
Authors: Zayd Al Rawi (MS-4, University of Missouri-Columbia); Catherine Parker, MD (PD/Associate Professor of EM/Attending Physician, University of Missouri-Columbia); Jessica Pelletier, DO, MHPE (APD/Assistant Professor of EM/Attending Physician, University of Missouri-Columbia) // Reviewed by: Sophia Görgens, MD (EM Physician, Yale University, CT); Cassandra Mackey, MD (Assistant Professor of Emergency Medicine, UMass Chan Medical School); Brit Long, MD (@long_brit)
Welcome to EM@3AM, an emDOCs series designed to foster your working knowledge by providing an expedited review of clinical basics. We’ll keep it short, while you keep that EM brain sharp.
A 73-year-old male presents to the ED with worsening shortness of breath over the last year. He also reports increased swelling in his lower extremities and has been sleeping with an extra pillow as his shortness of breath worsens when lying down. He has lost 15 pounds in the last year. His PMHx includes bilateral carpal tunnel release surgery but is otherwise unremarkable. He takes no medications.
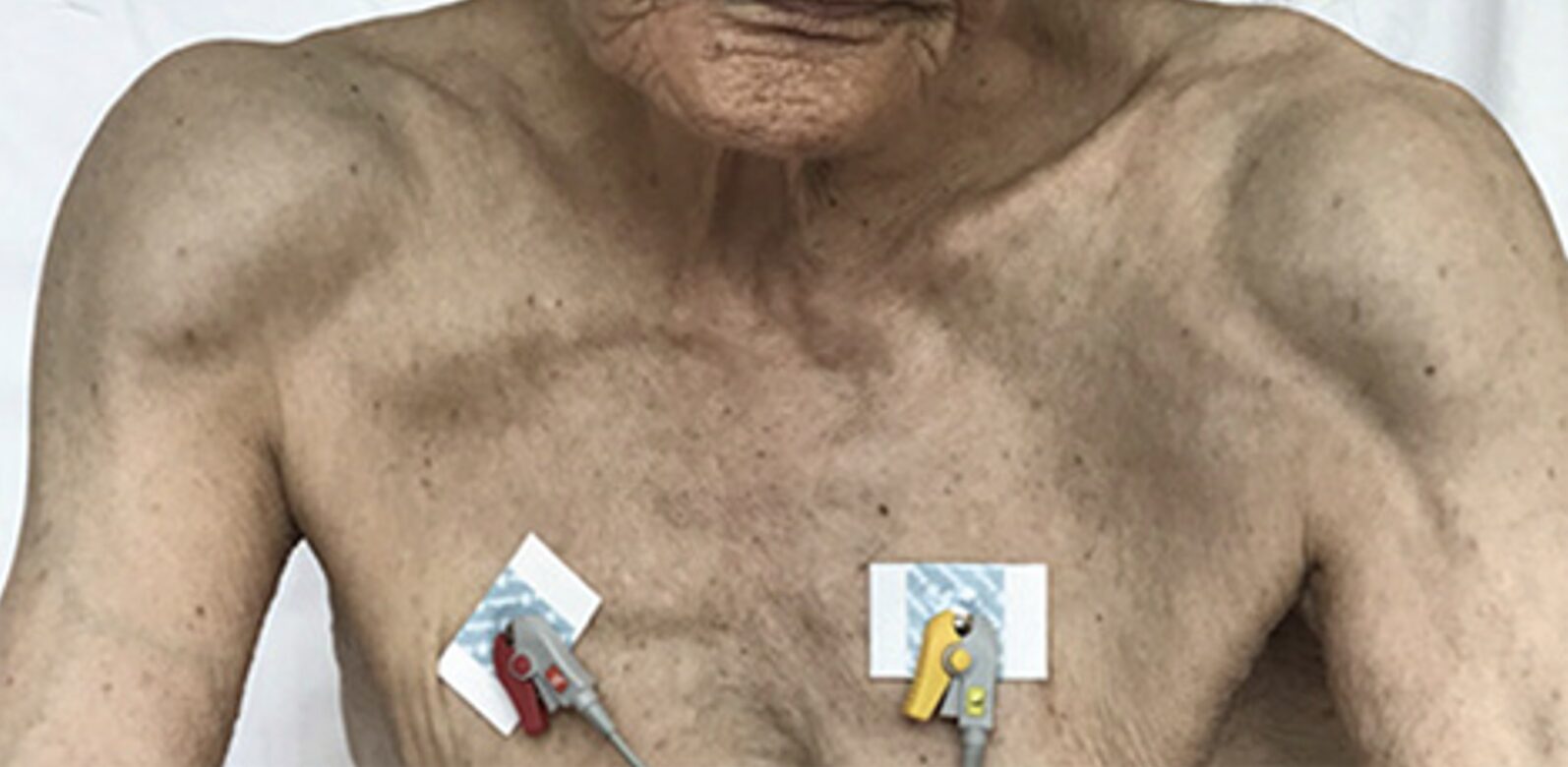
Vital signs are BP of 130/78, HR of 89, RR 18, SPO2 94% on RA, Temp 37 degrees Celsius. On exam, there is pitting edema in the lower extremities, and decreased sensation in the hands and feet bilaterally. Liver span is 17 cm. There is bilateral anterior shoulder swelling (Figure 1), peri-orbital purpura, and macroglossia.
