Author: Brit Long, MD (@long_brit, EM attending physician, San Antonio, TX) // Edited by: Alex Koyfman, MD (@EMHighAK)
Case
A 58-year-old female presents with fever. She has a history breast cancer and is receiving docetaxel for therapy. She has no other symptoms besides fatigue. Her vital signs include oral temperature 38.2o Celsius, heart rate 72, blood pressure 118/71 mm Hg, respiratory rate 16 breaths/minute, and saturation 99% on room air. On examination, she is well-appearing. No focal signs of infection are present, and she appears well-hydrated. Her chest x-ray and urinalysis are normal. However, her CBC reveals an absolute neutrophil count (ANC) of 435/microL. After acetaminophen and some IV antibiotics, you call her oncologist. He feels she is appropriate for discharge home. Wait… what? Can you discharge patients with neutropenic fever? How do you risk stratify these patients? This post evaluates neutropenic fever risk stratification and disposition.
Background
Cancer is a major cause of morbidity and mortality in the U.S.1-5 As life expectancy increases, the number of patients living with cancer will rise. With this comes increased chance of complications. One of these is neutropenic fever.
Neutropenic fever is an oncologic emergency, with over 100,000 cases per year.1-3 It is defined by a single oral temperature > 38.3o C or temperature > 38.0o C for 1 hour with neutropenia.6-8
Neutropenia is defined by an absolute neutrophil count (ANC) < 1500 cells/microL: mild (ANC 1000-1500 cells/microL), moderate (500-1000 cells/microL), severe (< 500 cells/microL), and profound (< 100 cells/microL).6-8 While 20-30% of cases of neutropenic fever are due to bacterial infection, neutropenic fever should be assumed to be due to microbial infection.9-13 The most common bacterial sources include gram-positive and gram-negative species.12-17
Patients can present with a range of symptoms, from well-appearing to hemodynamically unstable requiring emergent resuscitation. Those with hemodynamic shock and neutropenic fever experience a mortality rate approaching 50%.8-12 However, many patients will just present with fever.6-8
You know what to do for neutropenic fever: evaluate for the source, obtain blood cultures, resuscitate if needed, and provide broad-spectrum antibiotics. We will not cover the ED assessment and management of neutropenic fever in this post. Instead, we will focus on risk scores and disposition. Before we get to these topics, consultation with the patient’s oncologist is recommended. Clinical judgment should always overrule a clinical risk score.
Does every patient require admission to the hospital?
A significant number of patients with neutropenic fever are admitted. If the patient appears toxic, requires significant resuscitation, and has other major comorbidities, the decision is easy… admit. What about the patient who is otherwise well-appearing? In this situation, hospital admission can potentially expose the patient to harm with more procedures and exposure to other dangerous microbes. Patients who are low risk may be either admitted with IV antibiotics followed by transition to oral outpatient therapy, or discharged from the ED with oral antibiotics.
Is outpatient therapy safe in low-risk patients with neutropenic fever?
Several studies have evaluated the safety of outpatient therapy, with meta-analyses suggesting outpatient therapy is comparable to inpatient admission in terms of mortality and treatment failure. A meta-analysis by Teuffel et al. found no difference, and a 2019 Cochrane review included 10 randomized controlled trials (RCTs), with 628 adults and 366 pediatric patients.18,19 Authors found no difference in treatment failure in adults or pediatric patients (RR 1.23, 95% CI 0.82-1.85, and RR 1.04, 95% CI 0.55-1.99, respectively) and mortality in adult and pediatric patients (RR 1.04, 95% CI 0.29-3.71, and RR 0.63, 95% CI 0.15-2.70, respectively).19 This Cochrane review found no clear difference in secondary outcomes including duration of neutropenia or fever.19
How do you risk stratify patients with neutropenic fever?
