Today on the emDOCs cast with Brit Long (@long_brit), we cover EBM updates concerning the imaging and management of adult appendicitis. See part 1 for history and exam findings, laboratory testing, and risk diagnostic scores.
Episode 139: EBM Acute Appendicitis in Adults Part 2
What imaging is recommended?
- Several imaging tests available for diagnosis. X-ray has poor sensitivity and specificity. Other options include CT, ultrasound, MRI.
- The American College of Radiology (ACR) Appropriateness Criteria:
- CT abdomen and pelvis with intravenous (IV) contrast is the recommended initial imaging for patients with RLQ pain, fever, and leukocytosis in the context of suspected appendicitis.
- CT is usually appropriate for patients with isolated RLQ pain (37).
- In those with RLQ with or without fever and leukocytosis, CT abdomen and pelvis without contrast, US, and MRI may also be appropriate (37).
- In pregnant women with suspected appendicitis, US abdomen or MRI abdomen and pelvis without IV contrast is usually appropriate, while US pelvis, CT abdomen and pelvis with IV contrast, and CT abdomen and pelvis without contrast may be appropriate (37).
- ACR recommendations are based on the high sensitivity, specificity, and diagnostic yield of CT for appendicitis and other conditions that may need surgical intervention.
- The Society of American Gastrointestinal and Endoscopic Surgeons (SAGE) guidelines state that US is a reasonable first line study due to its low cost and lack of radiation, but CT and MRI are the most definitive modalities (10).
- CT is a reliable imaging modality.
- Meta-analysis data demonstrate sensitivity of 96% and specificity over 93% for CT with IV contrast (38).
- CT without contrast accurate: systematic review of 7 studies found CT without contrast had a sensitivity of 92.7% and specificity 96.1% (39). 2019 Cochrane review found CT without IV contrast had a sensitivity of 91% and specificity of 93% (38).
- Data suggest oral and rectal contrast do not improve diagnostic yield (38,40,41). Cochrane review found a sensitivity of 89% for CT with oral contrast (38).
