Welcome to the emDOCs Videocast – please subscribe to our YouTube channel. These videos will cover post summaries, take homes on clinical condition, and EBM/guideline literature updates. Today we focus on Andexanet versus 4F-PCC for reversal of DOAC-associated intracerebral hemorrhage (ICH).
EBM Update: ANNEXA-1 and DOAC Reversal in ICH
Article:
- Connolly SJ, Sharma M, Cohen AT, et al; ANNEXA-I Investigators. Andexanet for Factor Xa Inhibitor-Associated Acute Intracerebral Hemorrhage. N Engl J Med. 2024 May 16;390(19):1745-1755. doi: 10.1056/NEJMoa2313040.
Clinical Question:
- In adult patients on a DOAC with ICH, does the use of Andexanet compared to usual care improve hemostatic efficacy?
Design and Inclusion:
- Non-blinded, randomized trial conducted at 131 centers in 23 countries over 4 years.
- Included adult patients (> 18 years) with ICH with 6 hours on DOAC (medication taken within 15 hours).
Exclusion:
- GCS < 7, NIHSS > 35, surgery planned within 12 hours, thrombotic event within 2 weeks, time from symptom onset > 6 hours, pregnancy
Intervention:
- Andexanet alfa high-dose or low-dose bolus followed by infusion depending on DOAC dose and time from last use
- Comparison: Usual care
Outcomes:
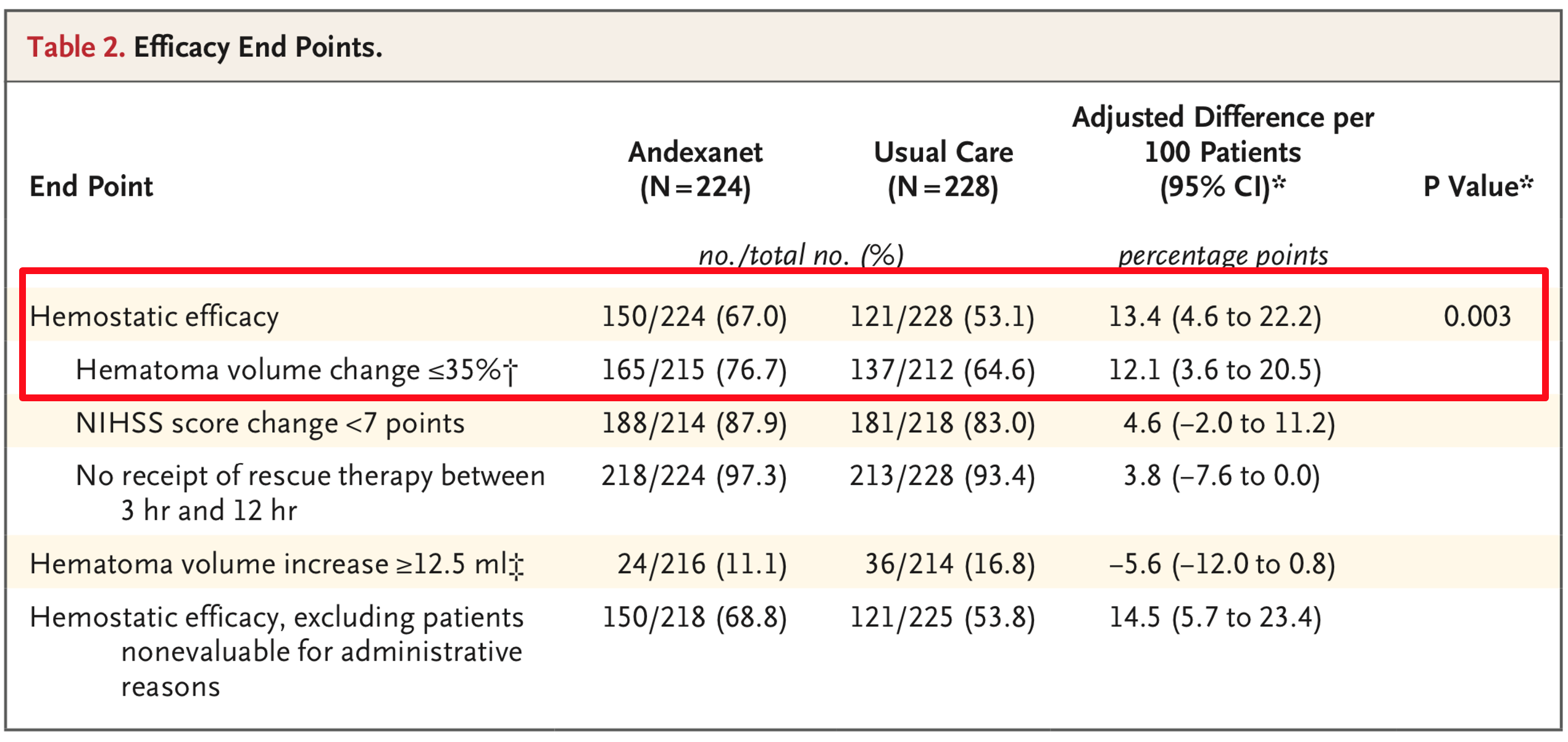
- Primary: Hemostatic efficacy at 12 hours after randomization, defined as:
- Excellent hemostatic efficacy: Change in hematoma volume <20%
- Good hemostatic efficacy: Change in hematoma volume <35%
- Increase in NIHSS < 7 points at 12 hours
- No receipt of rescue therapies within 3-12 hours from randomization
- No surgery to decompress the hematoma within 3-12 hours from randomization.