There are a significant number of risk scores available, such as The Multinational Association for Supportive Care in Cancer (MASCC) score and the Clinical Index of Stable Febrile Neutropenia (CISNE) score, which are likely the two best-known scoring systems.20-28 However, outpatient therapy is also supported by society guidelines, including the IDSA, American Society of Clinical Oncology (ASCO), and National Comprehensive Cancer Network (NCCN).6-8
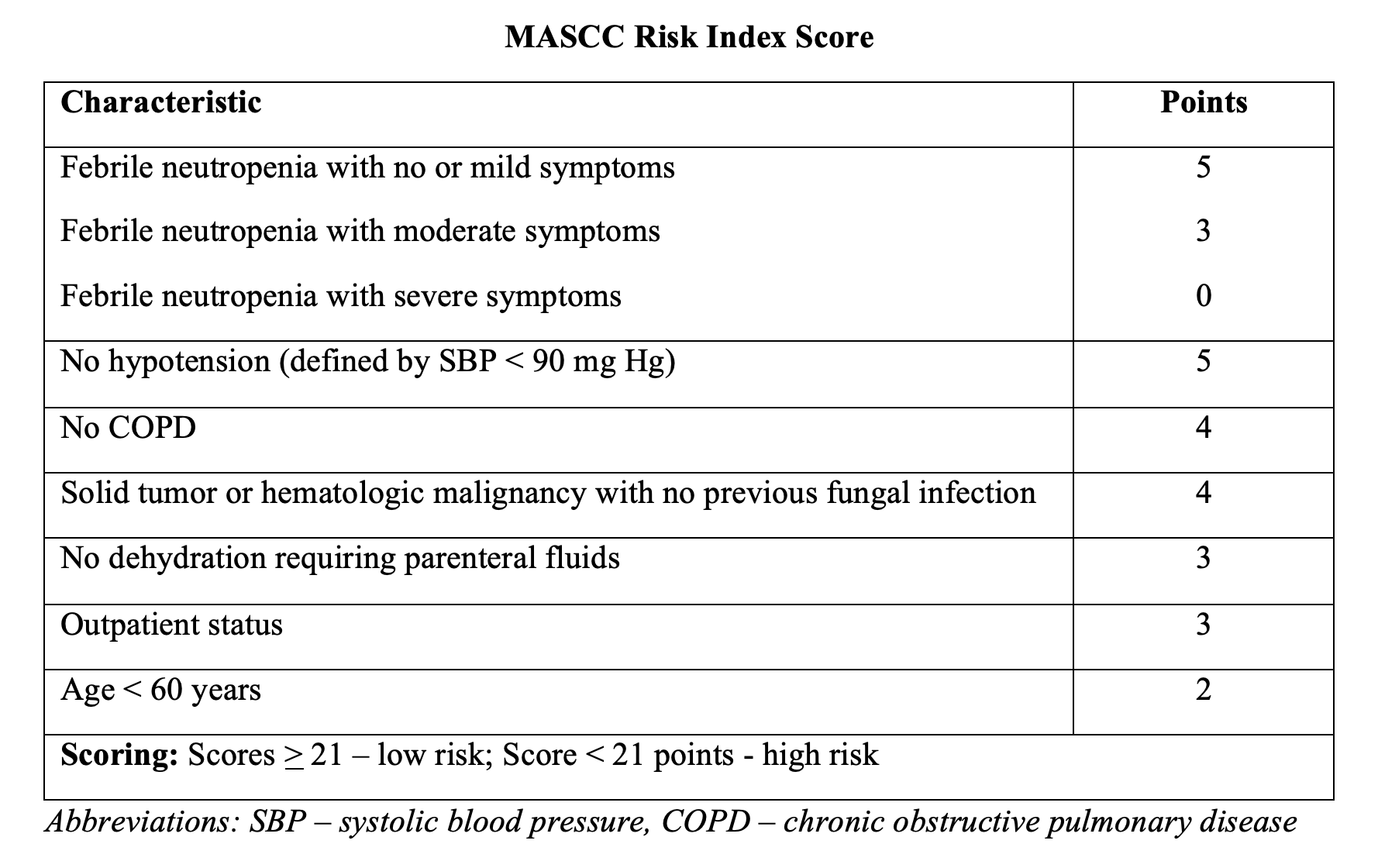
Perhaps the best-known score is the MASCC tool, which is a validated tool from ambulatory patients in the hematology-oncology setting.20-24 Patient symptoms, hemodynamics, history of COPD, fungal infection, dehydration, prior outpatient status, and age make up this score, with a score >21 considered low risk.20-24 Scores over this level have a sensitivity and specificity for identifying those at low risk of 71% and 68%, respectively.6-8,20-24 This score has also been used in several different patient populations, though its sensitivity and specificity have been called into question, specifically regarding its ability to predict major complications in neutropenic