Episode 142: Pediatric Intussusception
How is it defined?
- Intussusception occurs when a proximal segment of bowel telescopes into another segment.
- One of the most common pediatric abdominal emergencies, particularly in those between ages 3 months to 5 years.
- Misdiagnosed in up to 50% of cases on initial presentation.
- May lead to bowel ischemia and perforation; literature suggests mortality rates can reach 30%.
What is the underlying pathophysiology?
- Ileocolic intussusception involves the ileocecal junction; accounts for over 90% of cases.
- With intussusception, the mesentery and vasculature are dragged into the bowel, leads to lymphatic and venous congestion and intestinal edema. Bowel obstruction can also occur.
- If untreated, intussusception can lead to ischemia, bowel necrosis, perforation, and septic shock.
- 75-90% of cases are idiopathic with no identifiable trigger or mass.
- Lead point can cause intussusception when normal peristalsis traps the mass, which drags that part of the intestine into a distal segment.
- Lead point can be a polyp, cyst, tumor, diverticulum, hematoma, or vascular malformation. Typically associated with an underlying disorder, particularly in patients less than 3 months and older than 5 years.
- Disorders associated with development of a lead point: Meckel diverticulum, small bowel lymphoma, immunoglobulin A vasculitis, cystic fibrosis, inverted appendiceal stump, duplication cysts, and hemolytic uremic syndrome. Postoperative cases have also been documented.
How common is this?
- Most common cause of bowel obstruction in pediatric patients.
- Most commonly affects patients between 3 months to 5 years. Peak between 4-36 months.
- < 1% occur in those less than 3 months; around 10% of cases affect patients over 5 years.
- Up to 30% of patients develop intussusception following a bacterial or viral infection such as upper respiratory tract infection or otitis media. Likely associated with stimulation of lymphatic tissue within the intestinal tract and hypertrophy of Peyer patches
- Pathologic lead point more common in patients outside of 3 months to 5 years of age.
- Slight male predominance (3 males for every 2 females).
What should we look for on history and exam?
- Classic triad: abdominal pain, palpable sausage shaped mass in the right lower quadrant, currant jelly stool; occurs in 7.5-40%
- Separate triad of abdominal pain, emesis, and blood in the stool (either guaiac positive or visible blood) more common, with one retrospective study finding the triad was present in 89% of patients less than 1 year and 77% of children over 1 year (Mandeville).
- Abdominal pain most common symptom (80-100%).
- Typically severe, intermittent, progressive. Episodes occur at approximately 15–20-minute intervals; become more frequent and severe as the intussusception and obstruction worsen. Episodes of pain are often associated with crying; patient may draw up their legs towards the abdomen or develop pallor. May be asymptomatic between episodes.
- Vomiting in 60-94% and most commonly starts after the abdominal pain. Usually starts as non-bilious, but may progress to bilious emesis with obstruction.
- Bloody stools or currant jelly stools are often considered to be part of the classic presentation, but less than 25% of patients have hematochezia.
- Bloody stools more common in late stages of the disease with intestinal ischemia and in those less than 1 year.
- Over 60% will have occult blood present.
- Currant jelly stools occur in the setting of gross bleeding and mucosal sloughing and reflect intestinal necrosis.
- Sausage shaped mass palpable in up to 60%; may also be no palpable bowel in the right lower quadrant.
- Atypical presentations: up to 20% of patients have no abdominal pain; up to one third of patients have no gross or occult blood or identifiable abdominal mass.
- Younger patients may initially present with lethargy or altered mental status without abdominal pain or bleeding.
- Retrospective study of 300 patients with intussusception found 47% of patients less than 1 year presented with lethargy, compared to 26% of those between 1-3 years and 13% of those over 3 years (Mandeville).
- Consider intussusception in altered pediatric patient if no other cause is identified, particularly if GI symptoms also present. Also consider in patients with abdominal pain, particularly if intermittent, and emesis or bloody stools.
When is laboratory analysis recommended?
- Laboratory testing is not helpful in most patients with suspected intussusception.
- CBC, electrolytes, and renal and liver if concern for dehydration or volume depletion.
- If the patient is hemodynamically unstable or critically ill (e.g., peritonitis, septic shock), obtain lactate and blood cultures.
- Elevated lactate levels are associated with worse outcomes in intussusception.
Is an abdominal x-ray helpful for diagnosis?
- X-ray commonly used.