Figure 1. Shoulder pad sign in a patient with amyloidosis. Source: Uzunoğlu C, Toptaş T, İpek Y, Arıkan F, Yılmaz F, Tuğlular T. – Uzunoğlu C, Toptaş T, İpek Y, Arıkan F, Yılmaz F, Tuğlular T. Shoulder-Pad Sign in a Case of Amyloidosis Associated with Myeloma. Turk J Haematol. 2021 Aug 25;38(3):233-234. doi: 10.4274/tjh.galenos.2021.2021.0630. Epub 2021 May 20. PMID: 34014054; PMCID: PMC8386310.https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8386310/figure/f1/, CC BY 4.0, https://commons.wikimedia.org/w/index.php?curid=130031970
An ECG shows a second-degree heart block. BNP is significantly elevated. Point of care glucose and A1C are within normal limits. A bedside cardiac US shows bilateral ventricular wall thickening of 14mm, a preserved left ventricular ejection fraction (LVEF), and no ventricular dilatation.
What is the diagnosis?
Answer: Amyloidosis
Background:
- Amyloidosis is the deposition of abnormally folded proteins (amyloid), which leads to organ damage. In systemic amyloidosis, deposits can occur anywhere in the body.
- All subtypes begin with the letter A, representing amyloid, followed by an abbreviation for the deposited protein.1
Etiology:
- There are different types of amyloid, each with distinct underlying causes and treatments. The most common types include:
- Immunoglobulin light chain amyloid (AL): AL amyloidosis is the most common subtype in developed countries.2 The majority of cases are associated with monoclonal proliferation of plasma cells and their associated immunoglobulin light chains.1,3–5
- Amyloid deposition can occur in any organ other than the central nervous system.6
- Transthyretin amyloid protein (ATTR): ATTR is associated with hereditary mutations and can occur spontaneously with aging.4
- Serum amyloid A (AA): AA amyloidosis is associated with an underlying inflammatory or infectious diseases, including but not limited to inflammatory arthritis, IBD, immunodeficiencies, malaria, and TB .4,7–9
- Most common subtype in developing countries2
- Incidence of AA amyloidosis has decreased over time in developed countries, thought to be due to the advancement of treatments targeting underlying inflammatory conditions or infections.10
- Inflammatory conditions are now a more common underlying cause for AA amyloidosis in high-income settings; infections are a less common cause given the availability of antibiotics and a more cleaner environment11
- In developing parts of the world, incidence has not decreased.12
- This is thought to be due to the lack of availability of treatments to control underlying chronic inflammatory and infectious conditions2
- Immunoglobulin light chain amyloid (AL): AL amyloidosis is the most common subtype in developed countries.2 The majority of cases are associated with monoclonal proliferation of plasma cells and their associated immunoglobulin light chains.1,3–5
Epidemiology:
- Risk factors associated with AL amyloidosis include increasing age (>60), male sex, family history of AL amyloidosis, and underlying monoclonal gammopathies.13–15
- The incidence of amyloidosis is around 16 per million in the adult population.13,14
- The disease has become more prevalent over time, thought to be due to better treatment options increasing survival.3,13
Clinical Presentation:
- Signs and symptoms of amyloidosis involve multiple organs: The heart (70% of cases) and kidneys (60%) are by far the most affected organ systems, followed by the liver (20%) and gastrointestinal (15%), the peripheral (15%) or autonomic (10%) nervous system, and finally soft tissues (10%).4,10,16
- Cardiovascular symptoms: heart failure with preserved ejection fraction, including shortness of breath, orthopnea, paroxysmal nocturnal dyspnea (PND), arrhythmias, and elevated jugular venous pressure (JVP).