- Low-radiation protocols use 2-4 mSv versus the standard 8-10 mSv) (38,42).
- A single-center study evaluating 879 patients found no difference with low-dose versus standard-dose CT groups in sensitivity and specificity (42).
- OPTICAP trial found a low-dose protocol with IV contrast was not inferior for diagnostic accuracy compared to standard-dose protocol
- Cochrane review found similar sensitivity and specificity for low-dose and standard-dose CT (94% versus 95%) (38).
- CT findings: enlarged appendix (≥ 8-9 mm outer-to-outer diameter) with occluded lumen, periappendiceal fat stranding, wall thickening (> 3 mm), wall enhancement, and appendicolith (Figure 1) (37,44,45).

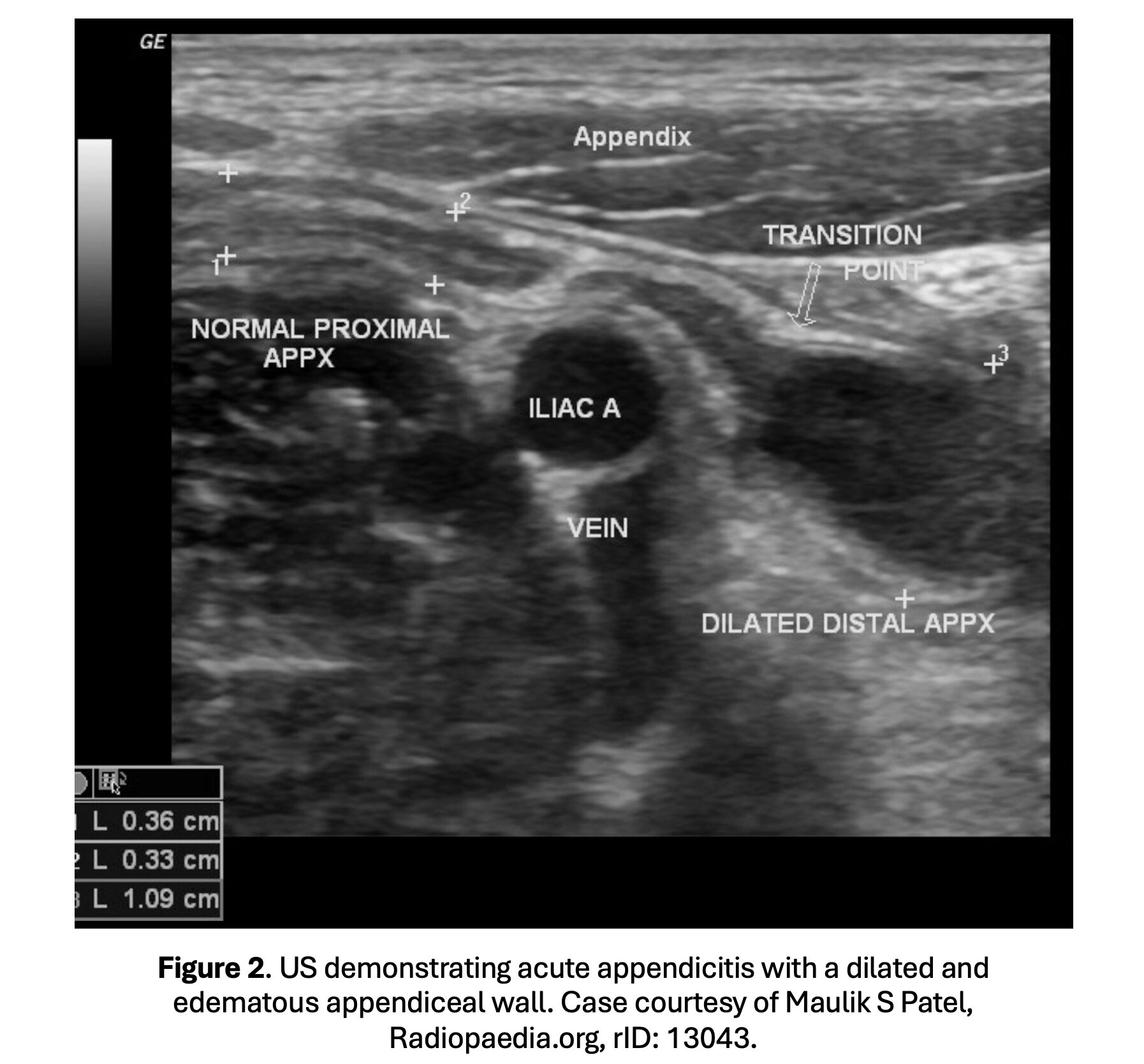
- Graded compression US has been evaluated in adults and is the first-line modality in pregnant women
- Sensitivity 21-96% and specificity 71-98% (46-57).
- Rates of non-visualization vary between 34-71%; indeterminate rates may reach 85% (52,53,58-60).
- Standardized results reporting improves US reliability for diagnosing of appendicitis (60).
- US is more likely to visualize the appendix in men, BMI < 22 mg/kg2, and more severe pain (50,52). Y
- US findings: noncompressible appendix with wall thickness > 6 mm, pain over the appendix with compression, hyperechoic appendicolith, increased echogenicity of periappendiceal fat, and fluid in the RLQ (Figure 2) (46-57).
- MRI is a third-line imaging modality
- This test is mostly used in pregnant women if US is unavailable or equivocal; MRI can also be used as a first-line imaging modality if available (61,62).
- Sensitivity is 85-98% and specificity is 97-99% for experienced radiologists; lower in less experienced readers (77-89% and 79-83%, respectively) (63-69).
- Non-diagnostic rate ranges between 20-40% (63-69).
- In pregnant patients, sensitivity ranges between 89-100% and specificity 93-99% (70-75).
- Imaging time is longer with MRI.
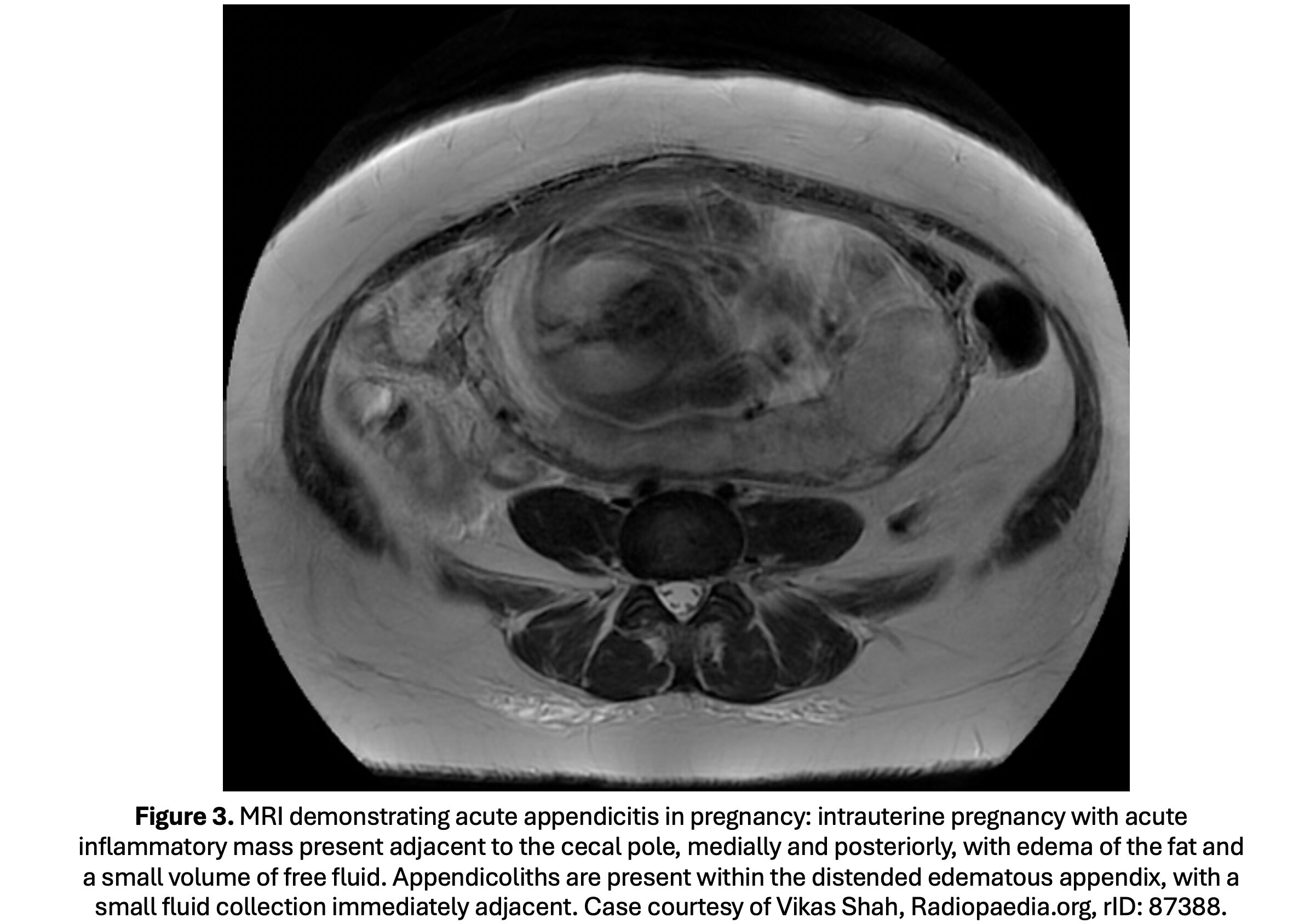
- MRI findings: fluid-filled, enlarged appendix (>7 mm) (Figure 3).