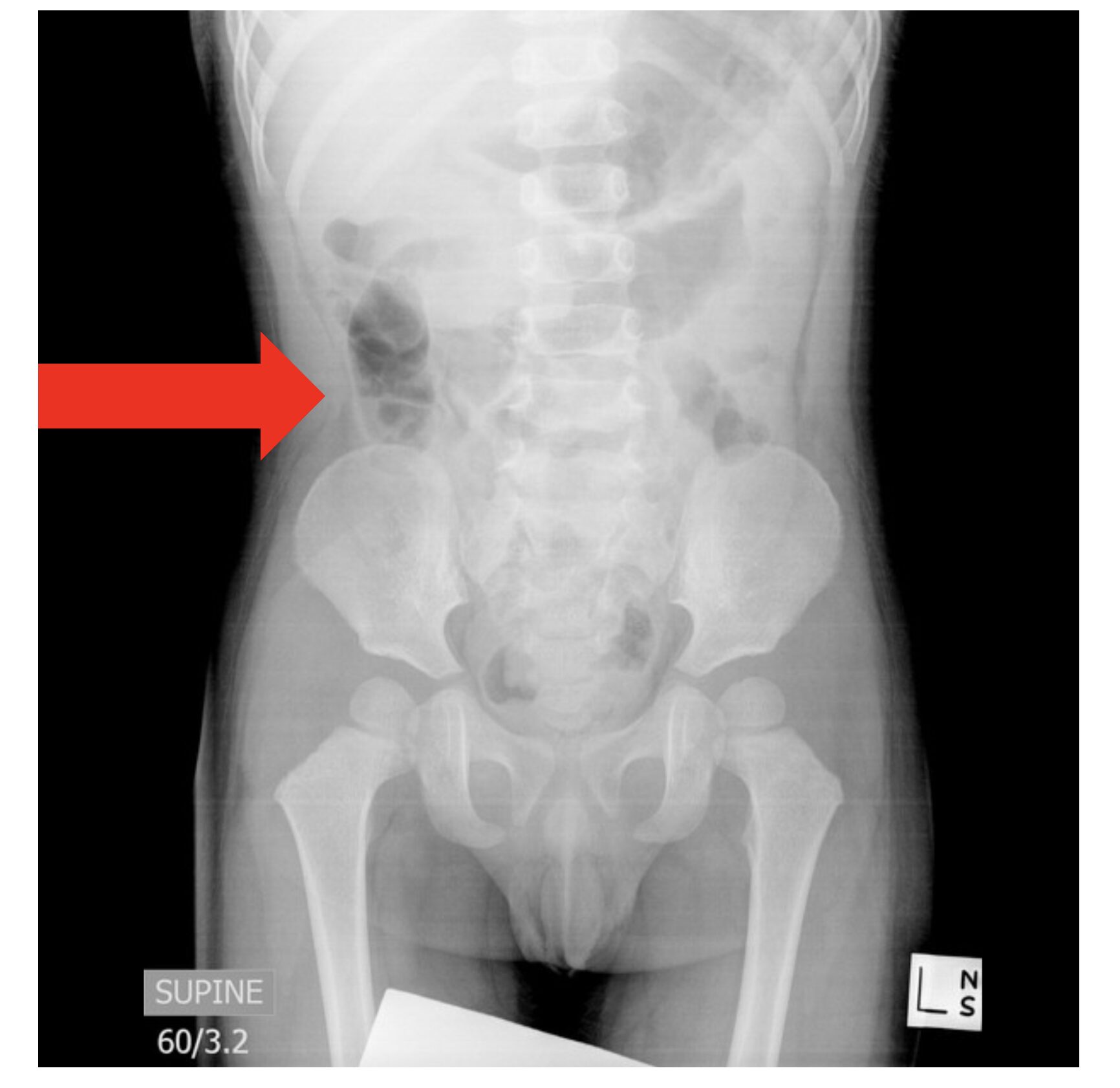
- Several findings suggest intussusception: distended bowel loops with absence of gas in the colon, target sign with two radiolucent concentric circles over the right kidney, meniscus or crescent sign (soft tissue density projecting into large bowel gas), obscurement of the liver margin, absence of air in the cecum (Figure 1).
- Air in the cecum or terminal ileum suggests against intussusception.
- X-ray has sensitivity between 25-60%, and up to 25% of cases have normal radiograph.
