Today on the emDOCs cast with Brit Long, MD (@long_brit), we cover stercoral colitis.
Episode 140: Stercoral Colitis
What is stercoral colitis?
- Stercoral colitis is an inflammatory condition of the large bowel.
- Caused by longstanding constipation with substantial stool burden; leads to high intraluminal pressures and colonic distension.
- Most common area is the sigmoid colon, the antimesenteric border of the rectosigmoid junction, and the anterior rectum.
- These areas exhibit decreased perfusion in watershed areas, smaller luminal diameters, and lower stool water content.
- High pressures and intraluminal distension cause vascular compression of bowel wall; if untreated, progresses to bowel ulceration, focal bowel ischemia, bowel wall perforation, peritonitis, sepsis, and death.
How common is this?
- True prevalence and incidence not well understood; likely uncommon overall.
- 2023 retrospective chart review of all ED encounters at 21 U.S. hospitals over a 29-month period identified that the words “stercoral colitis” appeared in the impressions of 0.008% of all CT abd/pelvis in patients > 65 years and 0.003% of CT impressions regardless of age.
- Median age of diagnosis was 76 years with a range of 6 to 98 years [1].
- Another study found 3.2% of all bowel perforations were due to stercoral colitis over 5 years.
- Mortality rates range between 32-60% if perforation occurs with stercoral colitis [7-8].
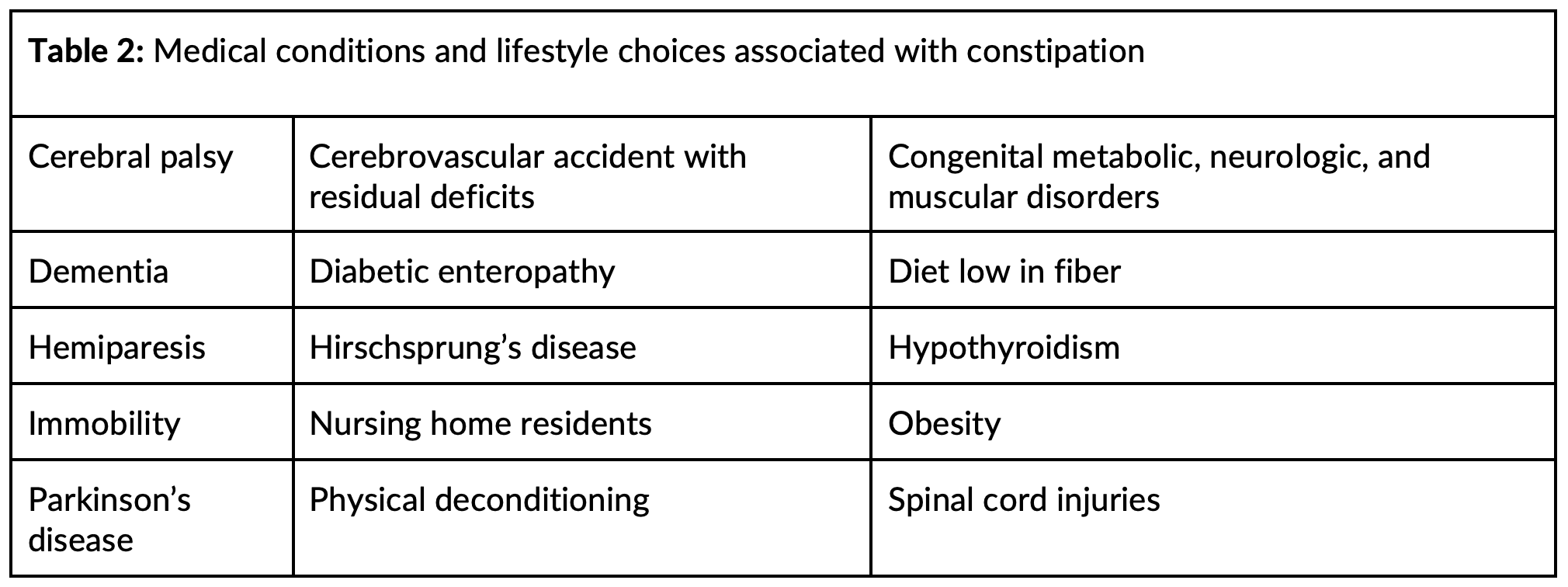
What are the major risk factors?