- Renal symptoms: nephrotic proteinuria not diabetic in origin, peripheral edema.
- Liver and GI symptoms: hepatomegaly, bleeding disorders (lack of clotting factors), unintentional weight loss, and early satiety.4,10,16
- Nervous system symptoms: Non-diabetic peripheral neuropathy, autonomic neuropathy (orthostatic hypotension, erectile dysfunction).4,16,17
- Soft tissue: macroglossia resulting in obstructive sleep apnea (OSA), periorbital purpura, and joint swelling from amyloid deposition.16,18–20
- Carpal tunnel syndrome is a major sign of amyloidosis (especially if bilateral, or history of carpal tunnel release surgery).21,22
- The shoulders are the most commonly affected joint in AL amyloidosis; the shoulder pad sign (as seen in the case above) is the increased prominence of the bilateral shoulders from amyloid deposition.19,23
- Up to a third of patients present with only one organ involved, emphasizing the importance of keeping a high index of suspicion.16,24
Evaluation:
- Labs to order include CBC, CMP, PT/PTT, troponins, BNP, and a 24-hour urine protein test.25,26
- Liver involvement is suggested by elevated liver function tests (LFTs) and abnormal coagulation studies (PT/PTT prolongation due to decreased factor X).16,26
- 24-hour urine protein >500 mg/day, predominantly albumin is indicative of renal involvement.
- BNP ≥ 332 (without renal failure or atrial fibrillation as the underlying cause) is indicative of cardiac involvement. May also see elevated troponin.25,26
- CBC has been shown to exhibit elevated blood counts, including WBCs, neutrophils, platelets, and RBCs, but is commonly unremarkable.27
- Electrocardiogram (ECG) may show low voltage in limb leads (<5 mm), poor R wave progression, arrhythmias, and heart block.4,8,16,28
- Cardiac ultrasound should be performed; the triad of ventricular wall thickening (LV ≥ 12 mm), preserved ejection fraction, and no ventricular dilatation increases suspicion for cardiac amyloidosis.4,26
- Lungs – computed tomography (CT) may show interstitial radiographic findings.26,29,30
- CT is preferred over plain radiographs (X-rays) because it is more sensitive for detecting diffuse interstitial amyloid deposits.
- As lung involvement is often clinically asymptomatic, CT scan can be ordered for screening in suspecting amyloidosis even without pulmonary symptoms.
- This can be deferred to the outpatient setting if the patient with suspected amyloidosis is not presenting with respiratory symptoms.
- X-ray may reveal interstitial pulmonary edema secondary to amyloidosis-induced heart failure or direct amyloid infiltration of the lungs.26,29,30
- As lung involvement is often clinically asymptomatic, CT scan can be ordered for screening in suspecting amyloidosis even without pulmonary symptoms.
- Magnetic resonance imaging (MRI) with late gadolinium enhancement (LGE): may be ordered on an outpatient basis, shows diffuse transmural (more common) or subendocardial (less common but pathognomonic) LGE pattern.8,31
- If amyloidosis is suspected and the patient has a prior hematologic disorder that might be a trigger (like a plasma cell dyscrasia), hematology should be consulted.25 Hematology should be consulted for all suspected AL amyloidosis cases.32
- Cardiology consult is also recommended in suspected amyloidosis with cardiac involvement.32
- CT is preferred over plain radiographs (X-rays) because it is more sensitive for detecting diffuse interstitial amyloid deposits.
