Author: Alex Koyfman, MD // Editor: Justin Bright, MD
Your next 3 patients…
#1) 23yo MMA fighter with low back pain
#2) 29yo M presents as pedestrian versus auto (“the car bumped my knee and I walked away… now it hurts”)
#3) 34yo M with forearm pain s/p fall off of ladder
–Pathology Cascade: Incr osseofascial compartment pressure from local trauma / soft tissue injury (edema, bleeding) => incr interstitial pressure => decr perfusion => (irreversible) nerve and muscle damage
–Most Common Site: leg (tibial shaft – #1); forearm (#2); hand; foot; thigh; any site where skeletal muscle is covered by fascia is a possibility
–Most Common Patient: Male; less than 35yo
–Causes: fracture, crush injury, GSW, contusion, tight splint/cast, IV infiltration, burn, arterial injury, snakebite, nephrotic syndrome
–Why it’s challenging: can present w/ vague sxs / exam
–Why we care: loss of function / limb
-4 leg compartments
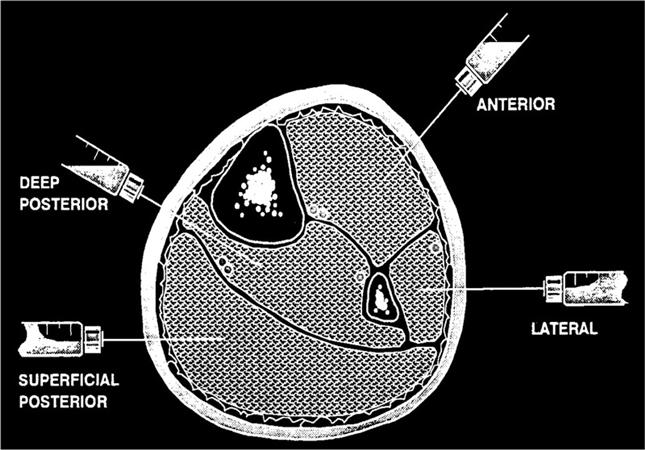
-3 forearm compartments

**Image credit: www.orthobullets.com
Clinical Pearls // Management
–Time is muscle! Time to dx is most important prognostic factor; serial exams are your friend, however understand exam isn’t perfect
–Pain out of proportion/rest pain is usually first symptom (few clinical entities cause this: mesenteric ischemia, deep soft tissue infection, AAA, biliary tract obstruction, bowel obstruction, pancreatitis, stomach/bowel perforation, MI, vascular occlusion, malignant otitis externa)
–not always present or easy to assess (neuropathy, AMS, intubated, polytrauma, young child, unreliable exam)
-important not to treat pain out of proportion to exam as someone opiate seeking
-Most sensitive finding: pain w/ passive stretch; other P’s of compartment syndrome we learned are late findings
(The 6 P’s: pain, paresthesia, pallor, paralysis, pulselessness, poikilothermia)
–Difficult to diagnose in children, thus typically delayed; consider in pt w/ proper context + restlessness / rising opioid requirement (see reference 14 for extended discussion)
-No difference in incidence b/t open vs closed fractures; can develop w/out fracture!!
–4-8 hours is commonly cited cut-off for when irreversible ischemic changes begin to occur (controversial)
-Work-up: XR as indicated; intracompartmental pressure measurements – w/in 5cm of fx site or area of maximal swelling (Stryker, NIRS) for low/medium risk pts; clinical dx in high-risk pts
-Call Gen Surg/Ortho immediately; remove / loosen dressing/splint/cast, elevate extremity, reduce fracture as appropriate
-Usually it is the surgical service doing the intracompartmental pressure measurement; if working in setting without surgical backup, important to know how to do it (https://www.youtube.com/watch?v=rtysrBh7AP0)
–Emergent fasciotomy: clinical dx or compartment pressures 30-45 mm Hg (exact # controversial and test w/ limitations – see reference 4) / compartment pressures within 30 mm Hg of DBP (delta P); controversial if late identification of compartment syndrome
References // Further Reading
1) http://www.ncbi.nlm.nih.gov/pubmed/24686026
2) http://www.ncbi.nlm.nih.gov/pubmed/24560014
3) http://www.ncbi.nlm.nih.gov/pubmed/23816339
4) http://www.ncbi.nlm.nih.gov/pubmed/23321294
5) http://www.ncbi.nlm.nih.gov/pubmed/23340119
6) http://www.ncbi.nlm.nih.gov/pubmed/23200336
7) http://www.ncbi.nlm.nih.gov/pubmed/23200335
8) http://www.ncbi.nlm.nih.gov/pubmed/22981663
9) http://www.ncbi.nlm.nih.gov/pubmed/22325557
10) http://www.ncbi.nlm.nih.gov/pubmed/20005667
11) http://www.ncbi.nlm.nih.gov/pubmed/20925169
12) http://lifeinthefastlane.com/ortho-library/compartment-syndrome/
13) http://lifeinthefastlane.com/bone-and-joint-bamboozler-002/
14) http://pedemmorsels.com/compartment-syndrome/
15) http://www.epmonthly.com/departments/cme/cme-archive/diagnosing-compartment-syndrome/





2 thoughts on “Compartment Syndrome: Pearls and Pitfalls”
Pingback: Compartment Syndrome | Medic Mindset