- Major risk factors are chronic constipation and older age.
- Chronic constipation affects over one third of patients over 60 years, with females more commonly affected [9].
- Other common risk factors include poor diet, immobility and/or sedentary lifestyle, nursing home or long care facility resident, dementia, psychiatric conditions, and medication side effects (in particular opioids, but many others).

How do these patients present?
- Variable presentation, with no pathognomonic constellation of symptoms.
- Common symptoms: abdominal pain and cramping, abdominal distention, constipation, rectal pain, nausea, and vomiting.
- Less common symptoms: general weakness, altered mental status, problems with urination, and gastrointestinal hemorrhage
- Exam: abdominal tenderness to palpation, tenderness and impacted stool on digital rectal examination. Peritonitis, abnormal vital signs/hemodynamic instability may be present with perforation.
- Literature suggests many patients will not present with the classic presentation:
- 39% of patients report a chronic history of constipation [3].
- 2024 study estimated that of patients with radiographic evidence of stercoral colitis, 62% denied abdominal pain; 22% had a chief complaint not GI related.
- 2023 chart review reported that 46% of mild cases and 22% of moderate to severe cases lacked common symptoms [5].
- Patients who are elderly or who have developmental disabilities are more likely to present with unrelated symptoms [14, 24-25].
- Key: Do not rely on the classic picture for diagnosis. Imaging need for further evaluation.
What testing is recommended?
- Diagnosis requires imaging with CT abdomen/pelvis IV contrast.
- No official diagnostic criteria for CT.
- Mild cases: impacted stool, fecaloma, colonic dilation.
- Moderate: colonic dilation >6 cm, colonic wall thickening >3 mm, pericolonic fat stranding.
- Severe/Perforation: pneumoperitoneum, pneumatosis intestinalis, pericolonic abscess, extraluminal stool, discontinuity in the bowel wall.
- X-ray (abdominal/chest) may reveal free air if perforation occurs.
- Laboratory testing is nonspecific: leukocytosis, elevated acute phase reactants, lactic acidosis, electrolyte abnormalities. Obtain blood cultures if unstable/concern for perforation.