patients. One study states that up to 16% of patients categorized as low risk by the MASCC score experienced adverse events.25 The IDSA and ASCO guidelines support the use of MASCC, stating those with high scores may be appropriate for discharge home.6-8
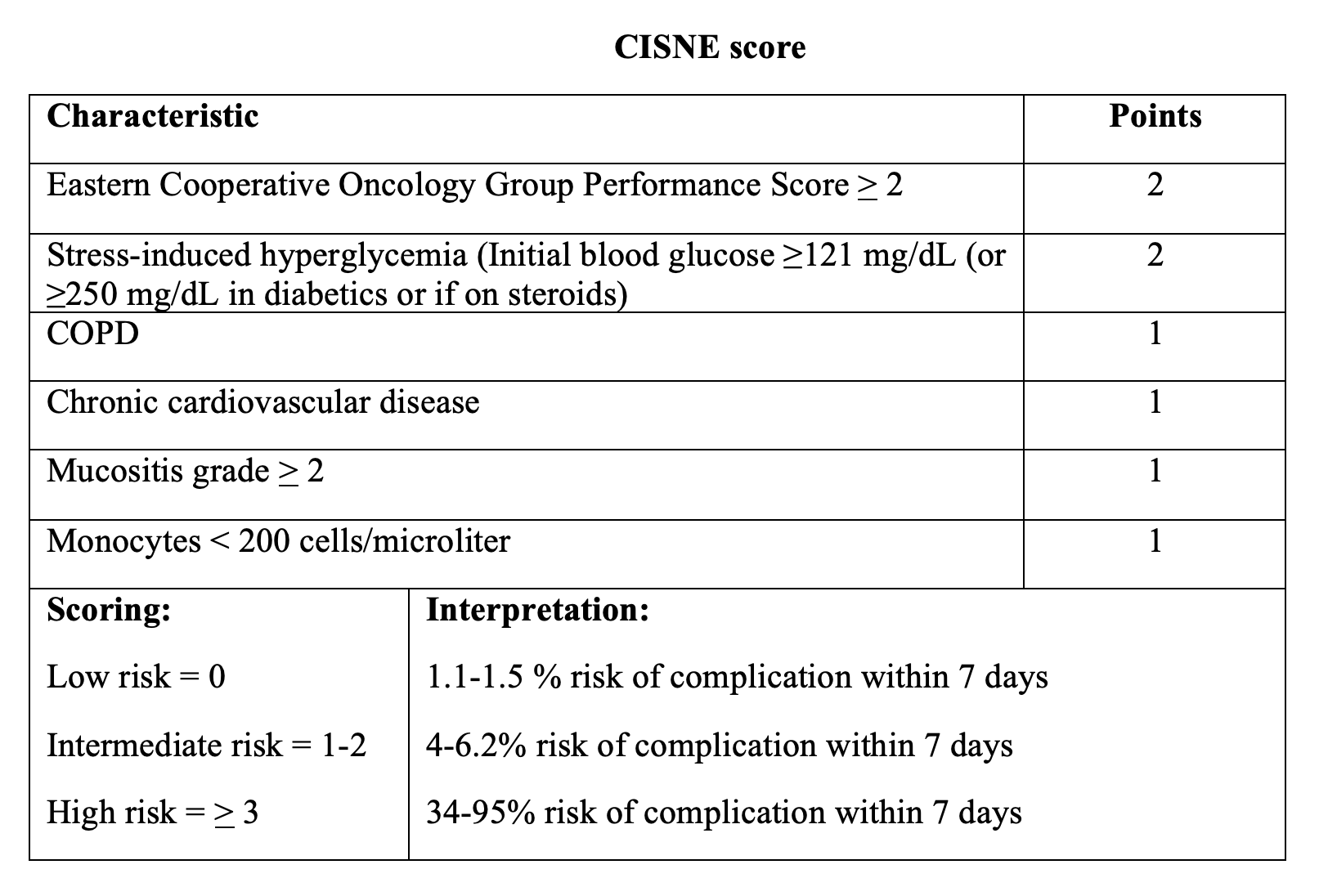
Another well-known score is CISNE score, which is relatively newer than the MASCC score. It was validated in the outpatient setting for patients with solid tumors and uses more historical factors compared to the MASCC score, as well as mucositis.25-28 This score incorporates COPD, hyperglycemia, cardiovascular disease, mucositis, and the Eastern Cooperative Oncology Group functional performance score. Scores above 0 points are associated with greater risk of adverse events or complications, defined as an episode of hypotension, cardiorespiratory failure, dysrhythmia, renal injury, delirium, DIC, acute abdomen, and major bleeding. Patients with a score of 0 are at low risk with a 1.1-1.5% risk of adverse event with 7 days.25-28 Those with scores of 3 or greater have much higher risk of complications. Specificity in identifying those patients at low risk is much higher for the CISNE score compared to the MASCC score, with one study suggesting a specificity of 98%.25
