Extracorporeal Membrane Oxygenation (ECMO) in the Emergency Department
By Brett Sweeney, MD
EM Chief Resident, New York Medical College/Metropolitan Hospital Center
Edited by Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UTSW / Parkland Memorial Hospital) and Stephen Alerhand, MD
Background
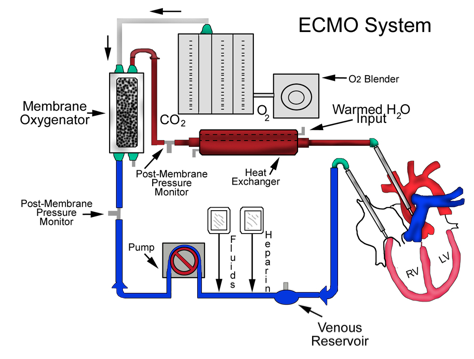
Extracorporeal membrane oxygenation (ECMO) is technology that has been used since the 1970s as a way of providing cardiac and respiratory support to patients who have potentially reversible causes of respiratory/cardiac failure. ECMO began in the neonate setting and quickly expanded to adult populations. (1) Today, EMCO is common practice in many ICU settings and is currently being used in select Emergency Departments across the U.S and internationally.
ECMO used in the emergent setting is more appropriately titled Extracorporeal Life Support (ECLS). Alternatively, ECMO used in the arresting patient has been termed Extracorporeal Cardiopulmonary Resuscitation (ECPR).
The focus of this article will be on the initiation of ECLS and ECPR in the Emergency Department setting.
The Basics
While there are two types of ECMO circuits, venous-arterial ECMO is the modality used for ECPR in the ED:
Venous-Arterial ECOM (VA ECMO)
• Goal: provide cardiovascular support during cardiac failure or shock.
• Indications:
o Bridge to therapy (PCI, transplant, LVAD)
o Refractory shock
o Cardiac Arrest
o Overdose
o Hypothermia w/ arrhythmias
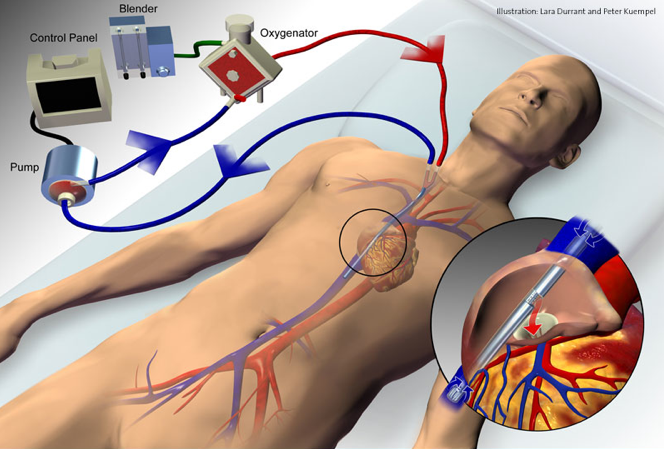
• Method: cannulation of the unilateral femoral vein and artery
Current Standard
Out of hospital cardiac arrest (OHCA)
• Traditional approach (ACLS w/ CPR) is highly unsuccessful
o Return of spontaneous circulation (ROSC) – 26.3% (2)
o Discharged from hospital – 9.6% (2)
• Associations with improved outcomes: (2-4)
o Rapid initiation of bystander CPR
o Rapid defibrillation
o Rapid PCI after ROSC
o Therapeutic hypothermia after ROSC
ECPR for OHCA
Currently there is mounting evidence that patients started on ECPR have better outcomes than those patients who receive traditional CPR for OHCA. While a RCT is lacking from the literature, some of the newer literature below in support of ECPR is used to answer relevant clinical questions.
Who are the candidates for ECPR?
This seems to be the most crucial part of a successful ECPR program for OHCA. While inclusion criteria differ among centers and studies, the general trend is outlined below. (6-11)
• Inclusion Criteria
o Witnessed arrest
o VF or VT as initial rhythm
o Age (18-70)
o Presumed cardiac cause
o Minimal interruptions in CPR
• Exclusion Criteria
o Irreversible causes
o Prolonged CPR/EMS transport
o Known cognitive impairment
o DNR/DNI
o Evidence of multi-organ dysfunction
How is ECPR initiated?
