
Authors: Alessia Cooney, DO (EM Resident Physician, North Shore/LIJ, Manhasset, NY); Alexander Nello, DO (EM Attending Physician, North Shore/LIJ, Manhasset, NY) // Reviewed by: Sophia Görgens, MD (EM Physician, Yale University, CT); Cassandra Mackey, MD (Assistant Professor of Emergency Medicine, UMass Chan Medical School)
Welcome to EM@3AM, an emDOCs series designed to foster your working knowledge by providing an expedited review of clinical basics. We’ll keep it short, while you keep that EM brain sharp.
A 45-year old African American woman presents to the ED with progressive fatigue over the past week and has experienced intermittent episodes of severe hand pain that typically self-resolve. She has also noted a worsening headache over the last day. Her blood pressure is 197/105 mm Hg and heart rate is 90 bpm. The physical exam is notable for smooth and taut skin on the patient’s face and hands. Laboratory values show a creatinine of 3.1 mg/dL, which is a significant change from lab studies performed 1 year ago. Her ECG is within normal limits.
What is the likely diagnosis?
Answer: Scleroderma
Background:
- Scleroderma, also known as systemic sclerosis, is a rare connective tissue disorder1
- Leads to a build of fibrous tissue in the skin, blood vessels, and/or organs.1
- Autoimmune disorder thats pathogenesis is not clearly understood
- Suspected to be secondary to endothelial dysfunction, microvascular injury, immune dysregulation, autoantibody production and progressive fibrosis driven by activated myofibroblasts.2
- Affects
- Primarily middle aged individuals3
- Females and individuals of African ancestry
- Females are 3 to 14 times more likely to develop scleroderma when compared to males4,5
- African Americans are two times more likely to develop scleroderma when compared to Caucasian individuals4,5
- Individuals with environmental exposure to silica and organic solvents6
- Individuals with specific human leukocyte antigen (HLA) subtypes in the major histocompatibility complex (MHC) region7
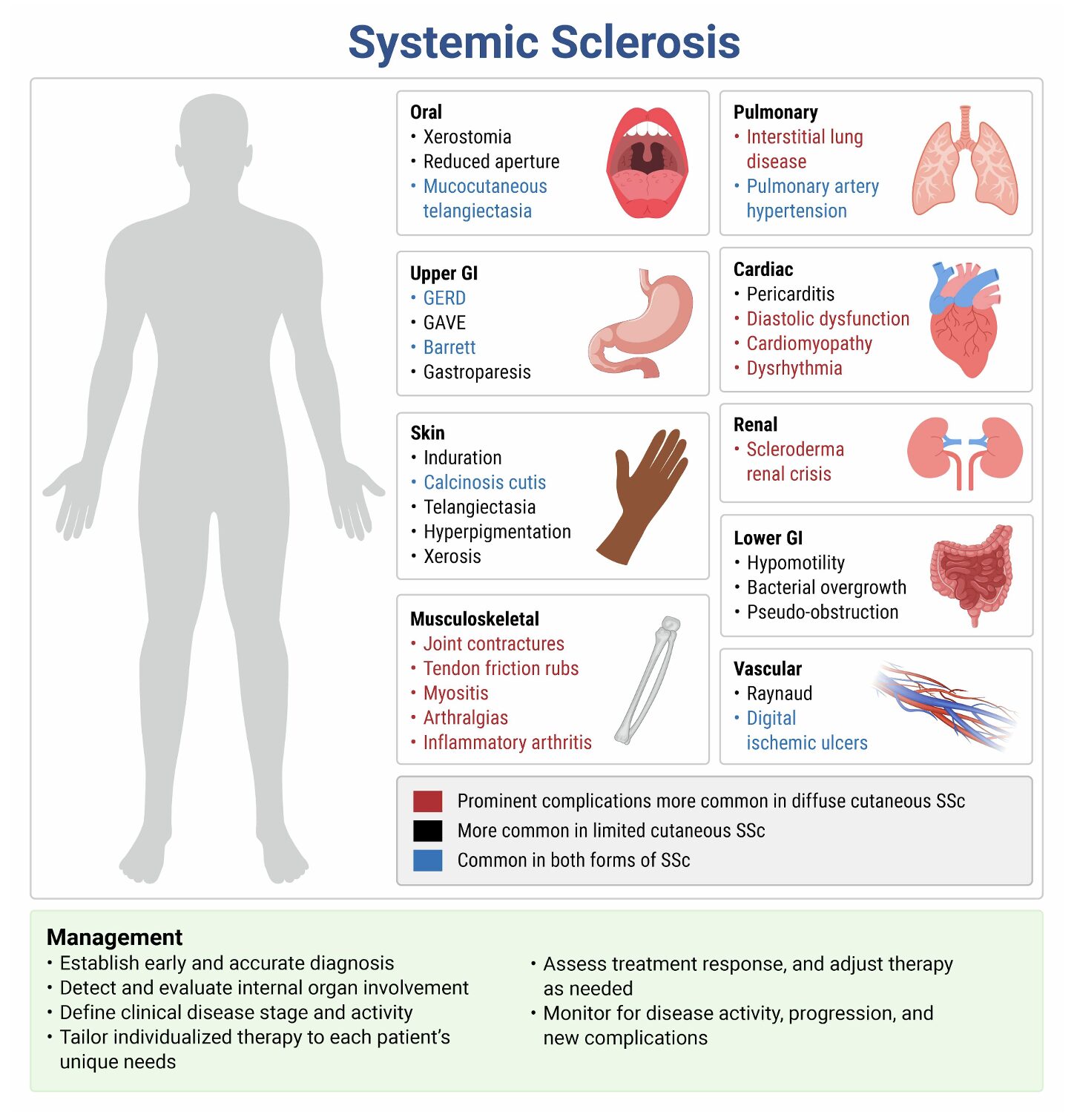
- Scleroderma can be divided into localized and systemic sclerosis.