- Guidelines:
- See ACR discussion above (CT with IV contrast first-line imaging modality in adults with RLQ abdominal pain or for suspected appendicitis).
- WSES recommends using clinician pre-image likelihood of appendicitis in conjunction with scoring systems (3,37). In intermediate risk patients based on AIR/AAS/Alvarado score, US can used as a first-line imaging test. If the patient has persisting pain in the RLQ, obtain cross-sectional imaging like CT; use low-dose CT with IV contrast in those with suspected appendicitis when clinically appropriate. For MRI, the WSES guidelines state that while it is sensitive and specific for appendicitis during pregnancy, a negative or inconclusive MRI should not be used to exclude the diagnosis if there’s high clinical suspicion (3). In patients with concern for complicated appendicitis (perforation, phlegmon, abscess), or in elderly patients, obtain CT with IV contrast.
- Summary: Based on the available data and guidelines, several imaging modalities are available. In well-appearing, US can be used as a first-line imaging test. If US is unable to visualize the appendix or if the patient has evidence of sepsis, is elderly, or is critically ill, obtain CT, preferably with IV contrast, but oral contrast is not routinely needed. For pregnant patients, use US and MRI if possible.
What is the management?
- Consult surgery for all patients with acute appendicitis and administer IV antibiotics (76).
- Operative intervention necessary for patients with critical illness or those with emergent intervention.
- Stable patients with a perforation with phlegmon or abscess can be managed with IV antibiotics and image-guided drainage; early appendectomy is associated with worse outcomes in these patients (3,9). If the patient does not improve, appendectomy is needed (77).
- Previously all patients with appendicitis were treated with surgery and antibiotics, but nonoperative management with antibiotics alone in appropriately selected patients has literature support.
- Nonoperative management with antibiotics alone only for those with uncomplicated appendicitis; defined as those without abscess, appendiceal gangrene, perforation, sepsis, or hemodynamic instability (78-87).
- 2025 meta-analysis included six trials with 2101 participants published between 2011 to 2021 (1050 received antibiotics and 1051 underwent appendectomy). Within one year, 57 (5.4%) of the 1050 patients receiving non-operative management with antibiotics alone experienced a complication, versus 87 (8.3%) of the 1051 patients receiving appendectomy (OR 0.49; 95% CI 0.20 to 1.20) (87). At one year, 33.9% of the antibiotics alone group had undergone appendectomy. Those with appendicolith at preinterventional imaging undergoing nonoperative management had a higher rate of complications versus appendectomy (15.0% versus 6.3%; OR 2.82; 95% CI 1.11 to 7.18; risk difference 13.2%; 95% CI 2.3% to 24.2%). In patients randomized to antibiotics alone, 94 (48.7%) of 193 patients with an appendicolith underwent appendectomy within one year, compared with 262 (30.6%) of 857 patients without an appendicolith (87).
- Several guidelines support non-operative management with antibiotics in uncomplicated appendicitis: the Journal of Trauma and Acute Care Surgery Emergency General Surgery Work Group, American Association for the Surgery of Trauma (AAST), and WSES (3,9,88).
- The Eastern Association for the Surgery of Trauma does not make a recommendation for or against non-operative management with antibiotics-first versus surgery for acute uncomplicated appendicitis due to what they state are limitations in the current data (89).
- The 2024 SAGE guidelines recommend that patients with either uncomplicated or complicated appendicitis be managed operatively and not nonoperatively (10).
- The WSES recommends nonoperative management in uncomplicated appendicitis without appendicolith.
- The AAST states that a fecalith does not preclude nonoperative management, but there is a higher probability of requiring additional procedures (3,88).