- Do not use to exclude diagnosis, but x-ray can be used if the patient is critically ill or concerned about perforation.
- X-rays can assess for pneumoperitoneum before treatment in stable patients.
Figure 1. Supine abdominal radiograph with mild dilatation of bowel loops in the right abdomen adjacent a subtle donut shaped soft tissue density (red arrow). No evidence of pneumoperitoneum. Case courtesy of Sally Ayesa, Radiopaedia.org, rID: 63984.
What is the preferred modality to diagnose intussusception?
- US is the diagnostic modality of choice.
- Literature suggests US has sensitivity and specificity between 92-100%.
- Most common sign is the target or donut sign present on the transverse view. US will show alternating areas of hyperechogenicity from the mesenteric adipose and hypoechogenicity from the bowel wall forming concentric rings. Usually present in the right side of the abdomen if ileocolic intussusception (Figure 2).
- US with color duplex can be helpful in looking for vascular flow.
- Pseudokidney sign is best seen in the longitudinal view (Figure 3). Hyperechoic tubular center surrounded on each side with a hypoechoic rim.
- Literature suggests POCUS can be used by emergency physicians with the lawnmower technique and high-frequency linear transducer.
- If the patient has a larger body habitus, use the curvilinear transducer.
- Other US findings: trapped peritoneal fluid in between the walls of the bowel, decreased or even absent color flow in the bowel wall, free fluid, free air, pneumatosis, and dilated loops of bowel suggesting obstruction.
- Fluoroscopy with contrast enema was previously used as reference standard for diagnosis.
- Classic signs are crescent and coiled spring signs.
- Crescent sign is presence of a curvilinear mass within the colon.
- Coiled spring sign is due to contrast in the colon lumen filling the space between the colon wall and the invaginated ileum
- CT is another imaging option and can identify any underlying etiology.
- Sensitivity close to 100%; may demonstrate a target sign, a sausage-shaped mass with differing layers of attenuation, and a kidney-like mass (Figure 4).
- CT more accurate than US in diagnosing pathologic lead points; may also be used if US unremarkable, if concern for perforation or peritonitis, or if pathologic lead point suspected.
Figure 2. Ultrasound examination of the right upper quadrant demonstrated bowel within the bowel, with a classic target sign. Case courtesy of Sally Ayesa, Radiopaedia.org, rID: 63984.

Figure 3. Longitudinal view of the intussuscepted bowel shows reniform shape (pseudokidney sign). Case courtesy of Tee Yu Jin, Radiopaedia.org, rID: 70238.

Figure 4. CT with extensive ileocecal intussusception extending up to the transverse colon. There is pelvic and susmesocolic free fluid, and free fluid within the invaginated bowels. Case courtesy of Maxime St-Amant, Radiopaedia.org, rID: 19235.

What are the key components of management?
- Treatment based on several factors: hemodynamic status, presence of perforation, and if the diagnosis is confirmed.
- If imaging evidence of ileocolic intussusception, normal vital signs, and no signs of perforation, nonoperative reduction is treatment of choice. May necessitate transfer.
- If the patient is unstable or has perforation, operative intervention, IV fluids/antibiotics needed. Operative intervention may also be needed if the resources and expertise necessary to perform non-operative intervention are not available and transfer is not feasible, but also in patients who fail non-operative intervention or for resection of a pathologic lead point.
- In the stable patient with no perforation, early nonoperative management reduces the risk of complications.
- May include hydrostatic enema using saline or contrast or pneumatic enema with sonographic or fluoroscopic guidance.
- External graded compression with intermittent visualization by US is another modality for reduction.
- This should be performed in a center with clinicians experienced in the technique and able to manage any complications such as perforation or tension pneumoperitoneum.
- Literature suggests sedation for reduction does not significantly impact the outcomes of attempted reduction and may be utilized is necessary.
- Prior to reduction: if dehydrated, administer IV fluids. Consider surgical consultation due to the risk of perforation and tension pneumoperitoneum. Antibiotics prior to or during reduction are not needed, except if the patient is unstable or critically ill.
- In general US with hydrostatic reduction or external graded compression is the treatment of choice if available, but fluoroscopic guidance can be used for pneumatic reduction as well.
- Success rates range between 80% to 95%.
- Decision to use hydrostatic or pneumatic reduction depends on the clinician and center performing the procedure.
- Reduction success rates may also be higher with administration of glucagon or atropine, which may relax colonic smooth muscle (Franken, Liu).