Traditionally, ECMO has been initiated by cardiothoracic surgeons in the OR. The advent of newer more mobile ECMO equipment has allowed ECMO implementation to be a common out-of-OR procedure. While most studies do not describe the exact method of ECMO implementation on OHCA patients, there is literature supporting the role of ED physicians in ED ECMO cannulation. (6,9)
Two US studies (6,9) have described the successful involvement of ED physicians in the initiation of ECPR. The best described ED ECPR algorithm is published by Drs. Shinar and Bellezzo who are strong advocates of ECPR and authors of the podcast/blog EDECMO.org. Below is their approach (completed by ED physician). (6)
Stage One:
• Traditional resuscitation efforts continue (ACLS with high quality CPR)
• ECLS Protocol is activated at discretion of the ED physician – ICU team alerted
• US-guided arterial and venous femoral angiocatheters are placed using commercially available kits.
Stage Two:
• Resuscitation continues
• Angiocatheters are replaced with guide wires – one at a time
• Using a commercially available kit, vessels are progressively dilated resulting in placement of large bore ECLS cannulas (17-21F venous and 15-19F arterial)
• ECLS system is primed by ED physician
Stage Three:
• Complete cardiopulmonary bypass is confirmed
• Adequate flow is achieved
• CPR is discontinued
What are the keys to successful outcomes?
The key to good outcomes is largely rooted in the inclusion criteria. Greater success has been demonstrated in the following situations: (7-13)
– Shorter time from arrest to ECLS initiation
– Cardiac cause with rapid catheterization
– ECLS combined with hypothermia protocols
– VT/VF as presenting rhythm
– Younger age at time of arrest
What types of outcomes are we seeing?
Le Guen M, et al. Extracorporeal life support following out-of-hospital refractory cardiac arrest. (2011)
• Single center prospective observational study
• Primary outcome – survival at 28 days after OHCA with ECLS
• 51 patients included in study
• 2 patients (4%) were alive at 28 days
Bellezzo JM. Emergency Physician-Initiated Extracorporeal Cardiopulmonary Resuscitation. (2012)
• Single center prospective observational study over 1 year (42 out of hospital cardiac arrests)
• Outcome – survival to hospital discharge neurologically intact
• 18 patients met inclusion criteria for ECMO
• 8 patients started on ECMO
• 5 patients survived to hospital discharge neurologically intact (12% of all OHCA)
SAVE-J Study Group. Extracorporeal cardiopulmonary resuscitation versus conventional cardiopulmonary resuscitation in adults with out-of-hospital cardiac arrest (2014)
• Multicenter (46) prospective observational study
• Goal – examine the neurological difference at 1 & 6 months in patients who had VF/VT arrest out of hospital – 2 groups: ECPR vs. conventional CPR
• 454 total patients (234 in ECPR group, 159 in CPR group)
• Neurologically intact at 1 month – 12.3% ECPR vs. 1.5% CPR
• Neurologically intact at 6 months – 11.2% ECPR vs. 2.6% CPR
Maekawa K, et al. Extracorporeal cardiopulmonary resuscitation for patients with out-of-hospital cardiac arrest of cardiac origin: a propensity-matched study and predictor analysis. (2014)
• Single center post hoc analysis from prospective observational cohort
• Primary Outcome – neurologically intact at 3 months after cardiac arrest
• Compared ECPR vs. conventional CPR
• Propensity scoring was used to compare 24 patients from each group
• Neurologically intact at 3 months – 29% ECPR vs. 8.9% CPR
Johnson NJ, et al. Extracorporeal life support as rescue strategy for out-of-hospital and emergency department cardiac arrest. Resuscitation (2014),
• Dual center prospective observational study
• Primary outcome – discharge from hospital after out of hospital or ED cardiac arrest
• 26 patients included
• 4 patients survived to hospital discharge (15%)
• 3 neurologically intact, 1 unknown
Potential Pros
– Potential life-saving therapy where alternative is certain death
– Allows bridge to definitive therapy
– Improves neurological outcomes and long-term survival in patient with historically poor outcomes
Potential Cons
– Requires well-established ECMO program
– Cost remains a well-stated concern
– Requires numerous resources and is logistically demanding

Further reading
• EDECMO.org – great blog/podcast dedicated to all things ED ECMO
• Extracorporeal Life Support Organization – elso.org o large international organization and registry dedicated to advancement of ECLS
References and Further Reading
1. Bartlett RH, Gazzaniga AB, Jefferies MR, et al. Extracorporeal membrane oxygenation (ECMO) cardiopulmonary support in infancy. Trans Am Soc Artif Intern Organs. 1976;22:80-93.