- Consideration: most current literature used CT for diagnosis and to confirm uncomplicated appendicitis, and the studies used IV antibiotics for several days while the patient was admitted, followed by oral antibiotics for 7-10 days (3,90).
- The APPAC II trial included 583 patients with uncomplicated appendicitis and compared moxifloxacin 400 mg per os (PO) for 7 days versus ertapenem 1 g IV followed by levofloxacin 500 mg PO with metronidazole 500 mg PO three times per day for 5 days (91). Seven days of oral moxifloxacin failed to demonstrate non-inferiority. Secondary analysis found a slightly higher appendectomy rate in those who received oral antibiotic monotherapy, and noninferiority could not be demonstrated (92).
- 2025 nested trial randomized patients with appendicitis but no perforation waiting for surgery to either receive antibiotics or not receive them until induction in the OR (93). Authors found similar rates of perforation (8.3% versus 8.9%; difference 0.6%; 95% CI -2 to 3.2). For the secondary outcome, lower rate of surgical site infection rate in the antibiotic group (14 of 887 [1.6%]) versus the no-antibiotic group (28 of 886 [3.2%]; absolute difference 1.6 percentage points; 95% CI 0.2 to 3.0) (93).
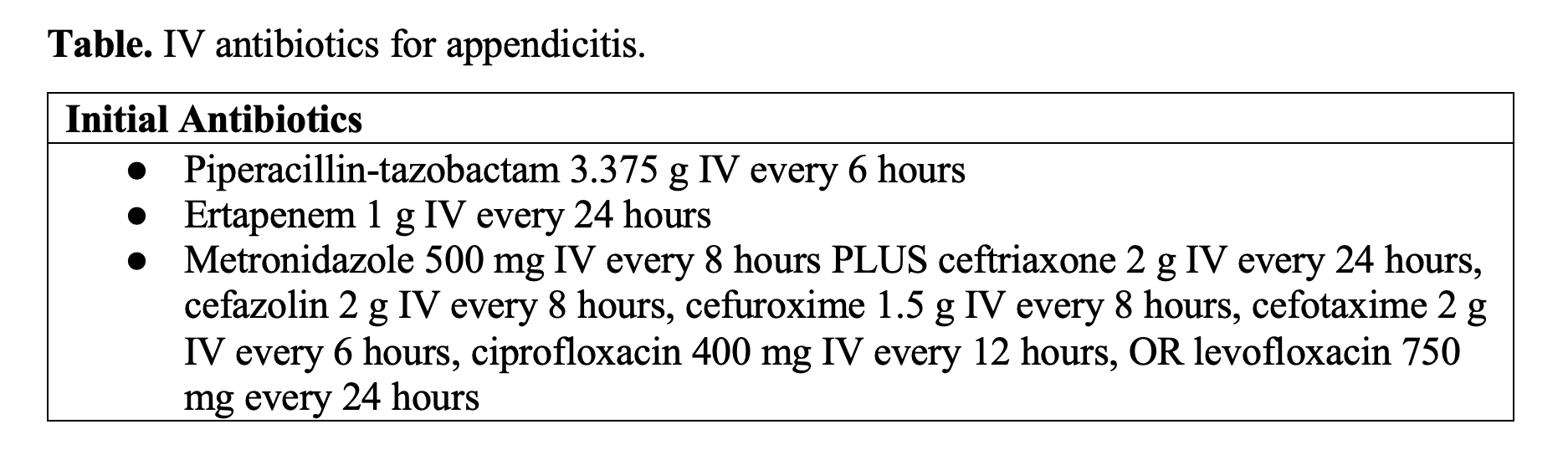
- For antibiotics, guidelines recommend using IV antibiotics initially, followed by transition to oral antibiotics based on the individual patient condition (3,9).
- Summary: Based on current evidence and guidelines, consult surgery and administer antibiotics for appendicitis. Non-operative management with antibiotics alone may be safe in select patients with uncomplicated appendicitis, particularly those without appendicolith.
- Caveats: Shared decision making is essential if using nonoperative management discussing possibility of failure and risk of complications (3). Non-operative management with antibiotics alone is not recommended in pregnant patients or elderly patients who are appropriate for surgery (3,94).
Summary:
- RLQ pain or tenderness, migrating pain, Rovsing’s sign, psoas sign, and obturator sign are suggestive of the diagnosis; no single finding in isolation can rule in or rule out the diagnosis.
- Combination of normal WBC, normal neutrophil distribution, and normal CRP suggest appendicitis is less likely.
- Current evidence demonstrates the highest diagnostic accuracy with AIR, AAS, and RIPASA.
- US or CT with IV contrast may be appropriate for the first-line imaging modality in adults, but use CT with IV contrast if concerned about a complication. For pregnancy, US and MRI are the recommended imaging tests.
- For treatment, consult surgery and administer antibiotics. Non-operative management with antibiotics alone may be safe in select patients with uncomplicated appendicitis with shared decision-making.
References:
- Morley EJ, Bracey A, Reiter M, et al. Association of Pain Location With Computed Tomography Abnormalities in Emergency Department Patients With Abdominal Pain. J Emerg Med 2020;59:485-90.