Diagnosis:
- Gold standard to diagnose amyloidosis: Congo red staining of a biopsy showing apple-green birefringence under polarized light.1,4,33
- Abdominal fat and bone marrow biopsies are preferred and can help establish a diagnosis earlier.4,16,24,34
- A bone marrow biopsy will also evaluate for possible underlying plasma cell dyscrasia (multiple myeloma, monoclonal gammopathy of unknown significance, etc).8,34
- Additionally, both serum and urine measurements of free light chains (FLC) and immunofixation electrophoresis (IFE) are required to help screen for monoclonal proteins.8,10,35
- These tests may not be available in the ED and thus may be deferred to the inpatient setting (if the patient is sick and needs admission) or the outpatient setting (if they are being discharged).
- After establishing the diagnosis of amyloidosis, tests that differentiate the subtype are important, as it will guide treatment.4,33
- Immunofluorescence (IF) or Immunohistochemistry (IHC) is often the initial method for differentiating the subtype, but mass spectrometry is used when the diagnosis is unclear.
Treatment:
- In patients with suspected amyloidogenic heart failure:36–38
- Avoid:
- Beta-blockers, calcium channel blockers, and digoxin (negative inotropy decreases the compensatory heart rate, which supports the cardiac output in a reduced stroke volume state).
- Nitrates and ACE inhibitors (may lead to hypotension/reduction in preload).
- Recommended medications: Loop diuretics such as furosemide or torsemide.
- If in shock, use inotropic agents, NOT vasodilators.39
- All patients with amyloidogenic heart failure presenting with atrial fibrillation need lifelong anticoagulation, regardless of CHADS2VASC score.39
- These patients are at high risk for thromboembolism and should not undergo cardioversion without a transesophageal ECHO.
- Patients with signs of acute organ failure (i.e., acute heart failure, renal failure, or liver failure) should be admitted to the hospital.
- Inpatient vs. outpatient therapies for amyloidosis, depending upon clinical stability:
- Autologous stem cell transplant (ASCT) is the preferred treatment option, but only 20% of patients are eligible after applying exclusion criteria (age >65, >2 organs affected, eGFR<50, LVEF<45%).33
- Current gold standard for induction therapy: Daratumumab plus cyclophosphamide-bortezomib-dexamethasone (CyBorD).8,40,41
- Relapsed or refractory patients: oral proteasome inhibitor (Ixazomib).8,42
- Avoid:
Prognosis:
- Level of cardiac dysfunction at diagnosis is the strongest predictor of prognosis for patients with AL amyloidosis.6
- There are several major staging systems for patients with AL amyloidosis:
- Mayo Clinic 2004 is most commonly used to predict early death.6
- Mayo Clinic 2012 is the best estimate of late survival.24,36,43
- European modification of the Mayo Clinic 2004 staging system predicts early death better than the Mayo Clinic 2012 staging system.44
- Prognosis by stage is highlighted in Table 1.
- Age >70 years or initial presentation with advanced cardiac disease are indicators of poor prognosis.33
- There are several major staging systems for patients with AL amyloidosis:
Table 1. AL amyloidosis prognosis by staging system.6 Adapted from: Sanchorawala V. Systemic Light Chain Amyloidosis. Longo DL, ed. N Engl J Med. 2024;390(24):2295-2307. doi:10.1056/NEJMra2304088. HR = hazard ratio.