What are the key tenets of management?
- No society guideline recommendations for treatment.
- Goal: resuscitate if necessary; decrease intraluminal pressure with fecaloma removal.
- Manage symptoms with antiemetics, analgesics (avoid opioids if possible), IV fluid resuscitation if dehydration, electrolyte repletion.
- Mild/moderate cases without perforation: consider performing a digital rectal disimpaction followed by bowel enema and oral bowel regimen [15].
- No specific enema superior in patients with stercoral colitis. In addition, an oral bowel regimen should be started.
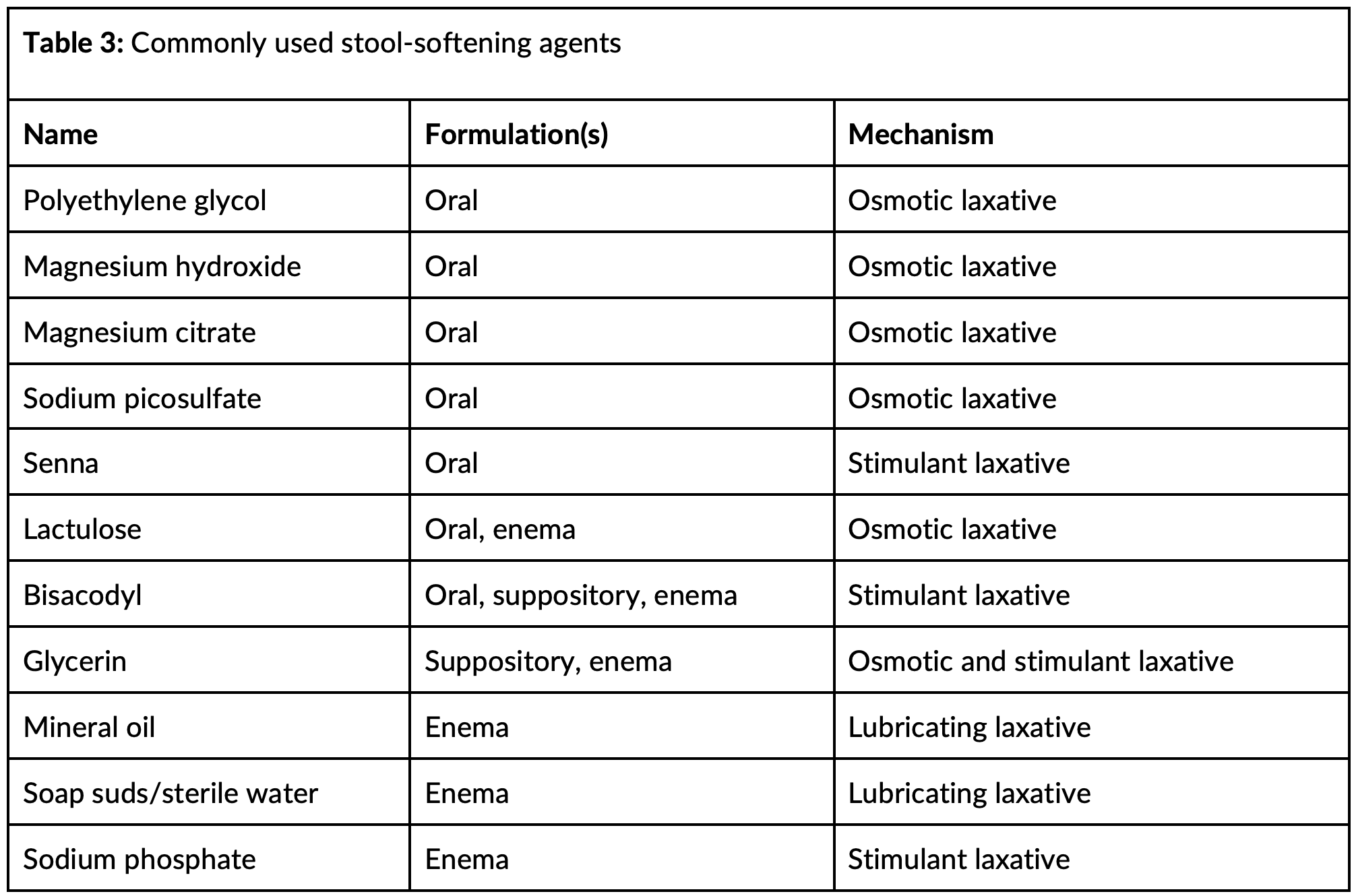
- Oral bowel regimen: combination of osmotic laxatives and stimulant laxatives.
Should we consult the surgeon in all cases of stercoral colitis?
- Consultation is recommended in most (if not all) patients with stercoral colitis.
- Emergent indications for surgical intervention: stercoral perforation, peritonitis, ischemic colitis, gastrointestinal hemorrhage, and failed conservative management [15].
- These patients need resuscitation (IV fluids and vasopressors), broad spectrum antibiotics that cover Pseudomonas aeruginosa, Enterobacter subspecies, anaerobic bacteria, and Enterococcus subspecies (piperacillin-tazobactam 4.5 g every 6 hours or meropenem 1 g every 8 hours or metronidazole 500 mg every 8 hours plus ampicillin 2 g every 4 hours plus cefepime 2 g every 8 hours).
- Surgical specialist consultation recommended for extensive bowel involvement (> 40 cm of contiguous involvement associated with increased mortality).
Why involve a surgeon in mild/moderate cases?
- Controversy as to whether patients with uncomplicated cases of stercoral colitis need surgery consultation in the ED.
- Positives: surgical specialists can perform endoscopic disimpaction and lavage (assist in bowel decompression); endoscopic disimpaction and lavage could be superior to digital disimpaction and medical management.
- Negatives: Unless direct visualization is required to secure the diagnosis, endoscopic disimpaction and lavage is often unnecessary, technically challenging, and may cause iatrogenic injury.
- Consultation with a surgical specialist is not a substitute for performing a digital rectal disimpaction and initiating medical management while the patient is in the ED.