- Cervellin G, Mora R, Ticinesi A, et al. Epidemiology and outcomes of acute abdominal pain in a large urban Emergency Department: retrospective analysis of 5,340 cases. Ann Transl Med. 2016;4:362.
- Di Saverio S, Podda M, De Simone B, et al. Diagnosis and treatment of acute appendicitis: 2020 update of the WSES Jerusalem guidelines. World J Emerg Surg. 2020 Apr 15;15(1):27.
- Petroianu A. Diagnosis of acute appendicitis. Int J Surg. 2012;10(3):115-9.
- Livingston EH, Woodward WA, Sarosi GA, et al. Disconnect between incidence of nonperforated and perforated appendicitis: implications for pathophysiology and management. Ann Surg. 2007;245:886–92.
- Ilves I. Seasonal variations of acute appendicitis and nonspecific abdominal pain in Finland. WJG. 2014;20:4037.
- Viniol A, Keunecke C, Biroga T, et al. Studies of the symptom abdominal pain–a systematic review and meta-analysis. Fam Pract. 2014;31:517–29.
- Bhangu A, Søreide K, Di Saverio S, et al. Acute appendicitis: modern understanding of pathogenesis, diagnosis, and management [published correction appears in Lancet. 2017 Oct 14;390(10104):1736]. Lancet. 2015;386(10000):1278-1287.
- Diaz JJ, Napolitano L, Livingston DH, et al. Evidence-based, cost-effective management of acute appendicitis: An algorithm of the Journal of Trauma and Acute Care Surgery emergency general surgery algorithms work group. J Trauma Acute Care Surg. 2025 Mar 1;98(3):368-373.
- Kumar SS, Collings AT, Lamm R, et al. SAGES guideline for the diagnosis and treatment of appendicitis. Surg Endosc. 2024 Jun;38(6):2974-2994.
- Sartelli M, Baiocchi GL, Di Saverio S, et al. Prospective Observational Study on acute Appendicitis Worldwide (POSAW). World J Emerg Surg. 2018;13:19. Published 2018 Apr 16.
- Fugazzola P, Ceresoli M, Agnoletti V, et al. The SIFIPAC/WSES/SICG/SIMEU guidelines for diagnosis and treatment of acute appendicitis in the elderly (2019 edition). World J Emerg Surg. 2020;15(1):19.
- Lee SL, Walsh AJ, Ho HS. Computed tomography and ultrasonography do not improve and may delay the diagnosis and treatment of acute appendicitis. Arch Surg. 2001;136(5):556-562.
- Wagner JM, McKinney WP, Carpenter JL. Does this patient have appendicitis? JAMA. 1996 Nov 20;276(19):1589-94.
- Golledge J, Toms AP, Franklin IJ, et al. Assessment of peritonism in appendicitis. Ann R Coll Surg Engl. 1996;78(1):11-14.
- Andersson RE, Hugander AP, Ghazi SH, et al. Diagnostic value of disease history, clinical presentation, and inflammatory parameters of appendicitis. World J Surg. 1999;23(2):133-140.
- Lane R, Grabham J. A useful sign for the diagnosis of peritoneal irritation in the right iliac fossa. Ann R Coll Surg Engl. 1997;79(2):128-129.
- Tanrıdan Okcu N, Banlı Cesur İ, İrkörücü O. Acute appendicitis in pregnancy: 50 case series, maternal and neonatal outcomes. Gebelikte akut apandisit: 50 olgu serisi, maternal ve neonatal sonuçları. Ulus Travma Acil Cerrahi Derg. 2021;27(2):255-259.
- Franca Neto AH, Amorim MM, Nóbrega BM. Acute appendicitis in pregnancy: literature review. Rev Assoc Med Bras (1992). 2015;61(2):170-177.
- Lapsa S, Ozolins A, Strumfa I, Gardovskis J. Acute Appendicitis in the Elderly: A Literature Review on an Increasingly Frequent Surgical Problem. Geriatrics (Basel). 2021 Sep 18;6(3):93.
- Er S, Özden S, Turan UF, Özdemir E, Saylam B, Tez M. Differences in the Clinical Course of Acute Appendicitis in Geriatric Patient Groups. Bull Emerg Trauma. 2020;8(4):224-228.
- Khan MN, Davie E, Irshad K. The role of white cell count and C-reactive protein in the diagnosis of acute appendicitis. J Ayub Med Coll Abbottabad. 2004;16(3):17-19.
- Yang HR, Wang YC, Chung PK, et al. Laboratory tests in patients with acute appendicitis. ANZ J Surg. 2006 Jan-Feb;76(1-2):71-4.
- Yang HR, Wang YC, Chung PK, et al. Role of leukocyte count, neutrophil percentage, and C-reactive protein in the diagnosis of acute appendicitis in the elderly. Am Surg. 2005 Apr;71(4):344-7.
- Andersson M, Andersson RE. The appendicitis inflammatory response score: a tool for the diagnosis of acute appendicitis that outperforms the Alvarado score. World J Surg. 2008 Aug;32(8):1843-9.
- Andersson RE, Stark J. Diagnostic value of the appendicitis inflammatory response (AIR) score. A systematic review and meta-analysis. World J Emerg Surg. 2025 Feb 8;20(1):12.