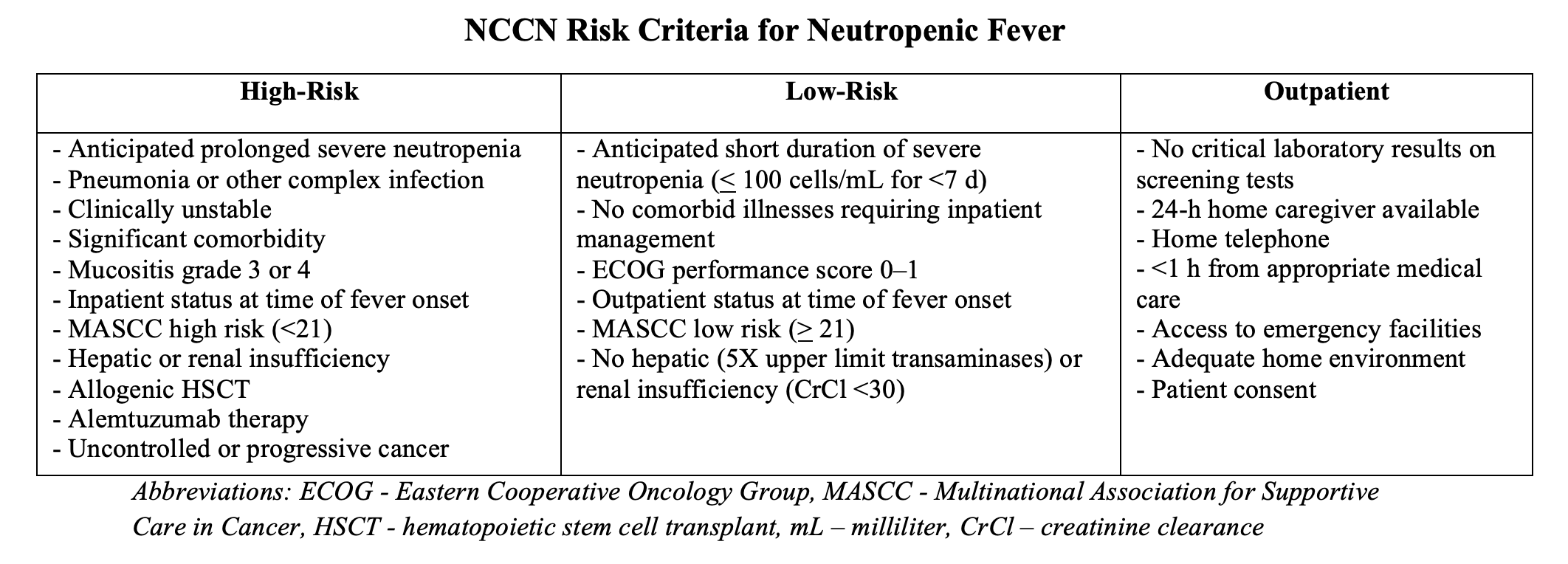
The IDSA and ASCO recognize the CISNE and MASCC scores.6-8 However, the IDSA and National Comprehensive Cancer Network have their own low risk versus high risk criteria.6-8 For patients to be appropriate for outpatient therapy with the IDSA criteria, they must meet low-risk and no high-risk criteria. Regarding the NCCN criteria, patients are appropriate for outpatient management if they meet none of the high risk criteria and all of the outpatient criteria.7 Patients at risk of failing outpatient therapy include those with mucositis, profound neutropenia (< 100 cells/microL), older than 70 years, and poor performance status.6-8

When it comes to MASCC vs. CISNE, the CISNE score appears to have lower risk of bias in study design and is more specific and reliable.25 However, there are several caveats. The CISNE score has been validated in patients with solid tumors, and thus this score needs further validation for patients with liquid tumors/hematologic malignancies before routine use.
