Today on the emDOCs cast with Brit Long, MD (@long_brit) and Rachel Bridwell, MD (@rebridwell), we cover the challenge of pulmonary hypertension.
Pulmonary Hypertension
Background:
– Pulmonary hypertension (PH) is characterized by increased pulmonary vascular resistance and pulmonary arterial pressure. It affects 15-60 million individuals worldwide.
– PH is defined by a mean pulmonary arterial pressure of greater than 25 mm Hg by right heart catheterization or inferred by echocardiogram. The WHO classify PH into 5 groups:

Pulmonary Pathophysiology:
– The pulmonary circulation is normally a low-resistance, low-pressure system, composed of thin-walled vessels capable of accommodating vast alterations in preload.
– In patients with chronic PH, pulmonary vascular resistance gradually increases with vascular remodeling of the pulmonary arteries with vascular smooth muscle and endothelial cell proliferation, inflammation, and fibrosis.
– Beyond a specific point of RV distension, RV output decreases secondary to increased pulmonary pressure and impedance to RV outflow. This sets in motion a cascade of interventricular dependence in which bulging of the RV into the left ventricle (LV) decreases LV filling, subsequently decreasing cardiac output. As cardiac output falls, end organ perfusion suffers.

– In a normal physiologic setting, the coronary arteries of the RV are perfused in both systole and diastole due to low RV wall tension as compared to the LV. In PH, as RV pressures increase, RV perfusion falls until pulmonary artery pressures exceed systemic pressure, generating RV ischemia. RV contractility declines, worsening RV overload.
ED Evaluation:
– Dyspnea is the most common presenting complaint, though patients also report fatigue, weakness, chest pain, and syncope.
– Angina results from ischemic subendocardial injury from ventilation-perfusion mismatch or compression of the left main coronary artery by the pulmonary trunk.
– Syncope is also associated with a poor prognosis, while hoarseness may occur due to compression of the recurrent laryngeal nerve by an enlarged pulmonary artery.
– In advanced disease, individuals frequently present with symptoms of right heart failure (RHF): ascites, peripheral edema, and hemoptysis.
– Evaluate for underlying precipitants of RHF including sepsis, unplanned withdrawal of PH therapy, medication non-compliance, pregnancy, pneumonia, anemia, and arrhythmias.
History
– History should include PH risk factors including: congenital heart disease, left-sided heart disease, valvular disease, pulmonary disease, connective tissue disease, liver disease, blood dyscrasias, thyroid disorders, dialysis-dependent renal disease, malignancy, stimulant use, and family history of PH.
– If available, a prior echocardiogram should be reviewed for signs of PH. Medication compliance and prior complications should be assessed.
Physical Examination
– In advanced PH, signs of RHF are commonly present: elevated JVP, hepatojugular reflex, ascites, hepatomegaly, and peripheral edema. An increased pulmonic component of the second heart sound (P2), an RV gallop, or the murmur of tricuspid regurgitation may be present.
– Arrhythmias including atrial fibrillation, atrial flutter, and atrioventricular node re-entry tachycardias are common.
– Patients with decompensated PH frequently present with hypotension, displaying signs of systemic hypoperfusion including diaphoresis, cool extremities, peripheral cyanosis, and tachycardia.
Studies
– An ECG may show right axis deviation and right ventricular hypertrophy (Figure 2). In addition to a tachyarrhythmia, right atrial enlargement, and ST segment depression and T wave inversion in the precordial leads may show right heart strain.
Figure 2. ECG with evidence of pulmonary hypertension.

– In patients with chronic PH, venous blood gas frequently demonstrates hypoxemia and respiratory alkalosis.
– BNP, troponin, renal function panel, electrolytes, liver function panel, and lactate.
– Imaging includes chest radiograph and bedside echocardiography (Figure 3). Radiographic findings of PH include dilated pulmonary arteries, peripheral pruning, and an enlarged right atria and RV, while pleural effusions may reflect severe disease. Bedside echocardiography may show right atrial enlargement, RV dilation (RV: LV > 1:1; normal < 0.6), increased RV free wall thickness (> 5-7 mm as measured at end-diastole by M-mode or 2D echocardiography from the parasternal long axis or subxiphoid view), end-systolic flattening of the intraventricular septum, and interventricular interdependence visualized as a “D”-shaped left ventricle in diastole (Figure 3).
Figure 3. Ultrasound depicting RV dilatation.

– CT demonstrating right atrial enlargement, RV dilation main pulmonary/ascending aorta diameter ratio is suggestive of PH. On CT, the pulmonary trunk should be no larger than 2.8 cm at the level of its bifurcation. Measurements > 2.8 cm suggest PH with a sensitivity of 69%–87% and a specificity of 89%–100%. For individuals with CTEPH, CT angiography may reveal thrombi in the pulmonary vasculature and identify shunts contributing to the patient’s presentation.
Figure 4. CT of the chest demonstrating evidence of PH with a main pulmonary/ascending aorta diameter ratio ³ 1 and a pulmonary trunk of >2.8 cm.