| System | Criteria | Stage | Outcome / Treatment Effect |
| Mayo Clinic, 2004 | Troponin T >0.035 ng/ml; NT‑proBNP >332 pg/ml | Stage I: Neither marker above cutoff | HR for death: 1.0 (reference) |
| Stage II: One marker above cutoff | HR for death: 2.5 (1.9–3.5) | ||
| Stage III: Both markers above cutoff | HR for death: 6.7 (6.0–9.1) | ||
| Mayo Clinic, 2012 | Troponin T ≥0.025 ng/ml; NT‑proBNP >1800 pg/ml; dFLC >180 mg/L | Stage I: 0 markers above cutoff | HR for death: 1.0 (reference) |
| Stage II: 1 marker above cutoff | HR for death: 1.7 (1.2–2.3) | ||
| Stage III: 2 markers above cutoff | HR for death: 4.1 (3.1–5.5) | ||
| Stage IV: 3 markers above cutoff | HR for death: 6.3 (4.8–8.3) | ||
| European Modification, 2013 | Troponin T >0.035 μg/L; NT‑proBNP >332 pg/ml; NT‑proBNP >8500 pg/ml | Stage I: Neither marker above cutoff | HR for death: 1.0 (reference) |
| Stage II: One marker above cutoff | HR for death: 2.5 (1.9–3.5) | ||
| Stage IIIa: Both markers above cutoff, NT‑proBNP ≤8500 pg/ml | HR for death: 4.9 (3.6–6.8) | ||
| Stage IIIb: Both markers above cutoff, NT‑proBNP >8500 pg/ml | HR for death: 11.1 (8.1–15.4) | ||
| Renal Staging | eGFR <50 ml/min/1.73 m²; Urine protein >5 g/24 hr | Stage I: Both criteria below cutoff | 2‑yr risk of dialysis: 0–3% |
| Stage II: One criterion above cutoff | 2‑yr risk of dialysis: 11–25% | ||
| Stage III: Both criteria above cutoff | 2‑yr risk of dialysis: 60–75% |
- There is no staging system for AA amyloidosis.47
- Poor prognostic indicators include:
- ESRD at presentation.
- Low serum albumin.
- Older age.
- Serum amyloid A protein (SAA) elevation (most important risk factor for renal failure/death).
- The most common identifiable complications leading to death in patients with amyloidosis are heart and renal failure.48,49
- Poor prognostic indicators include:
Pearls:
- Red flags for amyloidosis include bilateral carpal tunnel syndrome, combined cardiac symptoms and neuropathy, low-voltage ECG, and the shoulder pad sign.
- Remember that ANY organ can be involved!
- If heart failure doesn’t look like heart failure on POCUS (i.e., thick walls, normal chamber size, normal EF), think of amyloidosis.
- Avoid negative inotropes and carefully titrate loop diuretics in the patient with suspected amyloidogenic heart failure.
- Use inotropes for shock.
- AL amyloidosis is a medical emergency and needs specialty consults.
- Err on the side of admission for further workup, unless the suspected amyloidosis patient is markedly stable.

A 39-year-old man presents to the ED with shortness of breath. Imaging studies reveal cardiomegaly, and his laboratory workup is concerning for cardiomyopathy. He is admitted for further diagnostic evaluation. A fat biopsy with Congo red stain demonstrates apple-green birefringence under light microscopy. What type of cardiomyopathy is suggested?
- Autoimmune
- Congenital
- Infiltrative
- Metabolic
Correct answer: C
Amyloidosis is a protein misfolding disorder leading to the extracellular deposition of insoluble proteins in tissues and organs. Diagnosis is commonly made with an abdominal fat pad biopsy. The tissue is stained with Congo red dye and viewed under polarized light microscopy. The beta-pleated sheets of amyloid protein have a characteristic apple–green birefringence. Amyloidosis can affect nearly any organ in the body, including the heart, central nervous system, kidneys, corneas, skin, liver, bones, joints, pancreas, thyroid, and pituitary gland. Amyloid cardiomyopathy is an infiltrative condition associated with ventricular hypertrophy, diastolic dysfunction, elevated B–type natriuretic peptide, and elevated troponin levels.
There are several types of amyloidosis, depending on the type of amyloid precursor protein. Amyloid light chain (AL) amyloidosis is responsible for cardiac involvement, which is the leading cause of death from AL amyloidosis. Patients have poor atrial contractility, which can lead to atrial thrombosis and stroke. Patients with impaired cardiac function have a median survival rate of approximately 6 months after diagnosis. Cardiac transplantation is an option for select patients and is usually accompanied by high-dose intravenous melphalan and stem cell transplantation. Congestive heart failure is treated with diuretics, but certain medications (e.g., calcium channel blockers, beta-blockers, digitalis) can produce heart block due to interaction with amyloid fibrils, so they are relatively contraindicated.

Autoimmune (A) causes of cardiomyopathy include scleroderma, systemic lupus erythematosus, dermatomyositis, and rheumatoid arthritis.
Congenital (B) causes of cardiomyopathy are myriad and include hypertrophic cardiomyopathy, ion channelopathies (e.g., Brugada syndrome), long QT syndrome, and arrhythmogenic right ventricular cardiomyopathy.