- Chen KC, Arad A, Chen KC, et al. The clinical value of pathology tests and imaging study in the diagnosis of acute appendicitis. Postgrad Med J. 2016 Oct;92(1092):611-9.
- Baird DLH, Simillis C, Kontovounisios C, et al. Acute appendicitis. BMJ. 2017;357:j1703.
- Alvarado A. A practical score for the early diagnosis of acute appendicitis. Ann Emerg Med. 1986 May;15(5):557-64.
- Bolívar-Rodríguez MA, Osuna-Wong BA, Calderón-Alvarado AB, et al. ARTÍCULO ORIGINAL Análisis comparativo de escalas diagnósticas de apendicitis aguda: Alvarado, RIPASA y AIR [Comparative analysis of diagnostic scales of acute appendicitis: Alvarado, RIPASA and AIR]. Cir Cir. 2018;86(2):169-174.
- Ghali MS, Hasan S, Al-Yahri O, et al. Adult appendicitis score versus Alvarado score: A comparative study in the diagnosis of acute appendicitis. Surg Open Sci. 2023 Jul 20;14:96-102.
- Chong CF, Adi MI, Thien A, et al. Development of the RIPASA score: a new appendicitis scoring system for the diagnosis of acute appendicitis. Singapore Med J. 2010 Mar;51(3):220-5.
- Sulo SS, Al-Atrakchi HA. The Modified Alvarado Score versus Alvarado Score in the Diagnosis of Acute Appendicitis. Medical Journal of Babylon. 2019;16(3):203-206.
- Favara G, Maugeri A, Barchitta M, et al. Comparison of RIPASA and ALVARADO scores for risk assessment of acute appendicitis: A systematic review and meta-analysis. PLoS One. 2022 Sep 30;17(9):e0275427.z
- Frountzas M, Stergios K, Kopsini D, et al. Alvarado or RIPASA score for diagnosis of acute appendicitis? A meta-analysis of randomized trials. Int J Surg. 2018 Aug;56:307-314.
- https://www.appendicitisscore.com/
- Expert Panel on Gastrointestinal Imaging; Kambadakone AR, Santillan CS, Kim DH, et al. ACR Appropriateness Criteria® Right Lower Quadrant Pain: 2022 Update. J Am Coll Radiol. 2022 Nov;19(11S):S445-S461.
- Rud B, Vejborg TS, Rappeport ED, et al. Computed tomography for diagnosis of acute appendicitis in adults. Cochrane Database Syst Rev. 2019 Nov 19;2019(11):CD009977.
- Hlibczuk V, Dattaro JA, Jin Z, et al. Diagnostic accuracy of noncontrast computed tomography for appendicitis in adults: a systematic review. Ann Emerg Med 2010;55:51-59 e1.
- Kepner AM, Bacasnot JV, Stahlman BA. Intravenous contrast alone vs intravenous and oral contrast computed tomography for the diagnosis of appendicitis in adult ED patients. Am J Emerg Med. 2012;30(9):1765-1773.
- Paulson EK, Coursey CA. CT protocols for acute appendicitis: time for change. AJR Am J Roentgenol. 2009;193(5):1268-1271.
- Kim K, Kim YH, Kim SY, et al. Low-dose abdominal CT for evaluating suspected appendicitis. N Engl J Med. 2012;366(17):1596-1605.
- Sippola S, Virtanen J, Tammilehto V, et al. The accuracy of low-dose computed tomography protocol in patients with suspected acute appendicitis: the OPTICAP study. Ann Surg. 2018;1.
- Ives E, Sung S, McCue P, Durrani H, Halpern E. Independent Predictors of Acute Appendicitis on CT with Pathologic Correlation. Acad Radiol. 2008;15(8):996-1003.
- Cho J, Akers M, Siavoshi M, et al. Features on Computed Tomography That Correlate With Acute Appendicitis. Am Surg. 2023;89(6):2876-9
- Sezer TO, Gulece B, Zalluhoglu N, et al. Diagnostic value of ultrasonography in appendicitis. Adv Clin Exp Med 2012;21:633-6.
- Hasani SA, Fathi M, Daadpey M, et al. Accuracy of bedside emergency physician performed ultrasound in diagnosing different causes of acute abdominal pain: a prospective study. Clin Imaging 2015;39:476-9.
- Eng KA, Abadeh A, Ligocki C, et al. Acute Appendicitis: A Meta-Analysis of the Diagnostic Accuracy of US, CT, and MRI as Second-Line Imaging Tests after an Initial US. Radiology 2018;288:717-27.
- Piyarom P, Kaewlai R. False-negative appendicitis at ultrasound: nature and association. Ultrasound Med Biol 2014;40:1483-9.
- Al-Ajerami Y. Sensitivity and specificity of ultrasound in the diagnosis of acute appendicitis. East Mediterr Health J 2012;18:66-9.
- Boonstra PA, van Veen RN, Stockmann HB. Less negative appendectomies due to imaging in patients with suspected appendicitis. Surg Endosc 2015;29:2365-70.