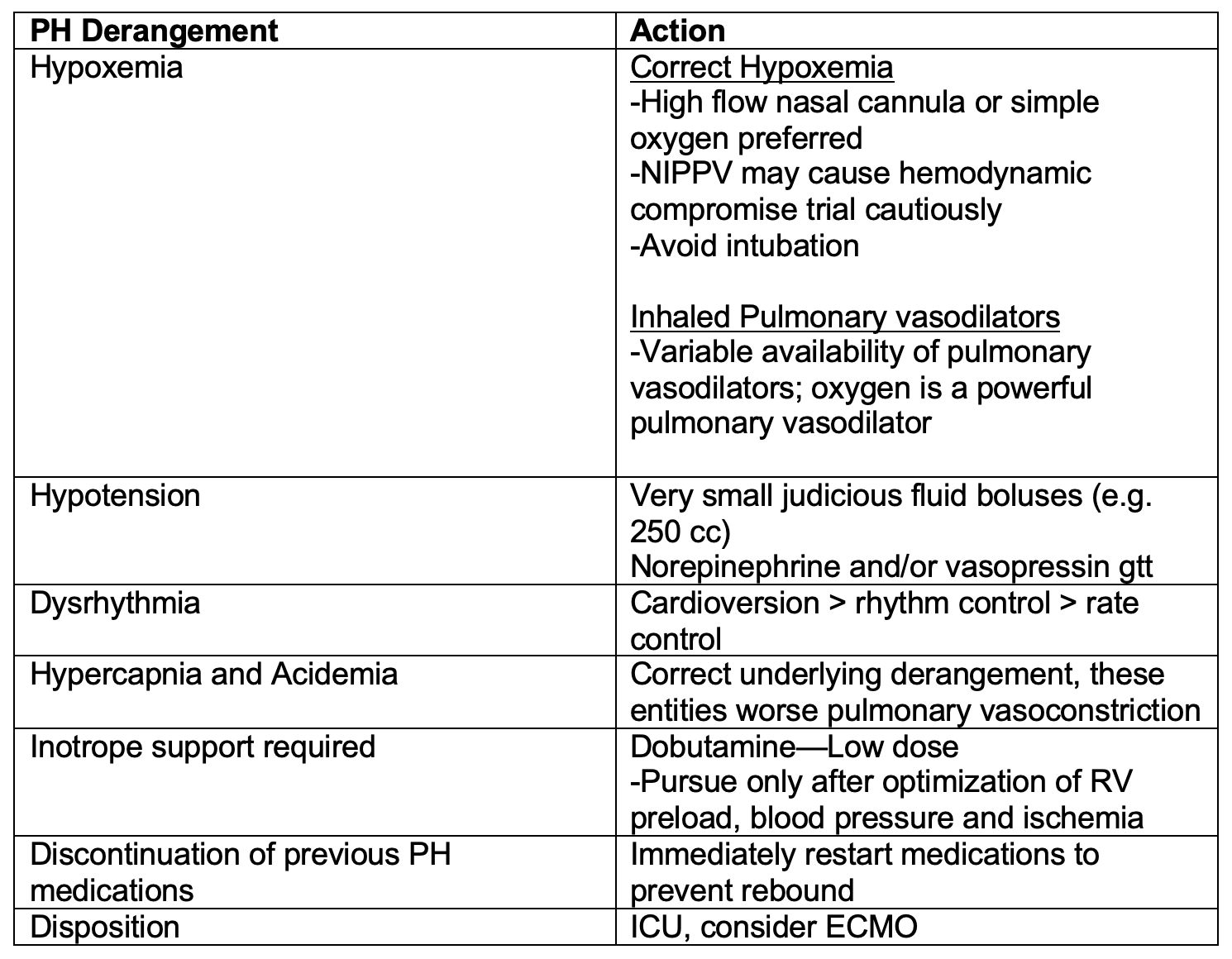
ED Management:

– Identify and treat the underlying etiologies of PH (e.g. alveolar hypoxia in COPD, hyperthyroidism, etc.). For individuals presenting with RHF, triggering factors should be addressed: antibiotic therapy administered for infections, transfusions given as indicated for anemia to maintain a hemoglobin of greater than 10 g/dL, and arrhythmias treated.
– New-onset atrial fibrillation or flutter is common in PH patients. Rhythm control is recommended, as rate control medications further impair RV function. Electrical cardioversion is favored as prolonged atrial arrhythmias in patients with PH are associated with rapid decompensation. In individuals with atrial arrhythmias lasting > 48 hours, anticoagulation is advised prior to cardioversion.
– In PH patients who present due to an unexpected discontinuation in oral or IV PH therapy, contact the patient’s PH specialist to initiate ED treatment and prevent acute decompensation. While prostacyclins, endothelin receptor agonists, and phosphodiesterase inhibitors may not be immediately available in the ED, initiating these therapies early in the ED course may help to stave off clinical instability, though optimizing oxygenation and circulation should take priority.
– In individuals with PH, supplemental oxygen is indicated to maintain an oxygen saturation > 90%. Hypercapnia should be avoided as it results in further pulmonary vasoconstriction. Continuous non-invasive positive pressure ventilation may be considered, though fluid balance must be optimized prior to initiation to eliminate dangerous decreases in cardiac output. High-flow nasal cannula (HFNC) is an alternative therapy that may improve hypoxemia, especially if patients are unable to tolerate the mask utilized for NIPPV.
– Intubation should be avoided if possible, as the effect of sedatives and positive intrathoracic pressure may reduce preload, cardiac function and cause peripheral vasodilation, resulting in hypotension and cardiovascular collapse. If intubation is required, etomidate is recommended for induction, given its limited effects on cardiac contractility and vascular tone. Hemodynamic optimization prior to intubation is recommended. If the patient is hemodynamically unstable, vasopressors should be initiated before attempts to establish a definitive airway are made.
– Awake intubation with topical anesthetics is an alternative that should be considered given the reduced risk of hemodynamic decompensation as compared to rapid sequence intubation. Medications administered during rapid sequence induction will likely result in profound hemodynamic collapse, hypercarbia, hypoxemia, and acidosis.
– Ventilator settings should target 6-8 mL/kg of ideal body weight and plateau pressures less than 30 cm H2O. Low positive end expiratory pressures should be utilized to minimize decreases in preload and increases in RV afterload.
– IV diuretics should be used cautiously to obtain a negative fluid balance, optimizing circulating blood volume and reducing RV preload, and thus improving cardiac output. For patients not previously receiving oral diuretics, an initial dose of 20 – 40 mg IV furosemide is recommended for hypervolemia. In individuals utilizing home diuretic therapy, the initial IV dose should be at least equivalent to the oral dose. In hypovolemic patients, volume should be delivered conservatively, with boluses of 250 mL over 15-30 minutes.
– Vasopressors should be initiated for hemodynamically unstable patients. Norepinephrine is an effective first-line vasopressor for patients with PH. The addition of low dose vasopressin (0.01-0.03 U/min) may be considered if the aforementioned therapies fail to result in hemodynamic improvement. Epinephrine may benefit PH patients given the combined alpha and beta stimulation which provides system vascular support with inotropy, though this may increase myocardial oxygen demand. Dopamine should be also avoided given b2-mediated decreases in systemic vascular resistance and possible arrhythmias.
– Inotropes increase the risk of tachyarrhythmias and should only be utilized in the setting of inadequate oxygen delivery, despite correction of abnormalities in RV preload and conditions causing RV ischemia. If inotrope support is required, dobutamine is the agent of choice. Milrinone, a selective PDE-3 inhibitor, is recommended for PH resulting from biventricular failure (0.375-0.75 mg/kg/min IV).
– Patients who fail to respond to inotrope and vasopressor therapy should be considered for venoarterial extracorporeal membrane oxygenation. Patients with PH have a high risk of sudden cardiac death and poor outcomes.
Special Population – Prostacyclin Agonist Pump
– A life-threatening emergency can occur if the patient has been prescribed IV epoprostenol or treprostinil and the IV catheter is removed or damaged, or the pump stops working. If possible, the pump should not be turned off as this may result in sudden death. If there is a problem with the line, pump, or cassette, peripheral access should be obtained and the pump tubing connected directly to this access.
– The line should not be primed or flushed, as a bolus of prostacyclin agonist may be delivered to the patient, resulting in fatal hypotension.
Inhaled Therapies
– With low systemic absorption, inhaled vasodilators, e.g. nitric oxide and epoprostenol, decrease pulmonary vascular resistance, improving cardiac output.
– These can be administered via endotracheal tube, NIPPV or HFNC, though depend on local hospital policy whether a closed circuit is required.
Pulmonary Hypertension Crisis Management
– Patients with PH may present unstable from an acute illness (e.g. sepsis) or become unstable after an intervention (e.g. intubation).
Disposition:
– If new onset PH, worsening or decompensated PH, or pump malfunction with prostacyclin agonist contribute to the ED presentation, admission and consultation with the specialty team are warranted.
Key Points:
-Myriad of chief complaints can be pulmonary hypertension; try to determine what is triggering the acute decompensation.
–Elevations in troponin and liver function tests portend a poor prognosis.
–Point of care ultrasound may be useful in guiding acute resuscitation, though evaluation of IVC may not reflect intravascular volume.
–Avoid hypoxemia and hypercarbia and maintain right ventricular preload support.
-Most patients will be admitted.
–Avoid intubating these patients if at all possible.
–Restart PAH meds if discontinued.