How should we manage the patient with mild/moderate stercoral colitis?
- Digital disimpaction dislodges impacted stool in the rectum and is recommended in those with no perforation. If perforation or severe inflammation, avoid disimpaction.
- Following disimpaction, administer enema. Enemas draw water into the bowel, directly lubricate the stool, and/or stimulate the large bowel to eliminate stool.
- Lubricating enemas include those containing mineral oil and soap suds/tap water.
- Stimulant enema: bisacodyl is a stimulant enema.
- Combination of osmotic, lubricating, stimulating effects: glycerin and sodium phosphate enemas.
- There are no guidelines or available data identifying the most superior enema in stercoral colitis.
- Signals toward harm for sodium phosphate enemas in elderly and pediatric patients being treated for constipation.
- Start oral bowel regimen:
- Polyethylene glycol, lactulose, magnesium hydroxide, magnesium citrate.
- Inexpensive, readily available oral osmotic laxatives.
- Polyethylene glycol and lactulose are superior to placebo for constipation.
- Some experts recommend a full bowel preparation (e.g., those prior to colonoscopy) as first line oral bowel regimen for stercoral colitis.
- Bisacodyl, sodium picosulfate, senna are stimulant laxatives: irritate sensory nerve endings in the colon, reduce colonic water absorption.
- Unless there is dietary fiber deficiency, fiber supplementation not recommended given its mechanism as a bulking agent (does not improve colonic motility).
- Polyethylene glycol, lactulose, magnesium hydroxide, magnesium citrate.
- PAMORAs (Peripherally acting μ-opioid receptor antagonists): medication class for patients with stercoral colitis induced by opioid use.
- Maldemedine, naloxegol, methylnaltrexone.
- American Gastroenterological Association recommends treatment of opioid induced constipation with conventional laxatives first, but guidelines recommend that PAMORAs be considered in cases of laxative-refractory opioid-induced constipation, defined as moderate to severe symptoms of constipation despite the use of laxatives from 1 or more laxative classes for at least 4 days over a 2 week period.
- If present, naldemedine or naloxegol is strongly recommended, but methylnaltrexone has a conditional recommendation.
- Naldemedine and naloxegol are available in oral formulations; methylnaltrexone is available in oral and subcutaneous formulations.
- Cost may limit availability.
Can patients with mild to moderate stercoral colitis be safely discharged from the ED?
- No evidence-based guidelines for disposition of patients diagnosed with stercoral colitis in the ED with immediate indication for surgical intervention [1-2].
- Also no current clinical decision tools to assist in determining disposition.
- Patients not requiring emergent surgical evaluation require aggressive medical management to prevent disease progression with multimodal bowel regimen, dietary changes.
- Repeat clinical assessment and monitoring of the quantity and consistency of bowel movements also necessary.
- Patients can experience electrolyte imbalances due to medical therapies for stercoral colitis.
- Due to these factors, combined with the high associated short term morbidity and mortality, inpatient admission likely beneficial.
What is the prognosis for patients diagnosed with stercoral colitis?
- High risk of short-term morbidity and mortality due to complications: ischemic colitis, stercoral perforation, intra-abdominal abscess, peritonitis, urinary retention, ureteral compression, and sepsis.
- Key complications associated with increased mortality: ischemic colitis (35%), perforation (35%), perforation with septic shock (60%).
- Patients with > 40 cm of involvement have mortality rate of 57.1%.
- Rare complications: lower GI hemorrhage; small bowel evisceration through stercoral perforation; infection or abscess of the musculature of the back, spine, epidural space.
- Complications needing urgent surgical intervention: abdominopelvic abscess, rectal stump leak, and interval re-development of stercoral colitis and perforation of the remaining bowel.
- 2023 retrospective chart review of stercoral colitis found 3.3% died of a complication from stercoral colitis within 3 months; all-cause mortality was 7.8%, 12.3%, and 19.8% at 1 month, 3 months, and 12 months, respectively [1]. Median days from ED diagnosis to death was 152, 76, and 81 for patients discharged from the ED, admitted to the hospital, and overall, respectively.
What are the takeaways?
