Authors: Patrick C Ng, MD (EM Chief Resident, SAUSHEC Emergency Medicine Department) and Brit Long, MD (@long_brit, EM Attending Physician, SAUSHEC Emergency Medicine Department) // Edited by: Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UTSW / Parkland Memorial Hospital) and Stephen Alerhand, MD (@SAlerhand)

Case 1
You get a call from EMS that they are en route to your ED with a 37-year-old male who was found down in a sewer, with a current CGS of 3. The patient is being ventilated with a BVM. ETA 2 minutes!
The patient arrives to your ED. You immediately set up your safety net of bilateral IVs, oxygen, and get the patient on the cardiac monitor. As you begin your resuscitation, EMS repeats that the patient was found down in a sewer. His colleagues report that he was working in there alone and was radio silent for approximately 30 minutes before EMS arrived. EMS reports a strong odor at the scene resembling rotten eggs. The patient had been found without any PPE or respirators on.
Vitals: BP 170/80, HR 100, RR 0, Temp 100.0°F, Sat 86% with 15L of oxygen via BVM
Recognizing that this patient is apneic and unresponsive, you prepare for intubation. Upon inserting the laryngoscope, copious amounts of a pink, frothy substance emerge from the airway. With suctioning, you get a grade 1 view and intubate successfully. In consultation with the poison control center for suspected hydrogen sulfide toxicity, you resuscitate the patient with fluids and administer sodium nitrite to induce methemoglobinemia.
Resulting labs are significant for a white blood cell count of 12.1 x 109, pH of 7.23, PaCO2 72 mm Hg, PaO2 51, and Lactate of 5.6 mmol/L. Troponin was normal.
CXR revealed bilateral pulmonary infiltrates and an ET tube 1 cm above the carina.
Head CT was negative for sign of trauma or CVA.
The patient was admitted to the MICU for respiratory failure and lactic acidosis likely secondary to hydrogen sulfide toxicity.
Introduction
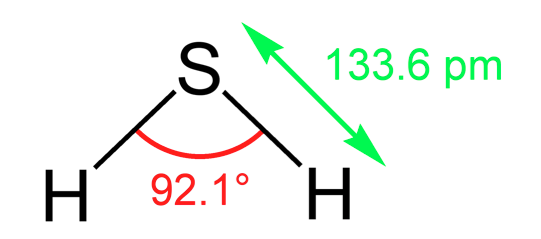
Hydrogen sulfide is a triatomic molecule that is typically found as a gas (Figure 1). It is a natural substance that is formed by the digestion of organic material by prokaryotes in the environment. Typically, hydrogen sulfide is found in sewers, wells, volcanoes, and hot springs1. Additionally, hydrogen sulfide is a major occupational hazard in the oil and gas industry. It is a component of natural gas, and a significant amount of the gas can be released in the extraction and refining of natural gas through hydraulic fracturing aka ‘fracking’2. Fracking is a process of drilling where a mixture containing water, chemicals, and sand is directed at rock at a high pressure causing fractures in the rock to allow the natural gas to flow out to the well head3.
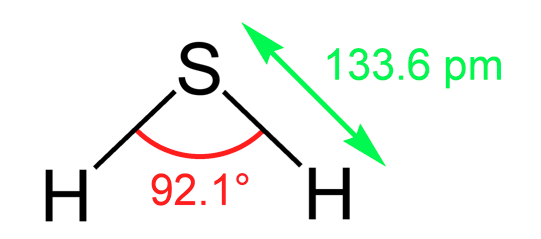
Figure 1: Molecular structure of H2S
Permissible OSHA exposure is 20ppm during an 8-hour shift
Over the past decade, particularly in Japan, there has been an increase in reports of “detergent suicides”, where individuals have been mixing household products such as toilet bowl cleaners and insecticides, which serve as a proton donor and sulfur source respectively, to commit suicide. The combination of these products can form H2S gas in toxic concentrations leading to toxicity, particularly when in an enclosed environment4. This also poses a threat to neighbors and first responders who can also be exposed to the gas6.
There are varying degrees of H2S toxicity. Variables such as length of exposure and concentration of exposure have direct effects on the level of toxicity (Table 1). Exposures to the gas can cause intense upper airway irritation, conjunctivitis, coughing, seizure, and dyspnea1,7. At higher concentrations, cardiac arrest, myocardial infarction, and death can occur1,7-9. The “knockdown” effect is described as a sudden loss of consciousness when exposed to high concentrations of H2S; the exact pathophysiology of this is not well known1. H2S has also been reported to cause olfactory fatigue, which can result from prolonged exposure as the classic rotten egg smell dissipates5.