While these scores can assist, the patient must be hemodynamically stable and well appearing. A discussion with oncology is also required, with follow up ensured after discharge and appropriate social situations. Patients who are toxic or those on fluoroquinolones for prophylaxis should be admitted. If the causative organism is suspected to be resistant, admission is recommended.6-8
Before discharge, ensure blood cultures are obtained, provide an intravenous dose of antibiotics, and observe the patient for 4 hours. If the patient worsens during this period, admission is recommended. While this is based on little data, it is a guideline recommendation per ASCO and the IDSA.6-8
What antibiotics are recommended for outpatient therapy?
An oral fluoroquinolone (ciprofloxacin or levofloxacin) plus amoxicillin/clavulanate is recommended. For those with a penicillin allergy, use clindamycin in place of the amoxicillin/clavulanate.6,8 If the fever continues after 2-3 despite outpatient oral antibiotic therapy, if new signs of symptoms develop, if blood cultures return as positive, or if the patient is unable to tolerate oral intake, admission is recommended with repeat laboratory examination.6,8
Back to our case…
After IV antibiotics and acetaminophen, the patient feels well. Her glucose is normal, and she has no COPD or cardiovascular disease, is not hypotensive, and has no mucositis. She is able to perform her activities of daily living and has follow-up with her oncologist. After observing her for 4 hours, you discharge her home with strict return precautions.
Key Points
- Fever with neutropenia is an emergency. Neutropenic fever is defined by the IDSA as oral temperature > 38.3o C or temperature >38.0o C for 1 hour with neutropenia.
- In patients who are risk stratified as low risk, outpatient therapy is safe when compared to inpatient therapy.
- Oncology consultation is recommended for patients with neutropenic fever, especially with the decision regarding discharge.
- While several risk scores can be used with oncology consultation, including the MASCC and CISNE scores, clinical judgment should overrule clinical scores.
- If the patient is appropriate for outpatient therapy following IV antibiotics and observation in the ED, an oral fluoroquinolone (ciprofloxacin or levofloxacin) plus amoxicillin/clavulanate is recommended.
References/Further Reading:
- Miller KD, Siegel RL, Lin CC, et al. Cancer treatment and survivorship statistics, 2016. CA Cancer J Clin 2016;66(4):271–89.
- Charshafian S, Liang SY. Rapid Fire: Infectious Disease Emergencies in Patients with Cancer. Emerg Med Clin N Am 2018;36:493-516.
- Cantwell L, Perkins J. Infectious Disease Emergencies in Oncology Patients. Emerg Med Clin N Am 2018;36:795–810.
- Kuderer NM, Dale DC, Crawford J, et al. Mortality, morbidity, and cost associated with febrile neutropenia in adult cancer patients. Cancer 2006;106(10):2258–66.
- Dulisse B, Li X, Gayle JA, et al. A retrospective study of the clinical and economic burden during hospitalizations among cancer patients with febrile neutropenia. J Med Econ 2013;16(6):720–35.
- Freifeld AG, Bow EJ, Sepkowitz KA, et al, Infectious Diseases Society of America. Clinical practice guideline for the use of antimicrobial agents in neutropenic patients with cancer: 2010 update by the Infectious Diseases Society of America. Clin Infect Dis 2011;52(4):e56–93.
- Baden LR, Swaminathan S, Angarone M, et al. Prevention and treatment of cancer-related infections, version 2.2016, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw 2016;14(7):882–913.
- Taplitz RA, Kennedy EB, Bow EJ, et al. Outpatient management of fever and neutropenia in adults treated for malignancy: American Society of Clinical Oncology and Infectious Diseases Society of America clinical practice guideline update. J Clin Oncol 2018. https://doi.org/10.1200/JCO.2017.77.6211.
- Melendez E, Harper MB. Risk of serious bacterial infection in isolated and unsuspected neutropenia. Acad Emerg Med. 2010;17(2):163-7.
- Wisplinghoff H, Seifert H, Wenzel RP, et al. Current trends in the epidemiology of nosocomial bloodstream infections in patients with hematological malignancies and solid neoplasms in hospitals in the United States. Clin Infect Dis. 2003;36(9):1103–10.
- Zinner SH. Changing epidemiology of infections in patients with neutropenia and cancer: emphasis on gram-positive and resistant bacteria. Clin Infect Dis. 1999;29(3):490-4.