- Stercoral colitis is an inflammatory condition of the large bowel associated with constipation and fecal impaction leading to increased intraluminal pressure, necrosis, ulceration, and even perforation of the colon
- Variety of ways it can present, but most commonly patients have abdominal pain and constipation
- Major risk factors are older age, constipation, bed-bound, and chronically ill patients.
- CT abd/pelvis with IV contrast recommended for diagnosis.
- Treatment goals are resuscitation if needed and intraluminal decompression.
- For mild to moderate stercoral colitis perform digital rectal disimpaction, followed by enema and oral bowel regimen.
- Surgery consultation with admission is likely helpful in all patients because of the complications and need for monitoring.
- Patients with severe complications like perforation need IV antibiotics, resuscitation, and operative intervention.
References:
- Keim AA, Campbell RL, Mullan AF, et al. Stercoral Colitis in the Emergency Department: A Retrospective Review of Presentation, Management, and Outcomes. Ann Emerg Med. 2023 Jul;82(1):37-46. doi: 10.1016/j.annemergmed.2023.02.003. Epub 2023 Mar 23. PMID: 36966044.
- Bae E, Tran J, Shah K. Stercoral colitis in the emergency department: a review of the literature. Int J Emerg Med. 2024 Jan 2;17(1):3. doi: 10.1186/s12245-023-00578-x. PMID: 38166616; PMCID: PMC10759528.
- Serpell JW, Nicholls RJ. Stercoral perforation of the colon. Br J Surg. 1990 Dec;77(12):1325-9. doi: 10.1002/bjs.1800771204. PMID: 2276009.
- Chakravartty S, Chang A, Nunoo-Mensah J. A systematic review of stercoral perforation. Colorectal Dis. 2013 Aug;15(8):930-5. doi: 10.1111/codi.12123. PMID: 23331762.
- Zacharias NA, Lubner MG, Richards ES, Mao L, Pickhardt PJ. Stercoral colitis: CT imaging findings and clinical risk factors. Abdom Radiol (NY). 2023 Oct;48(10):3050-3062. doi: 10.1007/s00261-023-03974-2. Epub 2023 Jun 27. PMID: 37369923.
- Maurer CA, Renzulli P, Mazzucchelli L, Egger B, Seiler CA, Büchler MW. Use of accurate diagnostic criteria may increase incidence of stercoral perforation of the colon. Dis Colon Rectum. 2000 Jul;43(7):991-8. doi: 10.1007/BF02237366. PMID: 10910249.
- Heffernan C, Pachter HL, Megibow AJ, Macari M. Stercoral colitis leading to fatal peritonitis: CT findings. AJR Am J Roentgenol. 2005 Apr;184(4):1189-93.
- Naseer M, Gandhi J, Chams N, Kulairi Z. Stercoral colitis complicated with ischemic colitis: a double-edge sword. BMC Gastroenterol. 2017 Nov 28;17(1):129
- Forootan M, Bagheri N, Darvishi M. Chronic constipation: A review of literature. Medicine (Baltimore). 2018 May;97(20):e10631
- Kakiuchi T, Fukuta A, Yoshimaru K, Zhang Y, Shimoda R, Matsuo M. Stercoral ulcer after Hirschsprung’s disease surgery. Clin Case Rep. 2021 Dec 26;9(12):e05239. doi: 10.1002/ccr3.5239. PMID: 34963813; PMCID: PMC8710845.
- Gekas P, Schuster MM. Stercoral perforation of the colon: case report and review of the literature. Gastroenterology. 1981 May;80(5 pt 1):1054-8. PMID: 7202964.
- Uwagbale E, Bodiwala V, Agbroko S, Bigajer E. A Case of Stercoral Colitis Complicated by Ischemic Colitis in a Young Patient. Cureus. 2022 Jun 17;14(6):e26050. doi: 10.7759/cureus.26050. PMID: 35859979; PMCID: PMC9288860.
- Tateno F, Sakakibara R, Aiba Y, et al. Stercoral Ulcer and Colonic Perforation in an Individual with Parkinson’s Disease with Constipation. J Am Geriatr Soc. 2016 Oct;64(10):e118-e120. doi: 10.1111/jgs.14357. Epub 2016 Oct 4. PMID: 27701730.