- Kaewlai R, Lertlumsakulsub W, Srichareon P. Body mass index, pain score and Alvarado score are useful predictors of appendix visualization at ultrasound in adults. Ultrasound Med Biol 2015;41:1605-11.
- Lourenco P, Brown J, Leipsic J, Hague C. The current utility of ultrasound in the diagnosis of acute appendicitis. Clin Imaging 2016;40:944-8.
- Stewart JK, Olcott EW, Jeffrey RB. Sonography for appendicitis: nonvisualization of the appendix is an indication for active clinical observation rather than direct referral for computed tomography. J Clin Ultrasound 2012;40:455-61.
- Shen G, Wang J, Fei F, et al. Bedside ultrasonography for acute appendicitis: An updated diagnostic meta-analysis. Int J Surg 2019;70:1-9.
- Chang ST, Jeffrey RB, Olcott EW. Three-step sequential positioning algorithm during sonographic evaluation for appendicitis increases appendiceal visualization rate and reduces CT use. Am J Roentgenol. 2014;203:1006–12.
- Matthew Fields J, Davis J, Alsup C, et al. Accuracy of point-of-care ultrasonography for diagnosing acute appendicitis: a systematic review and meta analysis. Acad Emerg Med. 2017;24:1124–36.
- Segev L, Segev Y, Rayman S, et al. The diagnostic performance of ultrasound for acute appendicitis in pregnant and young nonpregnant women: a case-control study. Int J Surg. 2016;34:81–5.
- Lehnert BE, Gross JA, Linnau KF, et al. Utility of ultrasound for evaluating the appendix during the second and third trimester of pregnancy. Emerg Radiol. 2012;19:293–9.
- Sola R, Theut SB, Sinclair KA, et al. Standardized reporting of appendicitisrelated findings improves reliability of ultrasound in diagnosing appendicitis in children. J Pediatric Surg. 2018;53:984–7.
- Garcia EM, Camacho MA, Karolyi DR, et al. ACR Appropriateness Criteria® Right Lower Quadrant Pain-Suspected Appendicitis. J Am Coll Radiol. 2018;15:S373–87.
- Amitai MM, Katorza E, Guranda L, et al. Role of emergency magnetic resonance imaging for the workup of suspected appendicitis in pregnant women. Isr Med Assoc J. 2016;18:600–4.
- Blumenfeld YJ, Wong AE, Jafari A, et al. MR imaging in cases of antenatal suspected appendicitis – a meta-analysis. J Mate Fetal Neonat Med. 2011;24:485–8.
- Heverhagen JT, Pfestroff K, Heverhagen AE, et al. Diagnostic accuracy of magnetic resonance imaging: a prospective evaluation of patients with suspected appendicitis (diamond). J Magn Reson Imaging 2012;35:617-23.
- Inoue A, Furukawa A, Nitta N, et al. Accuracy, criteria, and clinical significance of visual assessment on diffusion-weighted imaging and apparent diffusion coefficient quantification for diagnosing acute appendicitis. Abdom Radiol (NY) 2019;44:3235-45.
- Petkovska I, Martin DR, Covington MF, et al. Accuracy of Unenhanced MR Imaging in the Detection of Acute Appendicitis: Single-Institution Clinical Performance Review. Radiology. 2016;279:451-60.
- Byott S, Harris I. Rapid acquisition axial and coronal T2 HASTE MR in the evaluation of acute abdominal pain. Eur J Radiol 2016;85:286-90.
- Leeuwenburgh MM, Wiarda BM, Wiezer MJ, et al. Comparison of imaging strategies with conditional contrast-enhanced CT and unenhanced MR imaging in patients suspected of having appendicitis: a multicenter diagnostic performance study. Radiology 2013;268:135-43.
- Duke E, Kalb B, Arif-Tiwari H, et al. A Systematic Review and Meta-Analysis of Diagnostic Performance of MRI for Evaluation of Acute Appendicitis. AJR Am J Roentgenol 2016;206:508-17.
- Ramalingam V, LeBedis C, Kelly JR, et al. Evaluation of a sequential multi-modality imaging algorithm for the diagnosis of acute appendicitis in the pregnant female. Emerg Radiol 2015;22:125-32.
- Burke LM, Bashir MR, Miller FH, et al. Magnetic resonance imaging of acute appendicitis in pregnancy: a 5-year multiinstitutional study. Am J Obstet Gynecol 2015;213:693 e1-6.
- Theilen LH, Mellnick VM, Longman RE, et al. Utility of magnetic resonance imaging for suspected appendicitis in pregnant women. Am J Obstet Gynecol 2015;212:345 e1-6.
- Konrad J, Grand D, Lourenco A. MRI: first-line imaging modality for pregnant patients with suspected appendicitis. Abdom Imaging 2015;40:3359-64.
- Rapp EJ, Naim F, Kadivar K, et al. Integrating MR imaging into the clinical workup of pregnant patients suspected of having appendicitis is associated with a lower negative laparotomy rate: single-institution study. Radiology 2013;267:137-44.
- American College of Radiology. ACR Committee on MR Safety. ACR Manual on MR Safety. Version 1.0. Available at: https://www.acr.org/-/media/ACR/Files/Radiology-Safety/MR-Safety/Manual-on-MR-Safety.pdf. Accessed March 31, 2022.