- Several factors associated with lower likelihood of successful reduction: age < 1 year or > 5 years, presence of small bowel obstruction or ascites, absence of abdominal pain, fever, rectal bleeding, US evidence of left sided intussusception, absence of doppler flow, presence of a pathologic lead point, and symptoms > 24-48 hours.
- These are not contraindications to a reduction attempt. Hematochezia or currant jelly stool also not a contraindication to nonoperative reduction.
- Reduction confirmed based on patient symptoms and imaging.
- If reduction was partly successful (intussusception moved but did not completely reduce) and the patient is stable, repeated attempt at reduction can be performed within 30 minutes to 24 hours.
- Repeat reduction attempt is successful in about half of cases.
- If several nonoperative reduction attempts are unsuccessful or if the patient becomes unstable, emergent operative intervention is recommended.
- There are risks associated with attempted reduction.
- Bowel perforation (<4% of cases), usually in distal part of the intussusception in the transverse colon.
- Risk factors for perforation include age < 6 months, symptoms > 3 days, the presence of small bowel obstruction, and use of higher pressures during the reduction attempt.
- Air from pneumatic reduction resulting in perforation is generally less harmful than contrast within the peritoneal cavity. Tears in the colonic wall are also usually smaller compared to those with contrast.
Are there any benefits to repeating an ultrasound on patients with intussusception?
- Up to 13% of cases self-reduce.
- In patients diagnosed with intussusception who become asymptomatic before attempted reduction, a repeat US can be performed. If the intussusception is no longer visible, no further treatment is needed.
What are key considerations following successful reduction?
- Literature does not demonstrate benefit with antibiotics before, during, or after reduction in patients who are stable and have no evidence of peritonitis (Kelley-Quon). Antibiotics are recommended in patients with evidence of sepsis or need for operative intervention (e.g., peritonitis).
- Disposition:
- Classically children were admitted to the hospital for 24-48 hours to observe for PO tolerance, complications, and recurrence of intussusception.
- Up to 10% of patients will experience recurrence; highest rates in those > 1 year, those with pathologic lead points, and prior recurrence.
- More recent literature suggests up to 4% of patients with successful reduction experience recurrence in 48 hours.
- Literature suggests a brief observation period in the ED following successful reduction is appropriate: no difference in recurrence rates between discharged patients and those admitted for observation (Litz, Sujka).
- Meta-analysis and several observational studies suggest that patients with uncomplicated reduction who are afebrile, stable, PO tolerant, and asymptomatic can be discharged home, with no increase in mortality, need for operative intervention, intussusception recurrence rates, and return rates to the ED (Litz, Sujka).
- If discharging the patient, provide clear return precautions, including return if symptoms recur.
- If the patient returns with recurrent symptoms, US is the imaging modality of choice. Patients with recurrence can be treated again nonoperatively, but if the patient has a focal lead point, multiple recurrences, is unstable, or has perforation, operative intervention is needed (Navarro).
- Steroids have been proposed to prevent recurrence in those with idiopathic intussusception, especially with lymphoid hyperplasia, but data are controversial (Gluckman, Lin, Shteyer).
Summary
- Intussusception involves the telescoping of one part of the intestine into another; this may lead to bowel obstruction and perforation if untreated.
- Peak age between 4 months to 3 years, and most cases involve the ileocolic junction.
- Cases are often idiopathic, but a pathologic lead point may come from a mass or underlying disorder.
- Presentation usually includes sudden, severe, intermittent crampy abdominal pain associated with vomiting.
- Classic triad of abdominal pain, palpable mass, and currant jelly stools is not common. Younger patients may present atypically with altered mental status or lethargy with or without abdominal pain, though this is uncommon.
- Ultimately, consider intussusception in pediatric patients with abdominal pain, emesis, bloody stools, a sausage-shaped mass, or altered mental status or lethargy if no other causative etiology is found.
- Laboratory testing is not diagnostic but can be helpful if the patient is hypovolemic or critically ill.
- Ultrasound is the imaging modality of choice for diagnosis. Plain radiograph can be used to evaluate for pneumoperitoneum but should not be used to exclude a diagnosis of intussusception.
- Management is based on the patient’s presentation, hemodynamic status, and imaging. If unstable or if peritonitis is present, emergent surgical consultation for operative intervention is needed.
- For patients who are stable with no peritonitis, treatment of choice is non-operative reduction with ultrasound or fluoroscopy.