In the body, hydrogen sulfide hinders aerobic respiration by inhibiting cytochrome c oxidase in the mitochondria. This inhibits mitochondrial ATP production. This mechanism of toxicity is similar to cyanide toxicity. Additionally, H2S is thought to poison the brain, particularly in the respiratory centers leading to central apnea11. Also, it affects the L-type calcium channels in the heart causing arrythmia13. Hydrogen sulfide toxicity can result in coma, apnea, shock, and eventually cardiac arrest.
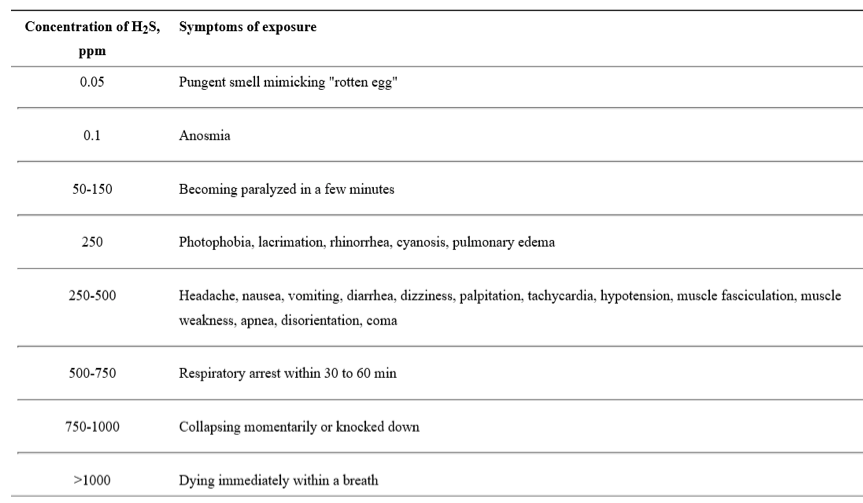
Table 1: Effects of H2S at various concentrations (Table reproduced from Morii et al)5
Key ED Work Up
For suspected H2S toxicity and with the understanding of complications such as pulmonary edema, apnea, and cardiac arrhythmia, it is important to monitor these patients very closely. Initial workup should include: VBG to assess respiratory status, lactate level as H2S can precipitate a profound lactic acidosis, a chest x-ray to assess for presence of pulmonary symptoms/edema, an ECG to assess for arrhythmias, and continuous cardiac monitoring as H2S toxic patients are at risk for cardiac arrhythmia. Since there is no diagnostic test to diagnose H2S toxicity, the ED provider must have a high clinical suspicion for this diagnosis based on history and physical. Consider basic labs such as CBC and Chem 8 as well as further imaging to assess for trauma in patients found unconscious. Co-oximetry should be considered as well in these inhalation injuries, particularly if sodium nitrite is used as therapy, as it causes a methemoglobinemia which can be monitored with co-oximetry. The EM provider must consider other gases that may have also been inhaled including but not limited to cyanide and carbon monoxide. Additionally, ophthalmologic complications have been reported and must be considered.
Key Management Principles
The first step in managing a patient exposed to H2S is to remove them from the exposure and to be aware of possible secondary exposure to bystanders and first responders. Rapid assessment of the ABCs is warranted and aggressive supportive care should take place. Sodium nitrite (0.33mL/kg of 3% solution) has been reported to treat hydrogen sulfide poisoning 1,17. There is no consensus on the proper dosing of sodium nitrite. Sodium nitrite induces a methemoglobinemia which increases hemoglobin’s ability to bind H2S. Sodium nitrite can cause hypotension, and induction of a methemoglobinemia in an apneic patient can worsen tissue hypoxia and end organ damage. Thus, aggressive supportive care with IV fluids and mechanical ventilation in a patient poisoned with H2S is of paramount importance. Close monitoring of methemoglobin is important, and co-oximetry should be obtained to measure methemoglobin levels 30 minutes after administration of sodium nitrite. There are several reports of using hyperbaric oxygen to treat H2S toxicity as well 13-14. Recently, there have been animal models that have demonstrated that the use of cobinamide, a vitamin b12 analog, may be effective in treating H2S toxicity, but this is still in the nascent stages of development18. Hydroxocobalamin and methylene blue have also been reported to be used for H2S toxicity19,20. Management of H2S exposures should take place with toxicology consultation.
Summary
-Hydrogen sulfide exposures can be deadly.
-Hydrogen sulfide exposures can happen in various industrial settings as well as in the home as a suicide attempt.
–Removal of the patient from the exposure as soon and as safely as possible is a key initial step.
–Aggressive supportive care is the mainstay of treatment.
–Sodium nitrite and other nitrite formulations can be used to induce a methemoglobinemia to treat H2S toxicity. Hyperbaric oxygen, methylene blue, and hydroxocobalamin have also been used.
-There is no consensus on dosing of sodium nitrite, and one must consider the drug’s side effects including hypotension.