- Bratzler DW, Dellinger EP, Olsen KM, et al. Clinical practice guidelines for antimicrobial prophylaxis in surgery. Am J Health Syst Pharm. 2013;70(3):195-283. doi:10.2146/ajhp120568
- Gorter RR, Eker HH, Gorter-Stam MA, et al. Diagnosis and management of acute appendicitis. EAES consensus development conference 2015. Surg Endosc. 2016;30(11):4668-4690.
- Podda M, Gerardi C, Cillara N, et al. Antibiotic treatment and appendectomy for uncomplicated acute appendicitis in adults and children: a systematic review and meta-analysis. Ann Surg. 2019;270:1028–40.
- Harnoss JC, Zelienka I, Probst P, et al. Antibiotics Versus Surgical Therapy for Uncomplicated Appendicitis: Systematic Review and Meta-analysis of Controlled Trials (PROSPERO 2015: CRD42015016882). Ann Surg. 2017;265(5):889-900.
- Salminen P, Paajanen H, Rautio T, et al. Antibiotic Therapy vs Appendectomy for Treatment of Uncomplicated Acute Appendicitis: The APPAC Randomized Clinical Trial. JAMA. 2015;313(23):2340-2348.
- Huston JM, Kao LS, Chang PK, et al. Antibiotics vs. appendectomy for acute uncomplicated appendicitis in adults: review of the evidence and future directions. Surg Infect. 2017;18:527–35.
- Vons C, Barry C, Maitre S, et al. Amoxicillin plus clavulanic acid versus appendicectomy for treatment of acute uncomplicated appendicitis: an open-label, non-inferiority, randomised controlled trial. Lancet. 2011 May 7;377(9777):1573-9.
- Talan DA, Saltzman DJ, Mower WR, et al; Olive View–UCLA Appendicitis Study Group. Antibiotics-First Versus Surgery for Appendicitis: A US Pilot Randomized Controlled Trial Allowing Outpatient Antibiotic Management. Ann Emerg Med. 2017 Jul;70(1):1-11.e9.
- O’Leary DP, Walsh SM, Bolger J, et al. A Randomized Clinical Trial Evaluating the Efficacy and Quality of Life of Antibiotic-only Treatment of Acute Uncomplicated Appendicitis: Results of the COMMA Trial. Ann Surg. 2021 Aug 1;274(2):240-247.
- Ceresoli M, Pisano M, Allievi N, et al. Never put equipoise in appendix! Final results of ASAA (antibiotics vs. surgery for uncomplicated acute appendicitis in adults) randomized controlled trial. Updates Surg. 2019 Jun;71(2):381-387.
- CODA Collaborative; Davidson GH, Flum DR, Monsell SE, et al. Antibiotics versus Appendectomy for Acute Appendicitis – Longer-Term Outcomes. N Engl J Med. 2021 Dec 16;385(25):2395-2397.
- Scheijmans JCG, Haijanen J, Flum DR, et al. Antibiotic treatment versus appendicectomy for acute appendicitis in adults: an individual patient data meta-analysis. Lancet Gastroenterol Hepatol. 2025 Mar;10(3):222-233.
- Schuster KM, Holena DN, Salim A, et al. American Association for the Surgery of Trauma emergency general surgery guideline summaries 2018: acute appendicitis, acute cholecystitis, acute diverticulitis, acute pancreatitis, and small bowel obstruction. Trauma Surg Acute Care Open. 2019 Mar 27;4(1):e000281.
- Rushing A, Bugaev N, Jones C, et al. Management of acute appendicitis in adults: A practice management guideline from the Eastern Association for the Surgery of Trauma. J Trauma Acute Care Surg. 2019 Jul;87(1):214-224.
- Podda M, Cillara N, Di Saverio S, et al. Antibiotics-first strategy for uncomplicated acute appendicitis in adults is associated with increased rates of peritonitis at surgery. A systematic review with meta-analysis of randomized controlled trials comparing appendectomy and non-operative management with antibiotics. Surgeon. 2017;15:303–14.
- Sippola S, Haijanen J, Grönroos J, et al. Effect of Oral Moxifloxacin vs Intravenous Ertapenem Plus Oral Levofloxacin for Treatment of Uncomplicated Acute Appendicitis: The APPAC II Randomized Clinical Trial. JAMA. 2021 Jan 26;325(4):353-362.
- Selänne L, Haijanen J, Sippola S, et al. Three-Year Outcomes of Oral Antibiotics vs Intravenous and Oral Antibiotics for Uncomplicated Acute Appendicitis: A Secondary Analysis of the APPAC II Randomized Clinical Trial. JAMA Surg. 2024 Jul 1;159(7):727-735.
- Jalava K, Sallinen V, Lampela H, et al. Role of Preoperative Antibiotic Treatment While Awaiting Appendectomy: The PERFECT-Antibiotics Randomized Clinical Trial. JAMA Surg. 2025 Jul 1;160(7):745-754.
- Antoniou SA, Mavridis D, Kontouli KM, et al. EAES rapid guideline: appendicitis in the elderly. Surg Endosc. 2021;35(7):3233-3243.