- Localized disease affects the skin and subcutaneous tissues with individuals having a stiffened appearance to their skin1
- Systemic sclerosis causes multisystem involvement.1
- Based on clinical and serologic criteria, systemic sclerosis can be further classified into
- Limited, formerly CREST syndrome
- CREST syndrome has five key features: Calcinosis, Raynaud’s phenomenon, Esophageal dysmotility, Sclerodactyly, and Telangiectasia.1
- Diffuse
- Limited, formerly CREST syndrome
- Scleroderma has the highest mortality among rheumatologic disease
- Individuals are 3 to 4 times more likely to die compared to the general population.8
- Prognosis is directly impacted by the degree of internal organ involvement.9,10
- Based on clinical and serologic criteria, systemic sclerosis can be further classified into
Complications:
- Scleroderma Renal Crisis
- Risk factors: Diffuse skin involvement, early disease progression, presence of antibodies to RNA polymerase III, exposure to doses of greater than 15 mg/kg of corticosteroids, new onset anemia, pericarditis, tendon friction rub, and congestive heart failure.11,12
- Epidemiology: Up to 75% of cases occur within the first four years of disease diagnosis.12 May present as the first manifestation of scleroderma in 20% of cases.11
- Pathophysiology: Suspected to be the consequence of structural changes to the endothelial cells of blood vessels which supply the kidneys. Decreased blood flow secondary to fibrin deposition and intimal thickening leads to renal vasospasm and ischemia which activates the renin-angiotensin-aldosterone system (RAAS) to cause an increase in blood pressure.12
- Clinical Presentation:12
- Acute onset of severe hypertension
- Acute renal failure (ie. oliguria vs. anuria)
- Thrombocytopenia
- Microangiopathic hemolytic anemia
- Changes in vision
- Changes in mental status
- Congestive heart failure
- Evaluation:
- CBC
- CMP
- UA
- Renal biopsy if atypical presentation12
- Treatment:
- ACE-inhibitors12
- Start with short acting ACE-inhibitor like Captopril
- Captopril 6.25 – 12.5 mg PO TID13
- Aim to reduce BP by about 20 mm Hg in 24 hours with the goal of obtaining BP of 120/70 mm Hg within 72 hours while avoiding hypotension.
- Goal to reduce BP rapidly through inhibiting RAAS
- Start with short acting ACE-inhibitor like Captopril
- Dihydropyridine Calcium Channel Blocker12
- Can be used to further reduce BP if max doses of ACE-inhibitors are used.
- Amlodipine and nifedipine are first line agents.14
- Consult Nephrology12,13
- Patient will require admission to carefully monitor blood pressure for approximately 72 hours
- ACE-inhibitor administration should not be delayed until nephrology consultation if there is a high clinical suspicion for scleroderma renal crisis as early initiation has been associated with better prognosis, with one year survival rates improving from 10% to 85%.9
- Avoid diuretics as this further stimulates RAAS
- 50% of patients may require dialysis
- Renal transplantation may be considered greater than 24 months after initial injury as renal recovery can often be a prolonged process.
- Patient will require admission to carefully monitor blood pressure for approximately 72 hours
- Disposition
- Always requires ICU admission due to frequent blood pressure monitoring and potential need for dialysis.
