Author: Brit Long, MD (@long_brit) // Reviewed by: Manny Singh, MD (@MPrizzleER) and Alex Koyfman, MD (@EMHighAK)
In the midst of the current COVID-19 pandemic, we often focus on pulmonary complications including hypoxemic respiratory failure. However, patients with COVID-19 are at risk of cardiac complications including heart failure, myocarditis, acute myocardial infarction (AMI), and several others. Even more challenging is that many patients with cardiovascular disease and AMI may not be infected with COVID-19.
Fortunately, the American College of Cardiology, the American College of Emergency Physicians, and the Society for Cardiovascular Angiography and Interventions published a joint statement in the Journal of the American College of Cardiology, detailing personal protective equipment (PPE), ST elevation myocardial infarction (STEMI) and NSTEMI management, emergency medical systems (EMS), and systems of care. For full access, please visit the Journal of the American College of Cardiology. The goals of this article were to 1) minimize EMS and healthcare provider exposure to COVID-19 while ensuring patients receive the appropriate level of cardiac care, 2) target PCI or fibrinolysis (at non-PCI capable hospitals) in STEMI patients and avoid reperfusion therapy for those with other causes of ST-segment elevation ECG, and 3) maximize the safety of medical personnel by appropriate masking of patients and use of PPE
This post will provide a succinct summary of these recommendations to help you on your next shift.
Systems of Care
Regional STEMI systems should update system of care including PPE during transport and procedures for STEMI in COVID-19 positive/probable patients.
First medical contact to reperfusion time is important, and delays to primary PCI for STEMI should be avoided. There may be a delay at primary PCI centers in the ED for confirmation of COVID-19 and STEMI status prior to transfer to the cath lab.
STEMI patients with shock and/or resuscitated cardiac arrest should still be prioritized for primary PCI. If PCI is not possible, or if the team/room/PPE is not available, fibrinolysis can be considered.
PPE, rapid sterilization procedures, and communication of patient COVID-19 status must prioritized throughout the entire system including transfer hospitals, EMS, ED, and cath lab.
Each system must recognize the competing and equally important principles of timely reperfusion of STEMI patients, safe regional transport and treatment of potentially high-risk patients, and additional emphasis on protection and safety of all health care personnel.
Emergency Medical Services
EMS should conduct a brief assessment of COVID-19 status in their report to the center. ED bypass is not recommended.
EMS providers should have a low threshold to wear appropriate PPE when responding to those with primary cardiac complaints. If responding to a patient with cardiac arrest, PPE is critical.
If the patient is at a referral (non-PCI capable) hospital with established COVID-19, fibrinolysis within 30 minutes of STEMI diagnosis and transfer when necessary for rescue PCI may be preferable.
Regarding a field STEMI activation, the patient should be evaluated in the ED to assess for COVID-19 and confirm diagnosis of STEMI.
Figure 1. EMS Field STEMI

Patients with STEMI presenting to a PCI Center
All STEMI patients should be evaluated in the ED prior to cath lab activation. Patients should have a face mask placed to prevent droplet contamination.
PCI remains the standard of care for patients presenting to PCI centers, including COVID-19 confirmed or probable patients. Many of these patients with COVID-19 may have a myocarditis or stress cardiomyopathy, and fibrinolysis increases the risk of bleeding in these patients.
The ED should focus on cath lab transfer as soon as possible in cases of confirmed STEMI. While door to balloon time of < 90 minutes from first medical contact is recommended, the article acknowledges there may be delays due to further evaluation and management required, including ultrasound (US) for wall motion abnormalities, assessment of COVID-19 status, and respiratory support. This should be appropriately documented.
If COVID-19 is probable or confirmed, and the patient has symptoms and ECG consistent with AMI, the article states ultrasound can be considered to evaluate for wall motion abnormality, but proceed to primary PCI. If COVID-19 is possible and symptoms and ECG are consistent with AMI, proceed to PCI (Figure 2).
If primary PCI is not feasible, a pharmacoinvasive approach with fibrinolysis may be considered (see below).
PCI should always be performed with PPE for aerosolized and droplet precautions for the cath team. A single negative pressure procedure room is preferred for COVID-19 confirmed or probable patients.
Patients with respiratory failure should be intubated prior to arriving at the cath lab.
Possible STEMI
In patients with equivocal symptoms, atypical ECG, or delayed presentation and possible but not confirmed STEMI, further evaluation in the ED is recommended. Use US, serial ECGs, and chest x-ray, while also evaluating for other conditions such as COVID-19 myocarditis. At this time, a joint decision between the emergency clinician and interventional cardiologist is recommended to determine further evaluation and management. If the patient is unstable, an invasive approach in the cath lab is recommended.
Futile Prognosis
Not all patients with COVID-19 and STEMI benefit from reperfusion or mechanical support. In those with critical disease at high risk for mortality (including ARDS and mechanically ventilated), compassionate care may be appropriate. This decision should be based on individual patient prognosis, patient/family wishes, and resources available at the local center.
Figure 2. STEMI.

