostic/therapeutic laparoscopy (3).
- Summary: The AIR, AAS, and RIPASA scores demonstrate the best clinical accuracy. In younger patients less than 40 years who are low risk, they may be used with shared decision-making to reduce the need for imaging. Guidelines also support their use. In those with scores who are not low risk, further diagnostic evaluation is recommended, and in those at high-risk based on clinical scores, consult the surgical specialist.
Stay tuned for part 2, where we cover imaging and management.
References:
- Morley EJ, Bracey A, Reiter M, et al. Association of Pain Location With Computed Tomography Abnormalities in Emergency Department Patients With Abdominal Pain. J Emerg Med 2020;59:485-90.
- Cervellin G, Mora R, Ticinesi A, et al. Epidemiology and outcomes of acute abdominal pain in a large urban Emergency Department: retrospective analysis of 5,340 cases. Ann Transl Med. 2016;4:362.
- Di Saverio S, Podda M, De Simone B, et al. Diagnosis and treatment of acute appendicitis: 2020 update of the WSES Jerusalem guidelines. World J Emerg Surg. 2020 Apr 15;15(1):27.
- Petroianu A. Diagnosis of acute appendicitis. Int J Surg. 2012;10(3):115-9.
- Livingston EH, Woodward WA, Sarosi GA, et al. Disconnect between incidence of nonperforated and perforated appendicitis: implications for pathophysiology and management. Ann Surg. 2007;245:886–92.
- Ilves I. Seasonal variations of acute appendicitis and nonspecific abdominal pain in Finland. WJG. 2014;20:4037.
- Viniol A, Keunecke C, Biroga T, et al. Studies of the symptom abdominal pain–a systematic review and meta-analysis. Fam Pract. 2014;31:517–29.
- Bhangu A, Søreide K, Di Saverio S, et al. Acute appendicitis: modern understanding of pathogenesis, diagnosis, and management [published correction appears in Lancet. 2017 Oct 14;390(10104):1736]. Lancet. 2015;386(10000):1278-1287.
- Diaz JJ, Napolitano L, Livingston DH, et al. Evidence-based, cost-effective management of acute appendicitis: An algorithm of the Journal of Trauma and Acute Care Surgery emergency general surgery algorithms work group. J Trauma Acute Care Surg. 2025 Mar 1;98(3):368-373.
- Kumar SS, Collings AT, Lamm R, et al. SAGES guideline for the diagnosis and treatment of appendicitis. Surg Endosc. 2024 Jun;38(6):2974-2994.
- Sartelli M, Baiocchi GL, Di Saverio S, et al. Prospective Observational Study on acute Appendicitis Worldwide (POSAW). World J Emerg Surg. 2018;13:19. Published 2018 Apr 16.
- Fugazzola P, Ceresoli M, Agnoletti V, et al. The SIFIPAC/WSES/SICG/SIMEU guidelines for diagnosis and treatment of acute appendicitis in the elderly (2019 edition). World J Emerg Surg. 2020;15(1):19.
- Lee SL, Walsh AJ, Ho HS. Computed tomography and ultrasonography do not improve and may delay the diagnosis and treatment of acute appendicitis. Arch Surg. 2001;136(5):556-562.
- Wagner JM, McKinney WP, Carpenter JL. Does this patient have appendicitis? JAMA. 1996 Nov 20;276(19):1589-94.
- Golledge J, Toms AP, Franklin IJ, et al. Assessment of peritonism in appendicitis. Ann R Coll Surg Engl. 1996;78(1):11-14.
- Andersson RE, Hugander AP, Ghazi SH, et al. Diagnostic value of disease history, clinical presentation, and inflammatory parameters of appendicitis. World J Surg. 1999;23(2):133-140.
- Lane R, Grabham J. A useful sign for the diagnosis of peritoneal irritation in the right iliac fossa. Ann R Coll Surg Engl. 1997;79(2):128-129.
- Tanrıdan Okcu N, Banlı Cesur İ, İrkörücü O. Acute appendicitis in pregnancy: 50 case series, maternal and neonatal outcomes. Gebelikte akut apandisit: 50 olgu serisi, maternal ve neonatal sonuçları. Ulus Travma Acil Cerrahi Derg. 2021;27(2):255-259.
- Franca Neto AH, Amorim MM, Nóbrega BM. Acute appendicitis in pregnancy: literature review. Rev Assoc Med Bras (1992). 2015;61(2):170-177.
- Lapsa S, Ozolins A, Strumfa I, Gardovskis J. Acute Appendicitis in the Elderly: A Literature Review on an Increasingly Frequent Surgical Problem. Geriatrics (Basel). 2021 Sep 18;6(3):93.