- ACE-inhibitors12
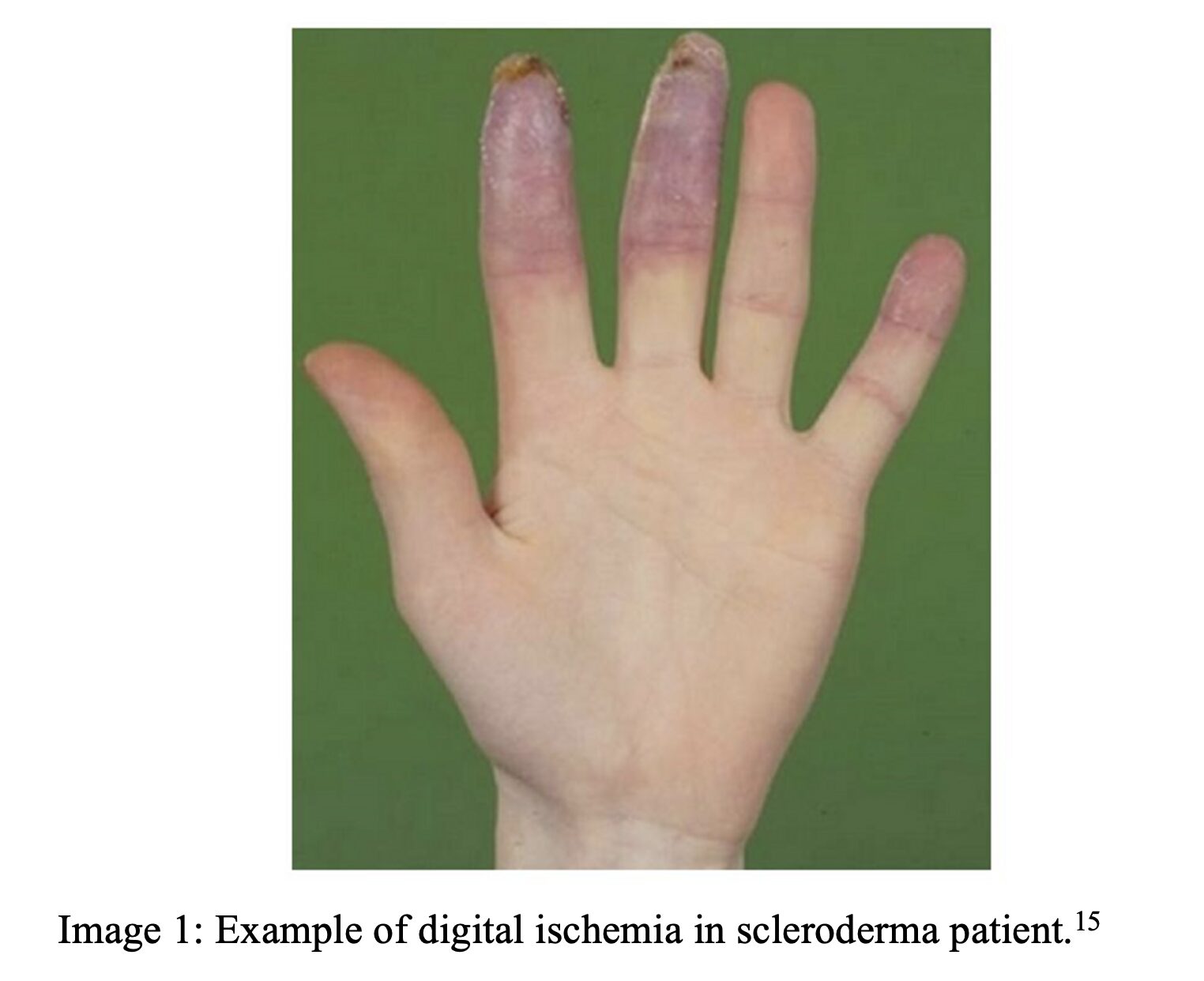
- Digital Ischemia/Ulceration
- Risk factors: Smoking, history of digital ulcers, positive autoantibodies (anti-centromere, ANCA, and anti-phospholipid antibodies), elevated inflammatory markers and known microvascular disease.11
- Epidemiology: 30% of patients annually will experience digital ischemia.15
- Pathophysiology: Migration of smooth muscle cells into the intimal layer of the microvasculature leads to differentiation into myofibroblast which secrete an extracellular matrix causing narrowing of the intravascular lumen thereby hindering blood flow.15 Some individuals may experience reversible vasospasm while others may experience vessel occlusion overtime.11 Decreased microvascular perfusion causes tissue ischemia leading to ulcer formation.
- Clinical Presentation:
- Painful wounds on the finger tips and dorsal aspect of the hands
- Necrotic/gangrenous wounds
- Delayed capillary refill in digits
- Paresthesias
- Blue or white discoloration of digits
- Evaluation:
- If digital ulceration is present, consider obtaining x-ray vs. MRI to evaluate for
- The prevalence of osteomyelitis reaches approximately 42% in patients with systemic sclerosis and infected digital ulcerations.16
- If digital ischemia is present, consider whether the ischemia is acute vs. chronic
- Consider CTA imaging vs. Duplex US
- Consider vascular consult
- Treatment
- Antiplatelet Agents15
- Aspirin 81 mg daily
- Limited evidence on the efficacy of using Clopidogrel alone or in addition to aspirin.
- Antiplatelet Agents15
- If digital ulceration is present, consider obtaining x-ray vs. MRI to evaluate for
- Vasodilator Therapy11,15
- Calcium Channel Blockers – Dihydropyridine
- Nifedipine – 10-20 mg three times a day14
- Amlodipine – specific dosing for scleroderma patients is limited.17,9
- Phosphodiesterase-5 Inhibitors14
- Sildenafil – 20 mg three times a day
- Tadalafil – once daily dosing, but specific doses vary
- Prostacyclin Infusion
- Iloprost or , Epoprostenol, or Treprostinil
- Iloprost regimen18
- Day 1: 0.5 ng/kg/min
- Increase by 0.5 ng/kg/min aliquots every 30 minutes (based on tolerability) up to a maximum of 2.0 ng/kg/min
- Days 2 and 3: Repeat dose titration
- Day 4: Starting dose is highest tolerated dose from Day 3
- Regimen to last 3-8 days for approximately 6 hours per day
- Does not require a central line
- Epoprostenol regimen19
- Start at 1-2 ng/kg/min and titrate upward in 1-2 ng/kg/min increments based on tolerability
- Requires a central line
- Potent vasodilators that also have inhibitory properties on smooth muscle proliferation and platelet aggregation.