- Secondary: % change from baseline in anti-factor Xa activity during the first 2 hours from randomization
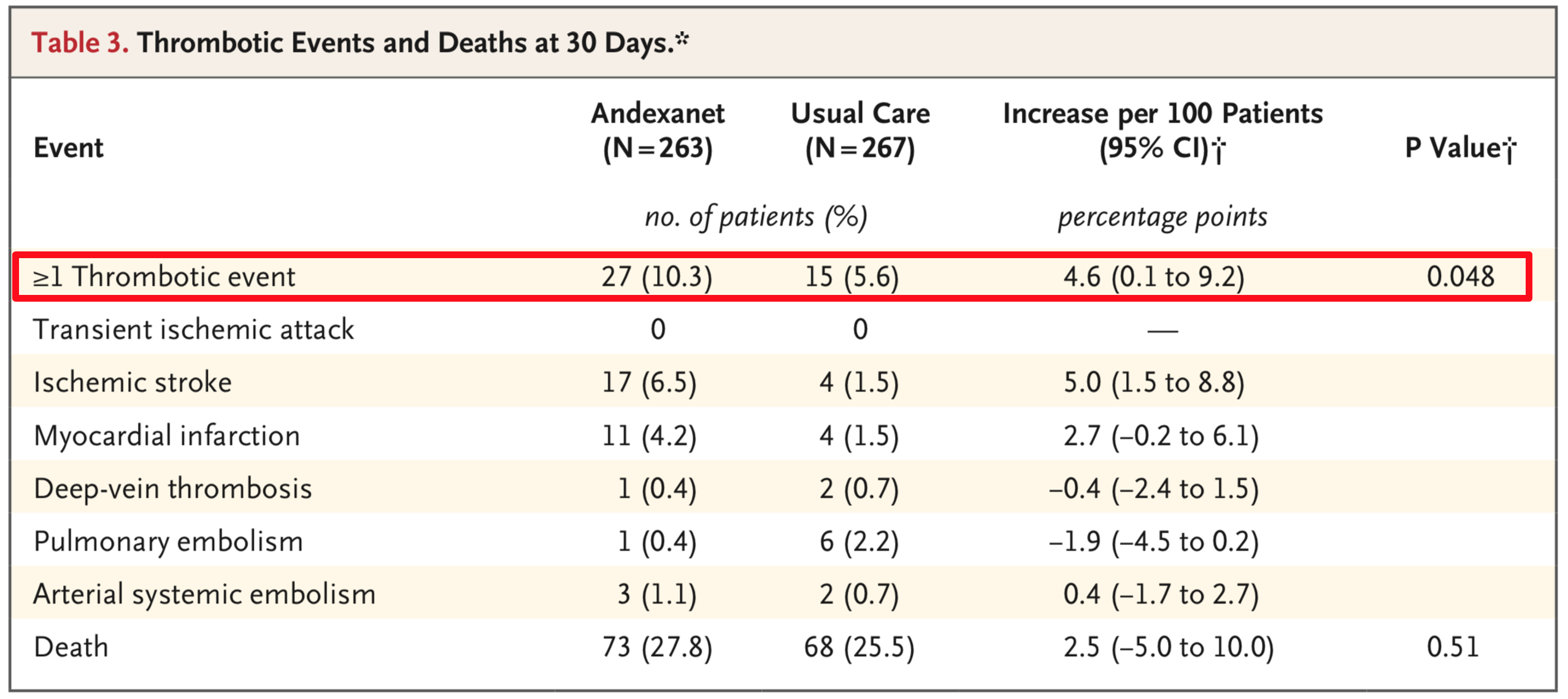
- Safety (assessed at 30 days): thrombotic events (ischemic stroke, VTE, myocardial infarction), mortality
Results:
- 452 patients analyzed for the primary outcome.