- Er S, Özden S, Turan UF, Özdemir E, Saylam B, Tez M. Differences in the Clinical Course of Acute Appendicitis in Geriatric Patient Groups. Bull Emerg Trauma. 2020;8(4):224-228.
- Khan MN, Davie E, Irshad K. The role of white cell count and C-reactive protein in the diagnosis of acute appendicitis. J Ayub Med Coll Abbottabad. 2004;16(3):17-19.
- Yang HR, Wang YC, Chung PK, et al. Laboratory tests in patients with acute appendicitis. ANZ J Surg. 2006 Jan-Feb;76(1-2):71-4.
- Yang HR, Wang YC, Chung PK, et al. Role of leukocyte count, neutrophil percentage, and C-reactive protein in the diagnosis of acute appendicitis in the elderly. Am Surg. 2005 Apr;71(4):344-7.
- Andersson M, Andersson RE. The appendicitis inflammatory response score: a tool for the diagnosis of acute appendicitis that outperforms the Alvarado score. World J Surg. 2008 Aug;32(8):1843-9.
- Andersson RE, Stark J. Diagnostic value of the appendicitis inflammatory response (AIR) score. A systematic review and meta-analysis. World J Emerg Surg. 2025 Feb 8;20(1):12.
- Chen KC, Arad A, Chen KC, et al. The clinical value of pathology tests and imaging study in the diagnosis of acute appendicitis. Postgrad Med J. 2016 Oct;92(1092):611-9.
- Baird DLH, Simillis C, Kontovounisios C, et al. Acute appendicitis. BMJ. 2017;357:j1703.
- Alvarado A. A practical score for the early diagnosis of acute appendicitis. Ann Emerg Med. 1986 May;15(5):557-64.
- Bolívar-Rodríguez MA, Osuna-Wong BA, Calderón-Alvarado AB, et al. ARTÍCULO ORIGINAL Análisis comparativo de escalas diagnósticas de apendicitis aguda: Alvarado, RIPASA y AIR [Comparative analysis of diagnostic scales of acute appendicitis: Alvarado, RIPASA and AIR]. Cir Cir. 2018;86(2):169-174.
- Ghali MS, Hasan S, Al-Yahri O, et al. Adult appendicitis score versus Alvarado score: A comparative study in the diagnosis of acute appendicitis. Surg Open Sci. 2023 Jul 20;14:96-102.
- Chong CF, Adi MI, Thien A, et al. Development of the RIPASA score: a new appendicitis scoring system for the diagnosis of acute appendicitis. Singapore Med J. 2010 Mar;51(3):220-5.
- Sulo SS, Al-Atrakchi HA. The Modified Alvarado Score versus Alvarado Score in the Diagnosis of Acute Appendicitis. Medical Journal of Babylon. 2019;16(3):203-206.
- Favara G, Maugeri A, Barchitta M, et al. Comparison of RIPASA and ALVARADO scores for risk assessment of acute appendicitis: A systematic review and meta-analysis. PLoS One. 2022 Sep 30;17(9):e0275427.z
- Frountzas M, Stergios K, Kopsini D, et al. Alvarado or RIPASA score for diagnosis of acute appendicitis? A meta-analysis of randomized trials. Int J Surg. 2018 Aug;56:307-314.
- https://www.appendicitisscore.com/
- Expert Panel on Gastrointestinal Imaging; Kambadakone AR, Santillan CS, Kim DH, et al. ACR Appropriateness Criteria® Right Lower Quadrant Pain: 2022 Update. J Am Coll Radiol. 2022 Nov;19(11S):S445-S461.
- Rud B, Vejborg TS, Rappeport ED, et al. Computed tomography for diagnosis of acute appendicitis in adults. Cochrane Database Syst Rev. 2019 Nov 19;2019(11):CD009977.
- Hlibczuk V, Dattaro JA, Jin Z, et al. Diagnostic accuracy of noncontrast computed tomography for appendicitis in adults: a systematic review. Ann Emerg Med 2010;55:51-59 e1.
- Kepner AM, Bacasnot JV, Stahlman BA. Intravenous contrast alone vs intravenous and oral contrast computed tomography for the diagnosis of appendicitis in adult ED patients. Am J Emerg Med. 2012;30(9):1765-1773.
- Paulson EK, Coursey CA. CT protocols for acute appendicitis: time for change. AJR Am J Roentgenol. 2009;193(5):1268-1271.
- Kim K, Kim YH, Kim SY, et al. Low-dose abdominal CT for evaluating suspected appendicitis. N Engl J Med. 2012;366(17):1596-1605.
- Sippola S, Virtanen J, Tammilehto V, et al. The accuracy of low-dose computed tomography protocol in patients with suspected acute appendicitis: the OPTICAP study. Ann Surg. 2018;1.