- While a nephrology consultation is not needed for the initiation of vasodilator therapy, consider consulting rheumatology when starting prostacyclin therapy given the complexity of administering and monitoring the infusion.17,18
- Iloprost regimen18
- Antibiotics
- Not routinely needed unless concurrent infection is present
- Disposition
- Depends on the degree of ischemia. Patients with acute critical digital ischemia should be admitted, while patients with mild to moderate digital ulcerations can be discharged home.17
- Iloprost or , Epoprostenol, or Treprostinil
- Calcium Channel Blockers – Dihydropyridine
- Respiratory – Interstitial Lung Disease (ILD)
- Risk factors: diffuse systemic sclerosis, elderly, male, anti-Scl-70/anti-topoisomerase I antibody positivity, absence of anti-centromere antibodies.20,21
- Epidemiology: More common within the first 3-5 years of disease progression. ILD is the most common pulmonary complication and the leading cause of death in systemic sclerosis, contributing to approximately 35% of scleroderma-related deaths.22,23
- Pathophysiology: Combination of immune dysregulation, vascular injury, and aberrant tissue repair that culminates in excessive extracellular matrix deposition and irreversible structural damage to the pulmonary tissue and pulmonary vasculature.24
- Clinical Presentation:
- Progressive dyspnea on exertion
- Non-productive cough
- Hypoxemia requiring supplemental oxygen
- Acute respiratory distress
- Evaluation:
- High resolution non-contrast CT scan of the chest25
- Pulmonary Function Test (PFT)
- This test is not needed for diagnosis alone and is not typically performed in the ED but should be obtained outpatient to have as a baseline and for monitoring.9
- Autoantibody testing (anti-Scl-70, anti-centromere)
- Treatment:
- Mycophenolate mofetil26
- Inhibits DNA synthesis and cell proliferation with lymphocytes being the primary target
- 3 grams per day
- Given PO9
- Cyclophosphamide26
- First line alternative
- IV preferred over oral route as it was found to have better efficacy and lower risk of urothelial toxicity.26
- IV dosing: 500–750 mg/m² IV every 4 weeks for 6 months27
- Oral dosing: 2 mg/kg per day for 12 months26
- Steroids
- Avoid steroids as current evidence suggests there is moderate risk for triggering scleroderma renal crisis by initiating steroids and a very low amount of evidence suggesting benefit in treatment for ILD.27
- Disposition
- Indications for admission include acute exacerbation of respiratory distress with new infiltrates on imaging, new or worsening oxygen requirement, hemodynamic instability and/or suspected infection.28
- Mycophenolate mofetil26
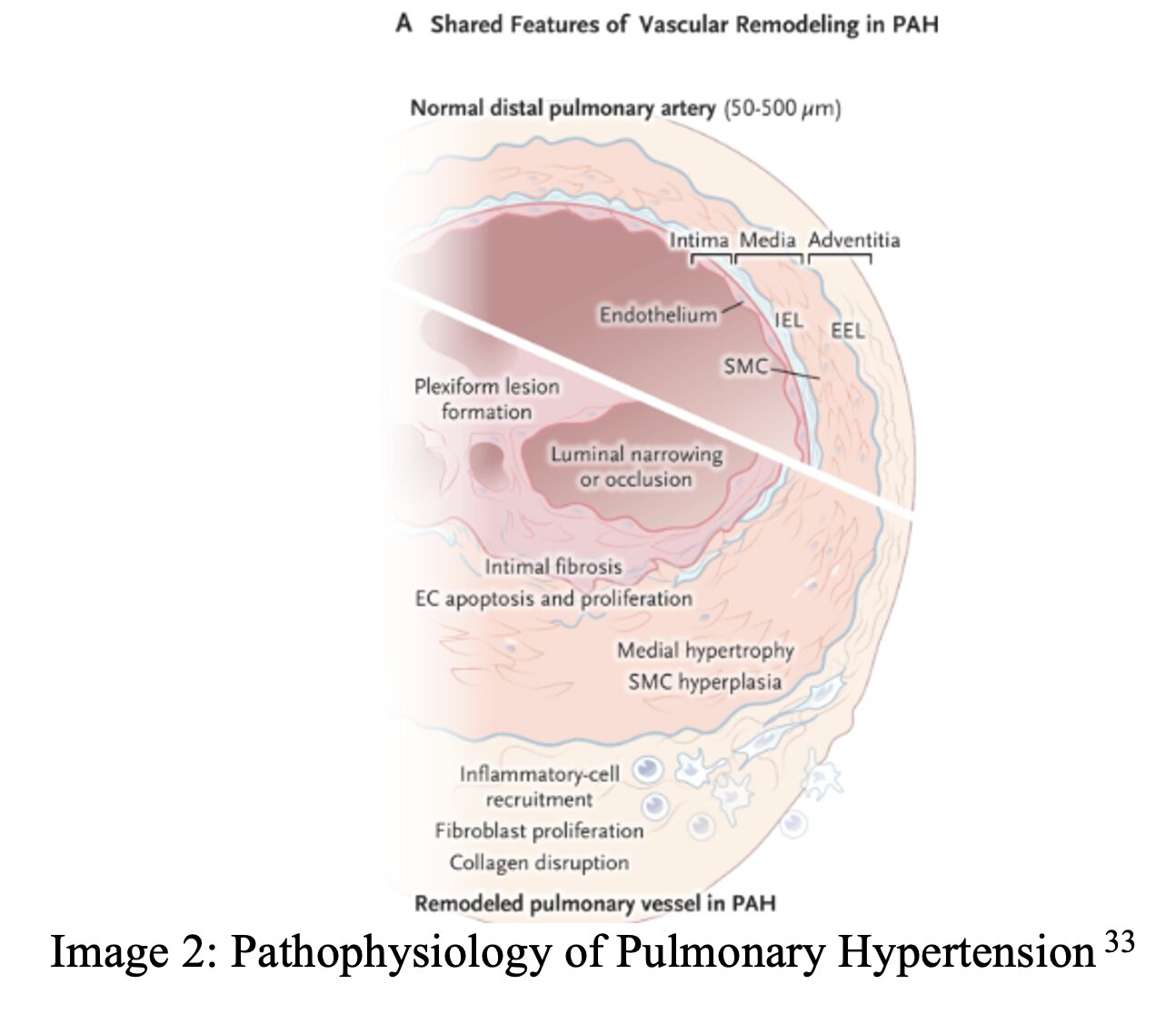
- Respiratory – Pulmonary Hypertension
- Risk factors: Older age, post-menopausal women, decline in diffusing capacity of the lung for carbon monoxide, anti-centromere antibody positivity, telangiectasias, and high brain natriuretic peptide.29,30 Isolated pulmonary hypertension is more likely to develop in patients with limited cutaneous systemic sclerosis after a prolonged period of disease duration, commonly 10-15 years after disease onset. Patients with diffuse cutaneous systemic sclerosis often develop pulmonary hypertension in the context of other pulmonary diseases.31
- Epidemiology: 8-15% of patients with scleroderma develop pulmonary hypertension. Pulmonary hypertension is the second leading cause of death in this population.9,32
- Pathophysiology: In systemic sclerosis, immune-mediated endothelial injury promotes abnormal vascular remodeling, resulting in gradual narrowing of pulmonary arterioles and the development of pulmonary arterial hypertension.9
- Clinical Presentation:
- Fatigue and dyspnea on exertion
- Chest discomfort
- Syncope or presyncope (particularly concerning for advanced disease)