- Ramphal R. Changes in the etiology of bacteremia in febrile neutropenic patients and the susceptibilities of the currently isolated pathogens. Clin Infect Dis. 2004;39(Suppl 1):S25-31.
- Oliveira AL, de Souza M, Carvalho-Dias VM, et al. Epidemiology of bacteremia and factors associated with multi-drug-resistant gram-negative bacteremia in hematopoietic stem cell transplant recipients. Bone Marrow Transplant. 2007 Jun;39(12):775-81.
- Portugal RD, Garnica M, Nucci M. Index to predict invasive mold infection in high-risk neutropenic patients based on the area over the neutrophil curve. J Clin Oncol 2009;27(23):3849–54.
- Yadegarynia D, Fatemi A, Mahdizadeh M, et al. Current spectrum of bacterial infections in patients with nosocomial fever and neutropenia. Caspian J Intern Med 2013;4(3):698–701.
- Mandal PK, Maji SK, Dolai TK, et al. Micro-organisms associated with febrile neutropenia in patients with haematological malignancies in a tertiary care hospital in eastern India. Indian J Hematol Blood Transfus 2015;31(1):46–50.
- Kanamaru A, Tatsumi Y. Microbiological data for patients with febrile neutropenia. Clin Infect Dis 2004;39(Suppl 1):S7–10.
- Teuffel O, Ethier MC, Alibhai SM, Beyene J, Sung L. Outpatient management of cancer patients with febrile neutropenia: a systematic review and meta-analysis. Annals of Oncology 2011;22(11):2358–65.
- Rivas-Ruiz R, Villasis-Keever M, Miranda-Novales G, Castelán-Martínez OD, Rivas-Contreras S. Outpatient treatment for people with cancer who develop a low-risk febrile neutropaenic event. Cochrane Database Syst Rev. March 2019. doi:10.1002/14651858.CD009031.pub2
- Klastersky J, Paesmans M, Rubenstein EB, et al. The Multinational Association for Supportive Care in Cancer risk index: a multinational scoring system for identifying low-risk febrile neutropenic cancer patients. J Clin Oncol 2000;18(16): 3038–51.
- Klastersky J, Paesmans M. The multinational association for supportive care in cancer (MASCC) risk index score: 10 years of use for identifying low-risk febrile neutropenic cancer patients. Support Care Cancer 2013;21(5):1487–95.
- Klastersky J, Paesmans M, Georgala A, et al. Outpatient oral antibiotics for febrile neutropenic cancer patients using a score predictive for complications. J Clin Oncol 2006;24(25):4129–34.
- Innes H, Lim SL, Hall A, et al. Management of febrile neutropenia in solid tumours and lymphomas using the Multinational Association for Supportive Care in Cancer (MASCC) risk index: feasibility and safety in routine clinical practice. Support Care Cancer 2008;16(5):485–91.
- Bitar RA. Utility of the Multinational Association for Supportive Care in Cancer (MASCC) risk index score as a criterion for nonadmission in febrile neutropenic patients with solid tumors. Perm J 2015;19(3):37–47.
- Coyne CJ, Le V, Brennan JJ, et al. Application of the MASCC and CISNE risk stratification scores to identify low-risk febrile neutropenic patients in the emergency department. Ann Emerg Med 2017;69(6):755–64.
- Carmona-Bayonas A, Gomez J, Gonzalez-Billalabeitia E, et al. Prognostic evaluation of febrile neutropenia in apparently stable adult cancer patients. Br J Cancer 2011;105(5):612–7.
- Carmona-Bayonas A, Jimenez-Fonseca P, Virizuela Echaburu J, et al. Prediction of serious complications in patients with seemingly stable febrile neutropenia: validation of the clinical index of stable febrile neutropenia in a prospective cohort of patients from the FINITE study. J Clin Oncol 2015;33(5):465–71.
- Cherif H, Johansson E, Bjorkholm M, et al. The feasibility of early hospital discharge with oral antimicrobial therapy in low risk patients with febrile neutropenia following chemotherapy for hematologic malignancies. Haematologica 2006; 91(2):215–22.





1 thought on “Emergency Oncology Updates: Can patients with neutropenic fever be discharged?”
It is important to clarify that CISNE is the sum of a score and eligibility criteria. It should only be used in patients with apparent clinical and haemodynamic stability, and without serious infections, as specified. Greetings.