- 5% (195/228) patients in the usual care arm received 4F-PCC.
- 1% (175/224) patients in the Andexanet arm received the low-dose regimen.
- 530 patients analyzed for safety outcome.
- Hemostatic efficacy achieved in 150 of 224 patients (67.0%) receiving andexanet and in 121 of 228 (53.1%) receiving usual care (adjusted difference, 13.4 percentage points; 95% CI 4.6 to 22.2).
- Median reduction from baseline to the 1-to-2-hour nadir in anti–factor Xa activity was 94.5% with andexanet and 26.9% with usual care.
Considerations:
- 1st RCT evaluating Andexanet alpha for DOAC reversal in ICH.
- Multicenter, multinational study, which increases generalizability.
- Blinded outcome assessors.
- Study funded by Astra Zeneca (makers of Andexanet).
- Clinicians not blinded to randomization.
- Convenience sample of patients; baseline differences between groups present.
- Excluded sickest patients.
- Primary outcome is not patient-oriented but rather disease-oriented. There were no signals of improved clinical outcomes in patients receiving Andexanet.
- Safety outcomes favored the usual care group. Increased thrombotic events with Andexanet alpha.
- 5% of patients in the usual care group received 4F-PCC. They do not report on the other patient subset.
- Multiple protocol changes present, and the study was powered for 450 but they stopped at 450 patients. Both of these can result in bias and steer data towards a benefit when none exists.
Conclusion:
- In patients with ICH on a DOAC, this RCT suggests that Andexanet may result in better control of hematoma expansion than usual care but is associated with thrombotic events.
- Hospital policy is essential for DOAC reversal in the setting of a bleed.
Literature Update:
Orso D, Fonda F, Brussa A, Comisso I, Auci E, Sartori M, Bove T. Andexanet alpha versus four-factor prothrombin complex concentrate in DOACs anticoagulation reversal: an updated systematic review and meta-analysis. Crit Care. 2024 Jul 5;28(1):221. doi: 10.1186/s13054-024-05014-x.
Design:
- Systematic review and meta-analysis of studies comparing Andexanet alpha versus 4F-PCC for anticoagulation reversal.
- Registered on PROSPERO.
Outcome:
- Primary outcome: determine which drug is more effective in reducing short-term all-cause mortality.
- Secondary outcome: determine which of the two reverting strategies is less affected by thromboembolic events.
Results:
- Evaluated 22 studies (1 RCT – ANNEXA 1).
- No difference in short-term mortality: Andexanet alpha vs. 4F-PCC RR 0.71(95% CI 0.37–1.34) in RCTs and PSMs. Retrospective studies pooled RR 0.84 (95% CI 0.69–1.01) for the common effects model and 0.82 (95% CI 0.63–1.07) for the random effects model (I2 = 34.2%).
- Higher thromboembolic events in controlled studies with Andexanet: common and the random effects model RR 1.74 (95% CI 1.09–2.77) and 1.71 (95% CI 1.01–2.89), respectively, for Andexanet alpha versus 4F-PCC.