- Palpitations
- Lower extremity edema and jugular venous distension(evidence of right heart failure)
- Acute respiratory distress
- Evaluation:
- ECG
- Pro-BNP
- Chest x-ray
- CTPA (pulmonary angiography)34
- The timing of this test is better for evaluating the pulmonary arteries.
- Echocardiogram
- Useful for stratifying disease probability which impacts further workup.
- Inevitably, individuals with pulmonary arterial hypertension will develop right heart failure, so obtaining an echo will determine if/when heart failure has developed.34
- Treatment:
- Avoid beta blockers and calcium channel blockers for tachydysthymias35
- Patients with pulmonary hypertension rely on heart rate to maintain cardiac output.
- Tachycardia is not well tolerated in pulmonary hypertension so consider immediate cardioversion for any tachydysrythmias36
- Avoid acidosis (induces pulmonary vasoconstriction)36
- Avoid intubation and noninvasive positive pressure ventilation36
- Avoid hypoxia (increases pulmonary vasoconstriction) and hypercapnia (increases pulmonary resistance)36
- Increase cardiac output/RV function37
- Dobutamine: starting dose of 0.5 to 1.0 mcg/kg/min and can increase to a maximum of 40 mcg/kg/min38
- Milrinone: Loading dose of 25 to 50 mcg/kg (loading dose given over 10 minutes) followed by continuous infusion of 0.375 to 0.75 mcg/kg/min39
- Optimize intravascular volume37
- Usually patients do not require IV fluids
- Assess volume status using point of care ultrasound
- Give 250 cc bolus if hypovolemic
- Consider gentle diuresis if hypervolemic
- Giving excess fluid worsens right ventricular dilatation, causing increased wall stress and impairing coronary perfusion which worsens cardiac output
- Norepinephrine is the first vasopressor of choice if the patient becomes hypotensive despite gentle fluid resuscitation.37
- Disposition
- Often these patients require admission if in acute exacerbation and may need ICU level of care.
- Indications for admission include acute or decompensated right heart failure, syncope, arrhythmia, new or worsening oxygen requirement, hemodynamic instability and/or new or worsening end organ damage.40
- Avoid beta blockers and calcium channel blockers for tachydysthymias35
- Intestinal Pseudo-Obstruction
- Risk factors: Opiate use, females, limited cutaneous systemic sclerosis11,41
- Epidemiology: Affects 4-10% of scleroderma patients.9 There is a high rate of recurrence; however approximately 70% of cases resolve spontaneously.42
- Pathophysiology: Obstructive symptoms without mechanical obstruction due to dysfunction in intestinal propulsion.11 Intestinal propulsion dysfunction is caused by multiple factors. There is a degeneration of the enteric nervous system, specifically a loss of interstitial cells of Cajal which act as pacemaker cells to help generate and propagate intestinal movement. Smooth muscle atrophy and fibrosis that replaces normal tissue also impact motility. Microvascular abnormalities also contribute to tissue ischemia and subsequent damage.43,44
- Clinical Presentation:
- Inability to tolerate PO intake
- Constipation/inability to pass gas
- Abdominal pain and distension
- Evaluation:
- Upright Abdominal X-ray
- Multiple air fluid levels and dilated loops of bowel that will lack a transition point or obstructing lesion.45
- CT abdomen/pelvis
- Upright Abdominal X-ray
- Treatment:
- NPO42
- NG Tube42
- Indicated for patients with active nausea and vomiting, severe abdominal distension, inability to tolerate PO intake or those who have failed conservative measures.43
- IV Hydration43
- Consider antibiotics if suspect small intestinal bacterial overgrowth (SIBO) 11
- Rifaximin 800-1200 mg in divided doses for 7 to 14 days46
- Ciprofloxacin 250 mg BID for 7 to 10 days46
- Both medications can be given PO.