Cardiomyopathy secondary to metabolic (D) causes includes conditions such as vitamin deficiencies (e.g., thiamine), endocrinopathies (e.g., hyperthyroidism), and electrolyte disturbances (e.g., hypocalcemia, hypophosphatemia).
Further Reading
Further FOAMed:
References:
- Buxbaum JN, Eisenberg DS, Fändrich M, et al. Amyloid nomenclature 2024: update, novel proteins, and recommendations by the International Society of Amyloidosis (ISA) Nomenclature Committee. Amyloid. 2024;31(4):249-256. doi:10.1080/13506129.2024.2405948
- Vasstrand HJ, Raki M, Skrunes R, et al. Epidemiology and clinical presentation of kidney amyloidosis have changed over the past three decades: a nationwide population-based study. BMC Nephrol. 2025;26(1):272. doi:10.1186/s12882-025-04136-w
- Ravichandran S, Lachmann HJ, Wechalekar AD. Epidemiologic and Survival Trends in Amyloidosis, 1987–2019. N Engl J Med. 2020;382(16):1567-1568. doi:10.1056/NEJMc1917321
- Picken MM. The Pathology of Amyloidosis in Classification: A Review. Acta Haematol. 2020;143(4):322-334. doi:10.1159/000506696
- Zhou P, Comenzo RL, Olshen AB, et al. CD32B is highly expressed on clonal plasma cells from patients with systemic light-chain amyloidosis and provides a target for monoclonal antibody–based therapy. Blood. 2008;111(7):3403-3406. doi:10.1182/blood-2007-11-125526
- Sanchorawala V. Systemic Light Chain Amyloidosis. Longo DL, ed. N Engl J Med. 2024;390(24):2295-2307. doi:10.1056/NEJMra2304088
- Papa R, Lachmann HJ. Secondary, AA, Amyloidosis. Rheum Dis Clin N Am. 2018;44(4):585-603. doi:10.1016/j.rdc.2018.06.004
- Ash S, Shorer E, Ramgobin D, et al. Cardiac amyloidosis‐A review of current literature for the practicing physician. Clin Cardiol. 2021;44(3):322-331. doi:10.1002/clc.23572
- Westermark P, Westermark GT. Reflections on amyloidosis in Papua New Guinea. Philos Trans R Soc B Biol Sci. 2008;363(1510):3701-3705. doi:10.1098/rstb.2008.0073
- Wechalekar AD, Gillmore JD, Hawkins PN. Systemic amyloidosis. The Lancet. 2016;387(10038):2641-2654. doi:10.1016/S0140-6736(15)01274-X
- Deshayes S, Aouba A, Grateau G, Georgin‐Lavialle S. Infections and AA amyloidosis: An overview. Int J Clin Pract. 2021;75(6):e13966. doi:10.1111/ijcp.13966
- Prakash J, Brojen T, Rathore SS, Choudhury TA, Gupta T. The Changing Pattern of Renal Amyloidosis in Indian Subcontinent: Two Decades of Experience from a Single Center. Ren Fail. 2012;34(10):1212-1216. doi:10.3109/0886022X.2012.723514
- Laires PA, Fang S, Evans J, et al. Incidence and prevalence of light chain amyloidosis in the United States in 2019–2021 using Optum EHR data. Sci Rep. 2025;15(1):25149. doi:10.1038/s41598-025-09498-7
- Kyle RA, Larson DR, Kurtin PJ, et al. Incidence of AL Amyloidosis in Olmsted County, Minnesota, 1990 through 2015. Mayo Clin Proc. 2019;94(3):465-471. doi:10.1016/j.mayocp.2018.08.041
- Ríos-Tamayo R. Epidemiology of Systemic Light-Chain (AL) Amyloidosis. Lymphatics. 2025;3(3):25. doi:10.3390/lymphatics3030025
- Vaxman I, Gertz M. When to Suspect a Diagnosis of Amyloidosis. Acta Haematol. 2020;143(4):304-311. doi:10.1159/000506617
- Shin SC, Robinson‐Papp J. Amyloid Neuropathies. Mt Sinai J Med J Transl Pers Med. 2012;79(6):733-748. doi:10.1002/msj.21352