- Following a successful reduction, patients who are well appearing, able to tolerate oral intake, and have no recurrence of symptoms may be discharged with close return precautions without admission.
References
- Long B, Easter J, Koyfman A. High risk and low incidence diseases: Pediatric intussusception. Am J Emerg Med. 2025 May;91:37-45.
- Charles T, Penninga L, Reurings JC, Berry MC. Intussusception in Children: A Clinical Review. Acta Chir Belg. 2015 Sep-Oct;115(5):327-33
- Waseem M, Rosenberg HK. Intussusception. Pediatr Emerg Care. 2008 Nov;24(11):793-800.
- Jiang J, Jiang B, Parashar U, et al. Childhood Intussusception: A Literature Review. Plos one. 2013;8:e68482.
- Lehnert T, Sorge I, Till H, Rolle U. Intussusception in children—clinical presentation, diagnosis and management. Int J Colorectal Dis. 2009;24:1187–1192.
- Applegate KE. Intussusception in children: evidence-based diagnosis and treatment. Pediatr Radiol. 2009 Apr;39 Suppl 2:S140-3.
- Mandeville K, Chien M, Willyerd FA, et al. Intussusception: clinical presentations and imaging characteristics. Pediatr Emerg Care. 2012;28:842.
- Daneman A, Navarro O. Intussusception. Pediatr Radiol. 2004;34(2):97–108.
- Daneman A, Navarro O. Intussusception. Part 2: An update on the evolution of management. Pediatr Radiol. 2004 Feb;34(2):97-108; quiz 187.
- Navarro O, Daneman A. Intussusception part 3: diagnosis and management of those with an identifiable or predisposing cause and those that reduce spontaneously. Pediatr Radiol. 2004;34:305–312.
- Daneman A, DJ A. Intussusception: issues and controversies related to diagnosis and reduction. Radiol Clin North Am. 1996;34:743Y756.
- Berlin L. Reducing the intussuscepted colon. Am J Roentgenol. 1998;170:1161–1163
- Meier DE, Coln CD, Rescorla FJ, et al. Intussusception in children: international perspective. World J Surg. 1996;20:1035–1039.
- Lochhead A, Jamjoom R, Ratnapalan S. Intussusception in children presenting to the emergency department. Clin Pediatr (Phila). 2013;52:1029.
- Tsou PY, Wang YH, Ma YK, et al. Accuracy of point-of-care ultrasound and radiology-performed ultrasound for intussusception: A systematic review and meta-analysis. Am J Emerg Med. 2019 Sep;37(9):1760-1769.
- Franken EA Jr, Smith WL, Chernish SM, et al. The use of glucagon in hydrostatic reduction of intussusception: a double-blind study of 30 patients. Radiology. 1983;146:687.
- Liu X, Yu HK, Gu LX, et al. Atropine Premedication Facilitates Ultrasound-Guided Reduction by Saline Enema in Children With Intussusception. Front Pharmacol. 2019;10:43.
- Sadigh G, Zou KH, Razavi SA, et al. Meta-analysis of Air Versus Liquid Enema for Intussusception Reduction in Children. AJR Am J Roentgenol. 2015;205:W542.
- Litz CN, Amankwah EK, Polo RL, et al. Outpatient management of intussusception: a systematic review and meta-analysis. J Pediatr Surg. 2019;54:1316.
- Gluckman S, Karpelowsky J, Webster AC, McGee RG. Management for intussusception in children. Cochrane Database Syst Rev. 2017 Jun 1;6(6):CD006476.
- Lin SL, Kong MS, Houng DS. Decreasing early recurrence rate of acute intussusception by the use of dexamethasone. Eur J Pediatr. 2000;159:551.
- Sujka JA, Dalton B, Gonzalez K, et al. Emergency department discharge following successful radiologic reduction of ileocolic intussusception in children: A protocol based prospective observational study. J Pediatr Surg. 2019;54:1609.
- Shteyer E, Koplewitz BZ, Gross E, Granot E. Medical treatment of recurrent intussusception associated with intestinal lymphoid hyperplasia. 2003;111:682.
- Melvin JE, Zuckerbraun NS, Nworgu CR, et al. Management and Outcome of Pediatric Patients With Transient Small Bowel-Small Bowel Intussusception. Pediatr Emerg Care. 2021 Mar 1;37(3):e110-e115.