- Prokinetic agents14
- Domperidone, Metoclopramide, Mosapride, Prucalopride, Linaclotide
- Domperidone is considered the first line agent. Dosing would be 10 mg TID PO.47
- Refractory case may benefit from octreotide with erythromycin
- This combination works because it produces more comprehensive prokinetic activity as octreotide inhibits gastric emptying while stimulating the small bowel, whereas erythromycin does the opposite.48
- Domperidone, Metoclopramide, Mosapride, Prucalopride, Linaclotide
Key Points:
- Scleroderma (systemic sclerosis) is a rare, high-mortality connective tissue disease where prognosis depends on extent of internal organ involvement.
- Major acute complications include renal crisis, digital ischemia/ulceration, interstitial lung disease, pulmonary hypertension, and intestinal pseudo-obstruction.
- Vascular dysfunction and fibrosis drive disease pathology causing hypertension, ischemia, organ failure, and impaired motility.
- Management focuses on early detection, avoiding triggers (steroids), targeted therapies (ACE inhibitors, immunosuppression, vasodilators), and multidisciplinary care to reduce complications and improve outcomes.
 A 54-year-old woman presents after a fall. She notes she usually walks with a cane but did not have it handy today. You notice contractures of the fingers bilaterally, and her skin is thick and hard. When you range her elbows, you can hear what sounds like crepitus along the triceps tendon during extension. What other clinical features are you likely to find in this patient based on the underlying diagnosis?
A 54-year-old woman presents after a fall. She notes she usually walks with a cane but did not have it handy today. You notice contractures of the fingers bilaterally, and her skin is thick and hard. When you range her elbows, you can hear what sounds like crepitus along the triceps tendon during extension. What other clinical features are you likely to find in this patient based on the underlying diagnosis?
A) Butterfly-shaped rash across the nose and cheeks
B) Fingers turn white, red, and blue in response to cold
C) Multiple extremity and spine deformities due to brittle bones
D) Rectovaginal fistula
Answer: B
This patient is presenting with systemic sclerosis, also known as scleroderma. This disease is caused by excessive accumulation of collagen and matrix in various tissues. Skin involvement is the most clinically apparent feature, manifesting as skin thickening and hardening. Early in the disease, patients may have nonpitting edema of the extremities and pruritus, which eventually progresses to such significant skin tightness that patients develop contractures (commonly in the hands) and digital ulcers. Scleroderma also affects the musculoskeletal system, leading to arthralgia, arthritis, and tendon friction rubs. The disease leads to widespread complications with problems in multiple organ systems, from interstitial lung disease to kidney impairment, to gastrointestinal dysmotility, and then vascular disease. Raynaud phenomenon is virtually always present in patients with scleroderma and is characterized by reversible vasospasm in the digital arteries of the hands and feet. This is often triggered by cold or stress and causes a characteristic white, red, and blue discoloration.
A butterfly-shaped rash across the nose and cheeks (A) describes a malar rash, which occurs classically in systemic lupus erythematosus but also occurs in rosacea, dermatomyositis, and pellagra.
Deformities caused by fractures in brittle bones (C) describes osteogenesis imperfecta, which is due to defective collagen production.
A rectovaginal fistula (D) may be a complication of cancer, radiation, or inflammatory bowel disease.
References:
- Horowitz D. Scleroderma: MedlinePlus Medical Encyclopedia. Medlineplus.gov. Published 2017. https://medlineplus.gov/ency/article/000429.htm
- Jimenez SA, Mendoza FA, Piera-Velazquez S. A review of recent studies on the pathogenesis of Systemic Sclerosis: focus on fibrosis pathways. Frontiers in Immunology. 2025;16. doi:https://doi.org/10.3389/fimmu.2025.1551911
- Alba MA, Velasco C, Simeón CP, et al. Early- versus late-onset systemic sclerosis: differences in clinical presentation and outcome in 1037 patients. Medicine (Baltimore). 2014;93(2):73-81. doi:10.1097/MD.0000000000000018
- Kwon OC, Han K, Park MC. Sex differences in the risk of incident systemic sclerosis: a nationwide population-based study with subgroup analyses. Sci Rep. 2025;15(1):8803. Published 2025 Mar 14. doi:10.1038/s41598-024-84856-5
- Kotamarti R, Hackshaw KV. Systemic sclerosis and scleroderma renal crisis in African American patients. J Natl Med Assoc. 2025;117(3):179-184. doi:10.1016/j.jnma.2025.04.006
- Marie I, Gehanno JF. Environmental risk factors of systemic sclerosis. Semin Immunopathol. 2015;37(5):463-473. doi:10.1007/s00281-015-0507-3
- Tsou PS, Sawalha AH. Unfolding the pathogenesis of scleroderma through genomics and epigenomics. J Autoimmun. 2017;83:73-94. doi:10.1016/j.jaut.2017.05.004
- Nikpour M, Baron M. Mortality in systemic sclerosis: lessons learned from population-based and observational cohort studies. Curr Opin Rheumatol. 2014;26(2):131-137. doi:10.1097/BOR.0000000000000027
- Volkmann ER, Andréasson K, Smith V. Systemic sclerosis. Lancet (London, England). 2022;401(10373). doi:https://doi.org/10.1016/S0140-6736(22)01692-0
- Hinchcliff M, Varga J. Systemic sclerosis/scleroderma: a treatable multisystem disease. Am Fam Physician. 2008;78(8):961-968.