- Aissi K, Rossi P, Bernard F, Granel B, Frances Y. Facial Signs Leading to the Diagnosis of Cardiac Amyloidosis. Am J Med. 2009;122(9):e1-e2. doi:10.1016/j.amjmed.2009.02.027
- Uzunoğlu C, Toptaş T, İpek Y, Arıkan F, Yılmaz F, Tuğlular T. Shoulder-Pad Sign in a Case of Amyloidosis Associated with Myeloma. Turk J Hematol. 2021;38(3):233-234. doi:10.4274/tjh.galenos.2021.2021.0630
- Tsourdi E, Därr R, Wieczorek K, et al. Macroglossia as the only presenting feature of amyloidosis due to MGUS. Eur J Haematol. 2014;92(1):88-89. doi:10.1111/ejh.12163
- Donnelly JP, Hanna M, Sperry BW, Seitz WH. Carpal Tunnel Syndrome: A Potential Early, Red-Flag Sign of Amyloidosis. J Hand Surg. 2019;44(10):868-876. doi:10.1016/j.jhsa.2019.06.016
- Sperry BW, Reyes BA, Ikram A, et al. Tenosynovial and Cardiac Amyloidosis in Patients Undergoing Carpal Tunnel Release. J Am Coll Cardiol. 2018;72(17):2040-2050. doi:10.1016/j.jacc.2018.07.092
- Elsaman AM, Radwan AR, Akmatov MK, et al. Amyloid arthropathy associated with multiple myeloma: A systematic analysis of 101 reported cases. Semin Arthritis Rheum. 2013;43(3):405-412. doi:10.1016/j.semarthrit.2013.07.004
- Muchtar E, Gertz MA, Kyle RA, et al. A Modern Primer on Light Chain Amyloidosis in 592 Patients With Mass Spectrometry–Verified Typing. Mayo Clin Proc. Published online February 2019:S0025619618306104. doi:10.1016/j.mayocp.2018.08.006
- D’Souza A. Amyloid consults do not have to be vexing. Hematology. 2023;2023(1):407-412. doi:10.1182/hematology.2023000440
- Gertz MA, Comenzo R, Falk RH, et al. Definition of organ involvement and treatment response in immunoglobulin light chain amyloidosis (AL): A consensus opinion from the 10th International Symposium on Amyloid and Amyloidosis. Am J Hematol. 2005;79(4):319-328. doi:10.1002/ajh.20381
- Ziarkiewicz M, Szczygieł J, Legatowicz-Koprowska M, et al. AL amyloidosis with elevated peripheral blood cell counts – A frequent association with liver involvement. A single-center retrospective study. Leuk Res Rep. 2025;23:100509. doi:10.1016/j.lrr.2025.100509
- Bhogal S, Ladia V, Sitwala P, et al. Cardiac Amyloidosis: An Updated Review With Emphasis on Diagnosis and Future Directions. Curr Probl Cardiol. 2018;43(1):10-34. doi:10.1016/j.cpcardiol.2017.04.003
- Cordier JF. Pulmonary Amyloidosis in Hematological Disorders. Semin Respir Crit Care Med. 2005;26(05):502-513. doi:10.1055/s-2005-922033
- Khoor A, Colby TV. Amyloidosis of the Lung. Arch Pathol Lab Med. 2017;141(2):247-254. doi:10.5858/arpa.2016-0102-RA
- Carvalho FPD, Erthal F, Azevedo CF. The Role of Cardiac MR Imaging in the Assessment of Patients with Cardiac Amyloidosis. Magn Reson Imaging Clin N Am. 2019;27(3):453-463. doi:10.1016/j.mric.2019.04.005
- American Heart Association. AL Amyloidosis Quick Reference Guide. Accessed April 13, 2026. https://www.heart.org/en/-/media/Files/Professional/AL-Amyloidosis/AL-Amyloidosis-Quick-Reference-Guide-v3_06132025.pdf?sc_lang=en
- Ryšavá R. AL amyloidosis: advances in diagnostics and treatment. Nephrol Dial Transplant. 2019;34(9):1460-1466. doi:10.1093/ndt/gfy291
- Wisniowski B, Wechalekar A. Confirming the Diagnosis of Amyloidosis. Acta Haematol. 2020;143(4):312-321. doi:10.1159/000508022