2. McNally B, Robb R, Mehta M, et al. Out of hospital cardiac arrest surveillance – Cardiac Arrest Registry to Enhance Surrvival (CARES), US, October 1, 2005-December 31, 2010 MMWR Surveill Summ. 2011 Jul 29 ;60(8):1-19.
3. Sasson C, Rogers MA, Dahl J, Kellerman AL. Predictors of survival from out of hospital cardiac arrest: a systematic review and meta-analysis. Circulation Cardiovascular quality and outcomes 2010; 3:63-81.
4. Bro-Jeppesen J, Kjaergaard J, Horsted TI, et al. The impact of therapeutic hypothermia on neurological function and quality of life after cardiac arrest. Resuscitation. 2009 Feb;80(2):171-6
5. Le Guen M, Nicolas-Robin A, Carreira S, et al. Extracorporeal life support following out-of-hospital refractory cardiac arrest. Crit Care 2011; 15:R29.
6. Bellezzo-JM. Emergency Physician-Initiated Extracorporeal Cardiopulmonary Resuscitation. Resuscitation 2012;83:966
7. SAVE-J Study Group. Extracorporeal cardiopulmonary resuscitation versus conventional cardiopulmonary resuscitation in adults with out-of-hospital cardiac arrest: A prospective observational study. Resuscitation. 2014;85(6):762-8. PubMed ID: 24530251
8. Maekawa K, Tanno K, Hase M, et al. Extracorporeal cardiopulmonary resuscitation for patients with out-of-hospital cardiac arrest of cardiac origin: a propensity-matched study and predictor analysis. Crit Care Med 2013; 41:1186–119
9. Johnson NJ, et al. Extracorporeal life support as rescue strategy for out-of-hospital and emergency department cardiac arrest. Resuscitation (2014).
10. Avalli L, Maggioni E, Formica F, et al. Favourable survival of in-hospital compared to out-of-hospital refractory cardiac arrest patients treated with extracorporeal membrane oxygenation: an Italian tertiary care centre experience. Resuscitation 2012; 83:579–583.
11. Chen YS, Lin JW, Yu HY, et al. Cardiopulmonary resuscitation with assisted extracorporeal life-support versus conventional cardiopulmonary resuscitation in adults with in-hospital cardiac arrest: an observational study and propensity analysis. Lancet 2008;372:554–61. 3. Dunne RB, Compton S, Zalenski RJ, Swor R, Welch R, Bock BF.
12. Bellezzo-JM Extracorporeal Cardiopulmonary Resuscitation in the Emergency Department. EM Critical Care. 2012 March
13. Kagawa E, Dote K, Kato M, et al. Should we emergently revascularize occluded coronaries for cardiac arrest?: rapid-response extracorporeal membrane oxygenation and intra-arrest percutaneous coronary intervention. Circulation 2012; 126:1605–1613.
14. http://www.ncbi.nlm.nih.gov/pubmed/22633715 15. http://www.ncbi.nlm.nih.gov/pubmed/21641147





8 thoughts on “Extracorporeal Membrane Oxygenation (ECMO) in the ED”
Pingback: Global Intensive Care | AIR Pro Series: Critical Care, Part 1 (2016)
And another study, just out:
Yannopoulos D et al. Minnesota Resuscitation Consortium’s Advanced Perfusion and Reperfusion Cardiac Life Support Strategy for Out-of-Hospital Refractory Ventricular Fibrillation. Journal AHA. 2016.
Pingback: AEM Early Access 05: The Role of Prehospital ACLS for Potential E-CPR Candidates – Global Intensive Care
Pingback: Podcast #84: Hypothermia and Lightning Strike: Code Baby Code - The Emergency Medical Minute
Pingback: July Conference Schedule 2020 – NewYork-Presbyterian Emergency Medicine
Pingback: Weekly Update – 29 June 2020 – NewYork-Presbyterian Emergency Medicine
Pingback: Conference Learning 1.24.18 – Boston City EM
Pingback: Week 35 – Critical Care – EM Ninja