–Cobinamide, a hydroxocobalamin derivative, may serve as an effective intramuscular antidote for H2S toxicity in the future.
References/Further Reading
- Yalamanchili C, Smith MD. Acute hydrogen sulfide toxicity due to sewer gas exposure. Am J Emerg Med 2008 May;26(4):518.
- The Process of Hydraulic Fracturing. https://www.epa.gov/hydraulicfracturing/process-hydraulic-fracturing; last accessed 15July2016.
- Carpenter DO. Hydraulic fracturing for natural gas: impact on health and environment. Rev Environ Health 2016 Mar;31(1):47-51.
- Reedy SJ, Schwartz MD, Morgan BW. Suicide Fads: Frequency and Characteristics of Hydrogen Sulfide Suicides in the United States. West J Emerg Med 2011 Jul;12(3):300-304.
- Morii D, Miyagatani Y, Nakamae N, Murao M, Taniyama K. Japanese experience of hydrogen sulfide: the suicide craze in 2008. J Occup Med Toxicol 2010;5:28.
- Knight LD, Presnell SE. Death by sewer gas: case report of a double fatality and review of the literature. Am J Forensic Med Pathol 2005 Jun;26(2):181-5.
- Truscott A. Suicide fad threatens neighbours, rescuers. CMAJ 2008 Aug 12;179(4):312-313.
- Lewis RJ, Copley GB. Chronic low-level hydrogen sulfide exposure and potential effects on human health: a review of the epidemiological evidence. Crit Rev Toxicol 2015 Feb;45(2):93-123.
- Wu N, Du X, Wang D, Hao F. Myocardial and lung injuries induced by hydrogen sulfide and effectiveness of oxygen therapy in rats. Clin Toxicol (Phila). 2011 Mar;49(3):161-6.
- Fiedler N, Kipen H, Ohman-Strickland P, Zhang J, Weisel C, Laumbach R et al. Sensory and cognitive effects of acute exposure to hydrogen sulfide. Environ Health Perspect 2008 Jan;116(1):78-85.
- Warenycia MW, Goodwin LR, Benishin CG, Reiffenstein RJ, Francom DM, Taylor JD et al. Acute hydrogen sulfide poisoning. Demonstration of selective uptake of sulfide by the brainstem by measurement of brain sulfide levels. Biochem Pharmacol 1989 Mar 15;38(6):973-81.
- Chenuel B, Sonobe T, Haouzi P. Effects of infusion of human methemoglobin solution following hydrogen sulfide poisoning. Clin Toxicol (Phila) 2015 Feb;53(2):93-101.
- Chen J, Chen S, Mao W. A Case of Survival: Myocardial Infarction and Ventricular Arrhythmia Induced by Severe Hydrogen Sulfide Poisoning. Cardiology. 2016 May 19;135(1):43-47.
- Asif MJ, Exline MC. Utilization of hyperbaric oxygen therapy and induced hypothermia after hydrogen sulfide exposure. Respir Care 2012 Feb;57(2):307-10.
- Belley R, Bernard N, Cote M, Paquet F, Poitras J. Hyperbaric oxygen therapy in the management of two cases of hydrogen sulfide toxicity from liquid manure. CJEM 2005 Jul;7(4):257-61.
- Smilkstein MJ, Bronstein AC, Pickett HM, Rumack BH. Hyperbaric oxygen therapy for severe hydrogen sulfide poisoning. J Emerg Med 1985;3(1):27-30.
- Fujino Y, Inoue Y, Onodera M, Kikuchi S, Endo J, Endo S et al. Case followed by delayed loss of consciousness after exposure to hydrogen sulfide that was treated with intermittent administration of sodium nitrite. Chudoku Kenkyu 2010 Dec;23(4):297-302.
- Jiang J, Chan A, Ali S, Saha A, Haushalter KJ, Lam WL et al. Hydrogen Sulfide—Mechanisms of Toxicity and Development of an Antidote. Sci Rep 2016 Feb 15;6:20831.
- Judenherc-Haouzi A, Zhang XQ, Sonobe T, Song J, Rannals MD, Wang J et al. Methylene blue counteracts H2S toxicity-induced cardiac depression by restoring L-type Ca channel activity. Am J Physiol Regul Integr Comp Physiol 2016 Jun 1;310(11):R1030-44.
- Haouzi P, Sonobe T, Judenherc-Haouzi A. Developing effective countermeasures against acute hydrogen sulfide intoxication: challenges and limitations. Ann N Y Acad Sci 2016 Jun;1374(1):29-40.
Acknowledgements
Thank you to Dr. Daniel Sessions, Dr. Joseph K Maddry, and Dr. Vikhyat S Bebarta, Medical Toxicologists and EM physicians for their meaningful feedback while producing this document.