- Palladini G, Russo P, Bosoni T, et al. Identification of Amyloidogenic Light Chains Requires the Combination of Serum-Free Light Chain Assay with Immunofixation of Serum and Urine. Clin Chem. 2009;55(3):499-504. doi:10.1373/clinchem.2008.117143
- Kumar S, Dispenzieri A, Lacy MQ, et al. Revised Prognostic Staging System for Light Chain Amyloidosis Incorporating Cardiac Biomarkers and Serum Free Light Chain Measurements. J Clin Oncol. 2012;30(9):989-995. doi:10.1200/JCO.2011.38.5724
- Falk RH, Alexander KM, Liao R, Dorbala S. AL (Light-Chain) Cardiac Amyloidosis. J Am Coll Cardiol. 2016;68(12):1323-1341. doi:10.1016/j.jacc.2016.06.053
- Giancaterino S, Urey MA, Darden D, Hsu JC. Management of Arrhythmias in Cardiac Amyloidosis. JACC Clin Electrophysiol. 2020;6(4):351-361. doi:10.1016/j.jacep.2020.01.004
- Kittleson MM, Ruberg FL, Ambardekar AV, et al. 2023 ACC Expert Consensus Decision Pathway on Comprehensive Multidisciplinary Care for the Patient With Cardiac Amyloidosis. J Am Coll Cardiol. 2023;81(11):1076-1126. doi:10.1016/j.jacc.2022.11.022
- Dima D, Mazzoni S, Anwer F, et al. Diagnostic and Treatment Strategies for AL Amyloidosis in an Era of Therapeutic Innovation. JCO Oncol Pract. 2023;19(5):265-275. doi:10.1200/OP.22.00396
- Kastritis E, Palladini G, Minnema MC, et al. Daratumumab-Based Treatment for Immunoglobulin Light-Chain Amyloidosis. N Engl J Med. 2021;385(1):46-58. doi:10.1056/NEJMoa2028631
- Sanchorawala V, Palladini G, Kukreti V, et al. A phase 1/2 study of the oral proteasome inhibitor ixazomib in relapsed or refractory AL amyloidosis. Blood. 2017;130(5):597-605. doi:10.1182/blood-2017-03-771220
- Mohamed A, Basali D, Zou Y, et al. Abstract 4366350: Ten-Year Survival in AL Cardiac Amyloidosis: Does Mayo Staging still matter in the Recent era? Circulation. 2025;152(Suppl_3). doi:10.1161/circ.152.suppl_3.4366350
- Khwaja J, Ravichandran S, Bomsztyk J, et al. Limited utility of Mayo 2012 cardiac staging system for risk stratification of patients with advanced cardiac AL amyloidosis – analysis of a uniformly treated cohort of 1,275 patients. Haematologica. Published online January 11, 2024. doi:10.3324/haematol.2023.284348
- Han M, Yoon SE, Kim S, et al. Prognostic value of mayo 2012 vs. european‑modified mayo 2004 staging in AL amyloidosis patients with discordant stage classifications. Blood. 2025;146(Supplement 1):5738-5738. doi:10.1182/blood-2025-5738
- Nienhuis HLA, Bijzet J, Hazenberg BPC. The Prevalence and Management of Systemic Amyloidosis in Western Countries. Kidney Dis. 2016;2(1):10-19. doi:10.1159/000444206
- Lachmann HJ, Goodman HJB, Gilbertson JA, et al. Natural History and Outcome in Systemic AA Amyloidosis. N Engl J Med. 2007;356(23):2361-2371. doi:10.1056/NEJMoa070265
- Barrett CD, Dobos K, Liedtke M, et al. A Changing Landscape of Mortality for Systemic Light Chain Amyloidosis. JACC Heart Fail. 2019;7(11):958-966. doi:10.1016/j.jchf.2019.07.007
- Staron A, Zheng L, Doros G, et al. Marked progress in AL amyloidosis survival: a 40-year longitudinal natural history study. Blood Cancer J. 2021;11(8):139. doi:10.1038/s41408-021-00529-w