- Liebowitz J. A Primer on the Management of Scleroderma Emergencies – The Rheumatologist. The Rheumatologist. Published September 28, 2023. Accessed January 17, 2026. https://www.the-rheumatologist.org/article/a-primer-on-the-management-of-scleroderma-emergencies/
- Vaidya PN, Basyal B, Finnigan NA. Scleroderma And Renal Crisis. PubMed. Published 2020. https://www.ncbi.nlm.nih.gov/books/NBK482424/
- Scleroderma – WikEM. Wikem.org. Published 2016. https://wikem.org/wiki/Scleroderma
- Asano Y, Jinnin M, Kawaguchi Y, et al. Diagnostic criteria, severity classification and guidelines of systemic sclerosis. J Dermatol. 2018;45(6):633-691. doi:10.1111/1346-8138.14162
- Schiopu E, Impens AJ, Phillips K. Digital Ischemia in Scleroderma Spectrum of Diseases. International Journal of Rheumatology. 2010;2010:1-8. doi:https://doi.org/10.1155/2010/923743
- Giuggioli D, Manfredi A, Colaci M, Lumetti F, Ferri C. Osteomyelitis complicating scleroderma digital ulcers. Clin Rheumatol. 2013;32(5):623-627. doi:10.1007/s10067-012-2161-7
- Hughes M, Allanore Y, El Aoufy K, et al. A Practical Approach to the Management of Digital Ulcers in Patients With Systemic Sclerosis: A Narrative Review. JAMA Dermatol. 2021;157(7):851–858. doi:10.1001/jamadermatol.2021.1463
- Ingegnoli F, Schioppo T, Allanore Y, et al. Practical suggestions on intravenous iloprost in Raynaud’s phenomenon and digital ulcer secondary to systemic sclerosis: Systematic literature review and expert consensus. Semin Arthritis Rheum. 2019;48(4):686-693. doi:10.1016/j.semarthrit.2018.03.019
- Badesch DB, McLaughlin VV, Delcroix M, et al. Prostanoid therapy for pulmonary arterial hypertension. J Am Coll Cardiol. 2004;43(12 Suppl S):56S-61S. doi:10.1016/j.jacc.2004.02.036
- Khanna D, Tashkin DP, Denton CP, Renzoni EA, Desai SR, Varga J. Etiology, Risk Factors, and Biomarkers in Systemic Sclerosis with Interstitial Lung Disease. American Journal of Respiratory and Critical Care Medicine. 2020;201(6):650-660. doi:https://doi.org/10.1164/rccm.201903-0563CI
- Cottin V, Brown KK. Interstitial lung disease associated with systemic sclerosis (SSc-ILD). Respiratory Research. 2019;20(1). doi:https://doi.org/10.1186/s12931-019-0980-7
- Esposito AJ, Selvan KC, Richardson C, et al. Systemic Sclerosis-Associated Interstitial Lung Disease: What We Know and How to Incorporate Guidelines into Clinical Practice. Chest. Published online Spring 2025:S0012-3692(25)058428. doi:https://doi.org/10.1016/j.chest.2025.11.047
- Raghu G, Montesi SB, Silver RM, et al. Treatment of Systemic Sclerosis-associated Interstitial Lung Disease: Evidence-based Recommendations. An Official American Thoracic Society Clinical Practice Guideline. Am J Respir Crit Care Med. 2024;209(2):137-152. doi:10.1164/rccm.202306-1113ST
- Perelas A, Silver RM, Arrossi AV, Highland KB. Systemic sclerosis-associated interstitial lung disease. The Lancet Respiratory Medicine. 2020;8(3):304-320. doi:https://doi.org/10.1016/S2213-2600(19)30480-1
- Chung JH, Walker CM, Hobbs S. Imaging Features of Systemic Sclerosis-Associated Interstitial Lung Disease. J Vis Exp. 2020;(160):10.3791/60300. Published 2020 Jun 16. doi:10.3791/60300
- Johannson KA, Chaudhuri N, Adegunsoye A, Wolters PJ. Treatment of fibrotic interstitial lung disease: current approaches and future directions. Lancet. 2021;398(10309):1450-1460. doi:10.1016/S0140-6736(21)01826-2
- Johnson SR, Bernstein EJ, Bolster MB, et al. 2023 American College of Rheumatology (ACR)/American College of Chest Physicians (CHEST) Guideline for the Treatment of Interstitial Lung Disease in People with Systemic Autoimmune Rheumatic Diseases. Arthritis Care & Research. Published online July 8, 2024.