Guideline:
Recommendations:
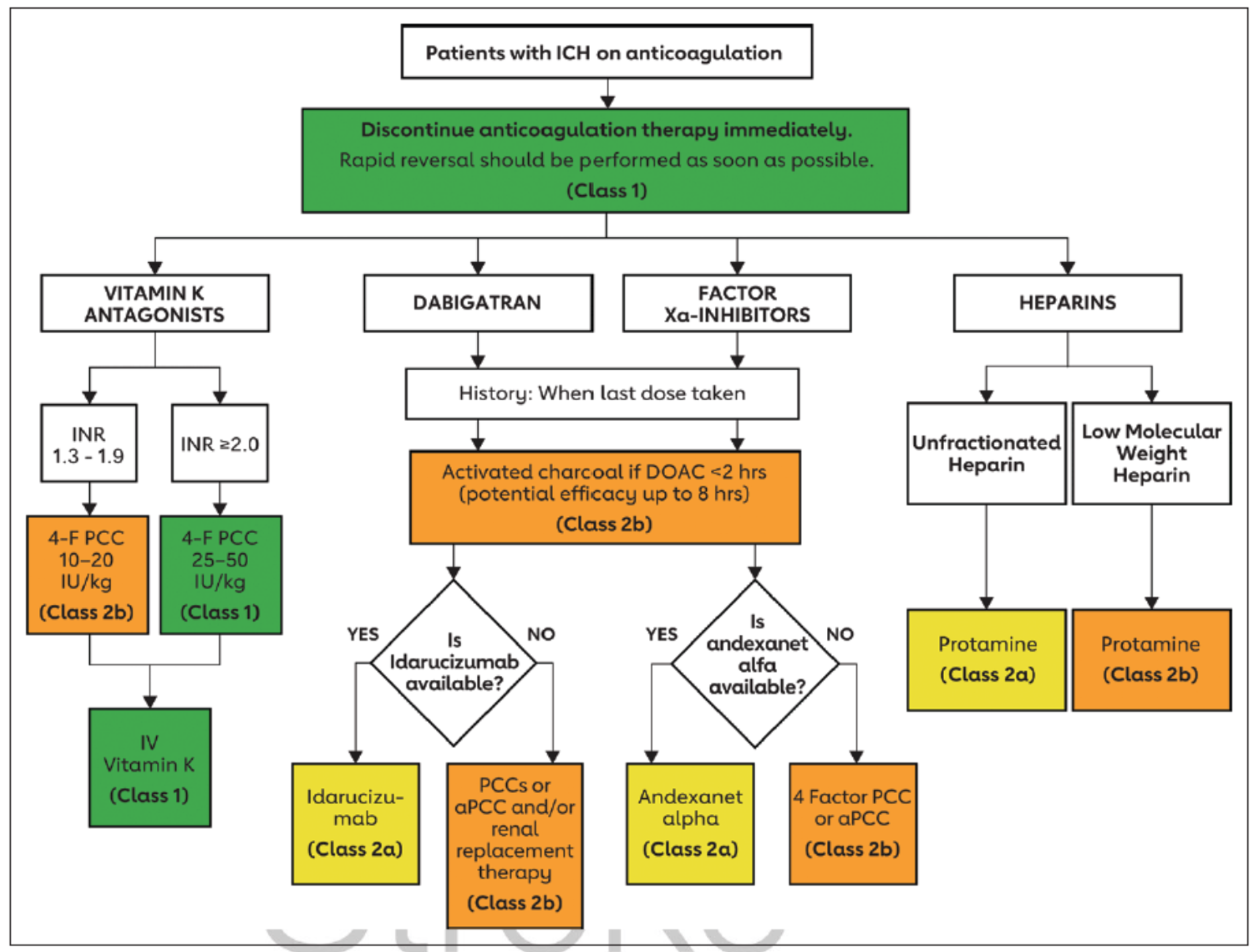
- In patients with direct factor Xa inhibitor–associated spontaneous ICH, andexanet alpha is reasonable to reverse the anticoagulant effect of factor Xa inhibitors. COR 2a, LOE B-NR.
- In patients with dabigatran-associated spontaneous ICH, idarucizumab is reasonable to reverse the anticoagulant effect of dabigatran. COR 2a, LOE B-NR.
- In patients with direct factor Xa inhibitor–associated spontaneous ICH, a 4-F PCC or activated PCC (aPCC) may be considered to improve hemostasis. COR 2b, LOE B-NR.
- In patients with dabigatran- or factor Xa inhibitor–associated spontaneous ICH, when the DOAC agent was taken within the previous few hours, activated charcoal may be reasonable to prevent absorption of the DOAC. COR 2b, LOE C-LD.
- In patients with dabigatran-associated spontaneous ICH, when idarucizumab is not available, aPCC or PCCs may be considered to improve hemostasis. COR 2b, LOE C-LD.
- In patients with dabigatran-associated spontaneous ICH, when idarucizumab is not available, renal replacement therapy (RRT) may be considered to reduce dabigatran concentration. COR 2b, LOE C-LD.
- Editorial Comment: There is limited evidence supporting improved patient-centered outcomes with andexanet alpha. 4-F PCC and aPCC are effective reversal agents, with more literature support compared to andexanet alpha for DOAC reversal. An institutional protocol utilizing PCC is recommended.
Content reviewed by Manny Singh and Alex Koyfman. Assistance with video provided by Kyle Smiley.