- Chowdhary R, Liu B, Husnain M. Stercoral Colitis as a Cause of Altered Mental Status in a Patient With Cerebral Palsy. Cureus. 2022 Dec 28;14(12):e33040. doi: 10.7759/cureus.33040. PMID: 36721554; PMCID: PMC9881501.
- Tajmalzai A, Najah DM. Stercoral colitis due to massive fecal impaction: a case report and literature review. Radiol Case Rep. 2021 Jun 8;16(8):1946-1950. doi: 10.1016/j.radcr.2021.04.067. PMID: 34149980; PMCID: PMC8193071.
- Panneerselvam S, Carlson JJ, Lin D. Stercoral Colitis: When Constipation is an Emergency. Am J Med Sci. 2021 Jun;361(6):e61-e62. doi: 10.1016/j.amjms.2020.11.013. Epub 2020 Nov 22. PMID: 33933225.
- Lee HJ, Kim KH, Lee SC, Song S. Prognostic Factors of Patients with Stercoral Perforation of the Colon. Korean J Gastroenterol. 2020 Oct 25;76(4):191-198. doi: 10.4166/kjg.2020.76.4.191. PMID: 33100314.
- Mahmoudi A, Maâtouk M, Noomen F, Nasr M, Zouari K, Hamdi A. La perforation stercorale du côlon: à propos d’un cas et revue de la littérature [Stercoral the perforation of the colon: report of a case and review of literature]. Pan Afr Med J. 2015 Nov 17;22:249. French. doi: 10.11604/pamj.2015.22.249.8114. PMID: 26958112; PMCID: PMC4764317.
- Moore LJ, Moore FA. Early diagnosis and evidence-based care of surgical sepsis. J Intensive Care Med. 2013 Mar-Apr;28(2):107-17. doi: 10.1177/0885066611408690. Epub 2011 Jul 11. PMID: 21747125.
- Morano C, Sharman T. Stercoral Colitis. 2023 Jul 10. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan–. PMID: 32809443.
- Hassranah S, Maharajh S, Solomon S, Naraynsingh V. Massive Rectal Hemorrhage From a Stercoral Ulcer. Cureus. 2022 Jul 18;14(7):e26963. doi: 10.7759/cureus.26963. PMID: 35989792; PMCID: PMC9382688.
- Ahmad H, Jannat H, Khan U, Ahmad N. Stercoral Colitis: A Diagnostic Challenge and Therapeutic Approach in an Elderly Patient With Chronic Constipation. Cureus. 2023 May 18;15(5):e39179. doi: 10.7759/cureus.39179. PMID: 37378172; PMCID: PMC10292177.
- Chiang CM, Chiang HC. Gastrointestinal: Stercoral colitis complicated with perforation and bleeding. J Gastroenterol Hepatol. 2024 Jun;39(6):984-985. doi: 10.1111/jgh.16460. Epub 2023 Dec 30. PMID: 38159081.
- Caillet A, Steiner M, Sawaya D, Nowicki M. Stercoral Colitis With Silent Perforation in a Child. J Clin Gastroenterol. 2016 Oct;50(9):799-800. doi: 10.1097/MCG.0000000000000610. PMID: 27466168.
- Kloub MN, Haddad A, Abushanab M, et al. Stercoral Colitis-Induced Ischemia Mimicking acute Mesenteric Ischemia: A case report and Literature Review. Eur J Case Rep Intern Med. 2024 Feb 28;11(3):004328. doi: 10.12890/2024_004328. PMID: 38455697; PMCID: PMC10917405.
- Latif E, Musthafa S, Ahmed A, Abu Amr A. Stercoral Perforation of Sigmoid Colon in Systemic Lupus Erythematosus: A Rare Cause of Peritonitis. Cureus. 2020 Jul 31;12(7):e9495. doi: 10.7759/cureus.9495. PMID: 32879819; PMCID: PMC7458703.
- Ottaviano KE, Hill SS. Management of Stercoral Colitis. Dis Colon Rectum. 2024 May 1;67(5):612-613. doi: 10.1097/DCR.0000000000003295. Epub 2024 Feb 7. PMID: 38595224.