- Dhanani Z, Gupta R. The Management of Interstitial Lung Disease in the ICU: A Comprehensive Review. J Clin Med. 2024;13(22):6657. Published 2024 Nov 6. doi:10.3390/jcm13226657
- Jiang Y, Turk MA, Pope JE. Factors associated with pulmonary arterial hypertension (PAH) in systemic sclerosis (SSc). Autoimmun Rev. 2020;19(9):102602. doi:10.1016/j.autrev.2020.102602
- Denton CP, Hachulla E. Risk factors associated with pulmonary arterial hypertension in patients with systemic sclerosis and implications for screening. Eur Respir Rev. 2011;20(122):270-276. doi:10.1183/09059180.00006111
- Dweik RA, Rounds S, Erzurum SC, et al. An official American Thoracic Society Statement: pulmonary hypertension phenotypes. Am J Respir Crit Care Med. 2014;189(3):345-355. doi:10.1164/rccm.201311-1954ST
- Morrisroe K, Huq M, Stevens W, et al. Risk factors for development of pulmonary arterial hypertension in Australian systemic sclerosis patients: results from a large multicenter cohort study. BMC Pulm Med. 2016;16(1):134. Published 2016 Sep 27. doi:10.1186/s12890-016-0296-z
- Hassoun PM. Pulmonary Arterial Hypertension. Taichman DB, ed. New England Journal of Medicine. 2021;385(25):2361-2376. doi:https://doi.org/10.1056/nejmra2000348
- Sirajuddin A, Mirmomen SM, Henry TS, et al. ACR Appropriateness Criteria® Suspected Pulmonary Hypertension: 2022 Update. Journal of the American College of Radiology. 2022;19(11):S502-S512. doi:https://doi.org/10.1016/j.jacr.2022.09.018
- Pulmonary hypertension – WikEM. Wikem.org. Published 2026. Accessed January 27, 2026. https://wikem.org/wiki/Pulmonary_hypertension
- Misch M. Pulmonary Hypertension | CritCases | EM Cases. Emergency Medicine Cases. Published March 28, 2017. https://emergencymedicinecases.com/pulmonary-hypertension/
- in. NUEM Blog. NUEM Blog. Published August 13, 2018. https://www.nuemblog.com/blog/pulmonary-hypertension-ed
- Ashkar H, Adnan G, Patel P, et al. Dobutamine. [Updated 2024 Feb 23]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK470431/
- Ayres JK, Maani CV. Milrinone. [Updated 2023 Aug 28]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK532943/
- Savale L, Kularatne M, Roche A, et al. Management of Acutely Decompensated Pulmonary Hypertension. Semin Respir Crit Care Med. 2023;44(6):762-770. doi:10.1055/s-0043-1770119
- Brandler JB, Sweetser S, Khoshbin K, Babameto M, Prokop LJ, Camilleri M. Colonic Manifestations and Complications Are Relatively Under-Reported in Systemic Sclerosis: A Systematic Review. Am J Gastroenterol. 2019;114(12):1847-1856. doi:10.14309/ajg.0000000000000397
- Mecoli C, Purohit S, Sandorfi N, Derk CT. Mortality, recurrence, and hospital course of patients with systemic sclerosis-related acute intestinal pseudo-obstruction. J Rheumatol. 2014;41(10):2049-2054. doi:10.3899/jrheum.131547
- den Braber-Ymker M, Vonk MC, Grünberg K, Lammens M, Nagtegaal ID. Intestinal hypomotility in systemic sclerosis: a histological study into the sequence of events. Clin Rheumatol. 2021;40(3):981-990. doi:10.1007/s10067-020-05325-8
- Strother AK, Anderton RM, Kalavar N, et al. Gastrointestinal histology of systemic sclerosis: A systematic review. Autoimmun Rev. Published online January 22, 2026. doi:10.1016/j.autrev.2026.103988
- Basilisco G, Marchi M, Coletta M. Chronic intestinal pseudo-obstruction in adults: A practical guide to identify patient subgroups that are suitable for more specific treatments. Neurogastroenterol Motil. 2024;36(1):e14715. doi:10.1111/nmo.14715
- Quigley EMM, Murray JA, Pimentel M. AGA Clinical Practice Update on Small Intestinal Bacterial Overgrowth: Expert Review. Gastroenterology. 2020;159(4):1526-1532. doi:https://doi.org/10.1053/j.gastro.2020.06.090
- Camilleri M, Kuo B, Nguyen L, et al. ACG Clinical Guideline: Gastroparesis. Am J Gastroenterol. 2022;117(8):1197-1220. doi:10.14309/ajg.0000000000001874
- Verne GN, Eaker EY, Hardy E, Sninsky CA. Effect of octreotide and erythromycin on idiopathic and scleroderma-associated intestinal pseudoobstruction. Dig Dis Sci. 1995;40(9):1892-1901. doi:10.1007/BF02208652