Patients with STEMI at Referral Centers (non-PCI capable)
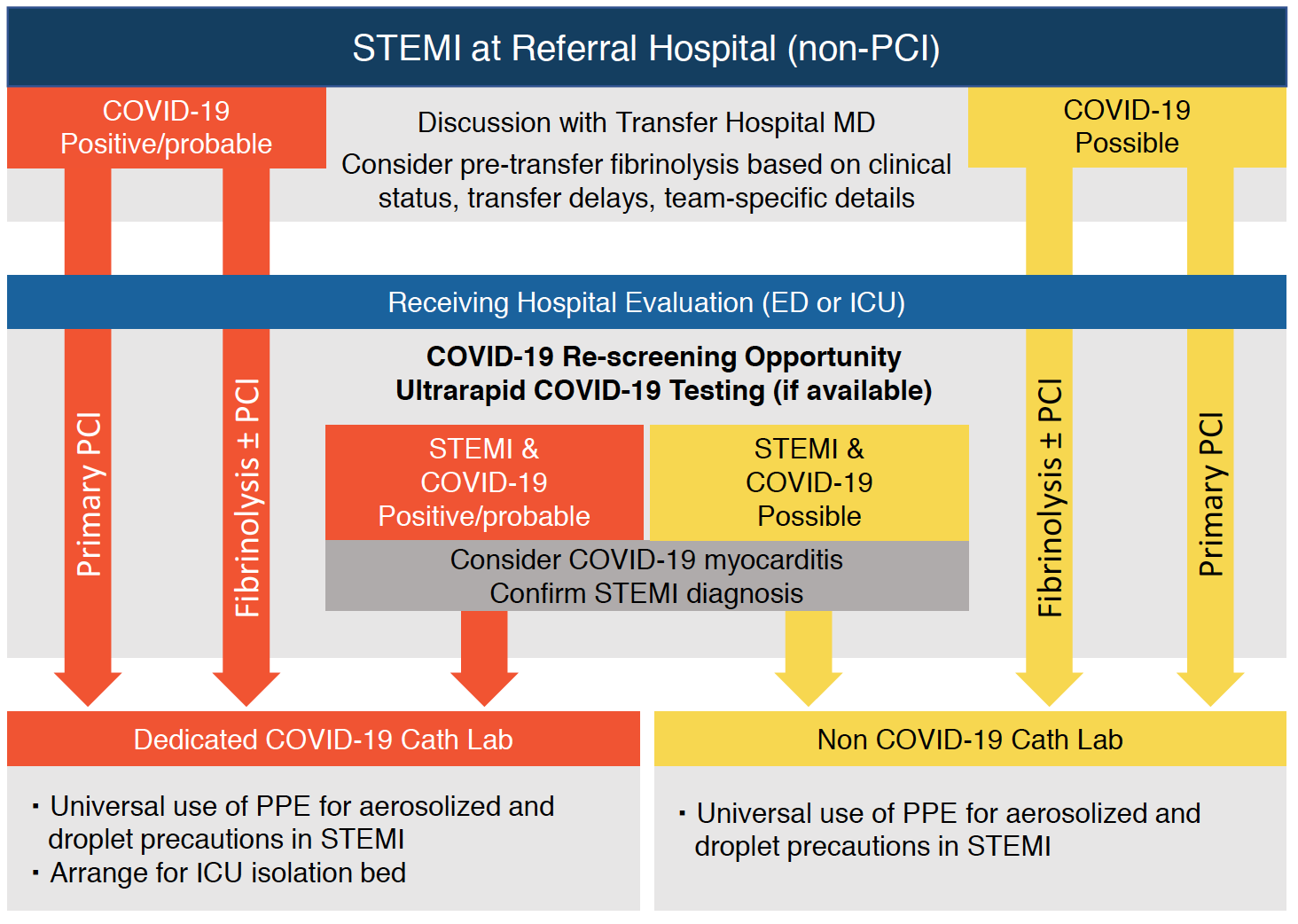
If primary PCI is not feasible, fibrinolytics may be administered, followed by consideration of transfer to a PCI-capable center. This decision should be discussed with the physician at the PCI center. Fibrinolysis within 30 minutes of STEMI diagnosis and transfer for rescue PCI when necessary may be preferable for all COVID-19 STEMI patients at a referral hospital if STEMI is likely (Figure 3).
Initial fibrinolysis therapy may be used in non-PCI capable hospitals if the first medical contact to reperfusion is felt to be > 120 minutes. Additional noninvasive imaging can help determine whether ST-elevation on the ECG is due to occluded coronary artery.
Figure 3. STEMI at Referral Hospital.
Patients with Cardiogenic Shock and/or Out-of-Hospital Cardiac Arrest (OHCA)
Patients with cardiogenic shock or OHCA have poor outcomes and are high risk for droplet-based spread of COVID-19. Resuscitated OHCA patients should be selectively considered for cath lab activation if persistent STEMI is present on ECG and wall motion abnormality on US is present. OHCA patients without STEMI should not receive an early intervention approach unless hemodynamically unstable and acute coronary occlusion is high on the differential diagnosis.
Mechanical circulatory support with revascularization may be considered for those with cardiogenic shock (team in full PPE). VV ECMO should be considered in those with severe pulmonary decompensation and failure to oxygenate.
Patients with NSTEMI
Elevated troponin is a poor prognostic marker in patients with COVID-19. Cardiac injury likely occurs due to several mechanisms. Patients with COVID-19 and NSTEMI should be managed medically and only taken for urgent angiography and possible PCI if high risk features are present (GRACE > 140), or if hemodynamically unstable.
Those with COVID-19 (confirmed or probable) and NSTEMI but no high-risk features can be managed with guideline-initiated medical therapies, and once stabilized, further evaluation as an outpatient is recommended once the infection has resolved.
For those with possible COVID-19 and ACS, standard medical therapy is indicated, with an early invasive approach if clinically indicated. Rapid COVID-19 testing is recommended to guide further evaluation and management.
Further Reading:
JACC – Management of Acute Myocardial Infarction During the COVID-19 Pandemic
REBEL EM – Cardiovascular Considerations
Emergency Medicine Cases – Cardiovascular Emergencies During The COVID-19 Pandemic





1 thought on “Managing the Patient with AMI and COVID-19 – JACC Consensus Statement”
Pingback: COVID-19: Cardiovascular Considerations - REBEL EM - Emergency Medicine Blog