- Crockett SD, Greer KB, Heidelbaugh JJ, Falck-Ytter Y, Hanson BJ, Sultan S; American Gastroenterological Association Institute Clinical Guidelines Committee. American Gastroenterological Association Institute Guideline on the Medical Management of Opioid-Induced Constipation. Gastroenterology. 2019 Jan;156(1):218-226. doi: 10.1053/j.gastro.2018.07.016. Epub 2018 Oct 16. PMID: 30340754.
- Ünal E, Onur MR, Balcı S, Görmez A, Akpınar E, Böge M. Stercoral colitis: diagnostic value of CT findings. Diagn Interv Radiol. 2017 Jan-Feb;23(1):5-9. doi: 10.5152/dir.2016.16002. PMID: 27910814; PMCID: PMC5214077.
- Brandt LJ, Feuerstadt P, Longstreth GF, Boley SJ; American College of Gastroenterology. ACG clinical guideline: epidemiology, risk factors, patterns of presentation, diagnosis, and management of colon ischemia (CI). Am J Gastroenterol. 2015 Jan;110(1):18-44; quiz 45. doi: 10.1038/ajg.2014.395. Epub 2014 Dec 23. PMID: 25559486.
- Thomas MJ, Nanagiri A, Duvidovich S, Levy L, Bamji N. Mission Disimpaction: Endoscopic Management of Stercoral Colitis in an Adolescent. JPGN Rep. 2023 Mar 9;4(2):e300. doi: 10.1097/PG9.0000000000000300. PMID: 37200732; PMCID: PMC10187833.
- Kakiuchi T, Fukuta A, Yoshimaru K, Zhang Y, Shimoda R, Matsuo M. Stercoral ulcer after Hirschsprung’s disease surgery. Clin Case Rep. 2021 Dec 26;9(12):e05239. doi: 10.1002/ccr3.5239. PMID: 34963813; PMCID: PMC8710845.
- Chopra A, Rothstein A, Mohamed Ahmed A, Pannell S. Small Bowel Evisceration Through a Perforated Stercoral Ulcer. Am Surg. 2023 Jun;89(6):2885-2887. doi: 10.1177/00031348221075733. Epub 2022 Feb 5. PMID: 35128955.
- Uy CE, Jiang SY, Murray MC. Epidural abscess and feculent meningitis secondary to stercoral ulcer rupture. BMJ Case Rep. 2015 Jan 7;2015:bcr2014207858. doi: 10.1136/bcr-2014-207858. PMID: 25566932; PMCID: PMC4289759.
- Serpell JW, Sen M, Giddins G, Nicholls RJ, Bradfield WJ. Stercoral perforation of the colon proximal to an end colostomy. Postgrad Med J. 1991 Mar;67(785):299-300. doi: 10.1136/pgmj.67.785.299. PMID: 2062783; PMCID: PMC2399011.
- Ori Y, Rozen-Zvi B, Chagnac A, Herman M, Zingerman B, Atar E, Gafter U, Korzets A. Fatalities and severe metabolic disorders associated with the use of sodium phosphate enemas: a single center’s experience. Arch Intern Med. 2012 Feb 13;172(3):263-5. doi: 10.1001/archinternmed.2011.694. PMID: 22332159.
- Mendoza J, Legido J, Rubio S, Gisbert JP. Systematic review: the adverse effects of sodium phosphate enema. Aliment Pharmacol Ther. 2007 Jul 1;26(1):9-20. doi: 10.1111/j.1365-2036.2007.03354.x. PMID: 17555417.
- Mazuski JE, Tessier JM, May AK, et al. The Surgical Infection Society Revised Guidelines on the Management of Intra-Abdominal Infection. Surg Infect (Larchmt). 2017 Jan;18(1):1-76. doi: 10.1089/sur.2016.261. PMID: 28085573
- van Nispen C, Long B. High risk and low incidence diseases: Stercoral colitis. Am J Emerg Med. 2025 Apr;90:151-156. doi: 10.1016/j.ajem.2025.01.056. Epub 2025 Jan 22. PMID: 39874678.




