
Authors: Richard B. Moleno DO, MS (EM Resident Physician, UTSW/Parkland Memorial Hospital) and Ashley Haynes MD (Toxicology Fellow, UTSW/Parkland Memorial Hospital) // Edited by: Alex Koyfman MD (@EMHighAK) and Stephen Alerhand MD (@SAlerhand)
Case Presentation
A 43 year-old woman with a past medical history of depression, DM, and HTN presents to the Emergency Department 2.5 hours after a suicide attempt by prescription drug ingestion. She reports that feeling upset with her home situation and ingested a “handful” of Metformin 500mg tablets in addition to drinking three 40oz beers. Initial vitals are HR 109, BP 165/96, Temp 36.4 and SpO2 on RA of 98%. Review of pill count from the Metformin bottle provided by EMS is significant for 30 missing pills (15g of Metformin). Being the astute and vigilant resident physician that you are, you quickly ask the nurse to move the patient into a critical care booth, as you remember learning about the dangers of Metformin during your toxicology rotation. Nursing begrudgingly complies. What should be done next?

Background
Metformin, a biguanide derived from guanidine, was introduced in the 1950’s as a treatment for diabetes, and remains widely used today with 40 million prescriptions filled worldwide in 2008 (1). Lactic acidosis is the primary toxicity of concern, with an estimated incidence of 0.03 per 1000 patients/year (2). Metformin-associated lactic acidosis may happen with therapeutic doses or after an acute overdose. Currently the data is mixed as to which situation leads to a more severe pattern of illness. Common initial symptoms are non-specific and include nausea, vomiting, diarrhea, abdominal pain, malaise, and decreased oral intake. In severe cases, altered mental status, tachypnea, hypothermia or cardiovascular collapse may occur.
Diagnosis
The diagnostic criteria for MALA are not well defined in the literature. Labs to obtain include a CBC, CMP, Lactate, and blood gas for determining pH. In intentional overdoses, make sure to also check for life-threatening co-ingestions (APAP/ASA). In general, the diagnosis should be considered in any patient with a lactate >5 mg/dl and the presence of Metformin (in either routine use or overdose). An elevated anion gap may also be suggestive. The possibility of diagnostic confusion can occur since this definition often overlaps with the more common diagnosis of diabetic ketoacidosis (DKA).
Pathophysiology
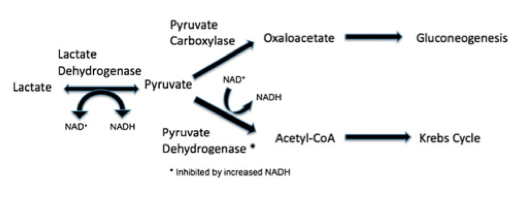
Metformin works via reducing gluconeogenesis, increasing peripheral uptake of glucose, and decreasing fatty acid oxidation. This in turn increases lactic acid formation. Metformin also inhibits pyruvate carboxylase, further increasing formation of lactate (3).
Metformin is excreted unchanged by the kidneys. In most cases where intentional ingestion is not the culprit, MALA occurs secondary to decreased Metformin excretion (due to kidney dysfunction). The elimination half-life is approximately 17 hours and 90% of the drug is excreted by the kidneys within 24 hours. One can see how someone who is on Metformin chronically can develop MALA in the setting of renal insufficiency (3).
Management
The initial step in treating any patient with a poisoning should be to call the poison control center at 1-800-222-1222. A toxicologist should be involved early in these cases. The mainstay of treatment is supportive care, but this will need to be done in an ICU setting. Patients will need frequent blood gases and lactate measurements. Certainly, Metformin should be discontinued during any critical illness or in any patient with elevated lactate levels. Sodium bicarbonate infusions may be used to correct acidosis (4). While low arterial pH and high lactate have been reported as prognostic factors, a recent review of pharmaco-vigilance data demonstrated a lack of prognostic value of these measures, with survival of patients even with pH as low as 6.5 (5).

The extracorporeal removal of Metformin has also been considered and utilized in a number of cases. Metformin has low molecular weight and limited protein binding, but a large volume of distribution (6). Continuous renal replacement therapy may need to be continued for longer periods of time if the goal is drug removal, due to this large Vd, especially after large overdoses (7). While there are currently no clear indications for dialysis methods for MALA, it can be considered for the associated renal failure, in the setting of very large overdoses or to correct severe acidemia.
Our Case
Our patient was admitted to the ICU. She received IVF, and q4h VBGs and Lactates. Initial labs revealed a lactate of 4.1, an anion gap of 21 and a pH of 7.37. Her lactate peaked at 6.2 and her lowest recorded pH via VBG was 7.33. She did not end up requiring bicarbonate infusion or hemodialysis, only IVF. She was eventually discharged from the hospital after psychiatric evaluation 36 hours after admission.
Major Points
– MALA is a rare but life-threatening condition seen after use of Metformin. The condition should be considered in patients who present with elevated lactate (>5 mg/L) and acidemia.
– Get your local toxicologist involved early, as it carries a high mortality, up to 50%.
-The management is mainly supportive, but Metformin use must be stopped and intravenous bicarbonate can be infused to correct severe acidosis.
–Renal replacement therapy can be used to remove the drug and also to correct the acidosis. If you are not at a facility that has hemodialysis capabilities, you should transfer the patient to a center capable of this higher level of care.
-Survivors tend to regain kidney function.
References/Further Reading
- Available at: http://drugtopics.modernmedicine.com/drug-topics/news/modernmedicine/modern-medicine-news/2009-top-200-generic-drugs-total-prescriptions?page=full. Accessed September 25, 2015.
- Van berlo-van de laar IR, Vermeij CG, Doorenbos CJ. Metformin associated lactic acidosis: incidence and clinical correlation with metformin serum concentration measurements. J Clin Pharm Ther. 2011;36(3):376-82.
- Kopec KT, Kowalski MJ. Metformin-associated lactic acidosis (MALA): case files of the Einstein Medical Center medical toxicology fellowship. J Med Toxicol. 2013;9(1):61-6.
- Wen YK. Impact of acute kidney injury on metformin-associated lactic acidosis. Int Urol Nephrol. 2009;41(4):967-72
- Misbin RI, Green L, Stadel BV, Gueriguian JL, Gubbi A, Fleming GA. Lactic acidosis in patients with diabetes treated with metformin. N Engl J Med. 1998;338(4):265-6.
- Juurlink DN, Roberts DM. The enigma of metformin-associated lactic acidosis. Clin Toxicol (Phila). 2014;52(2):85-7.
- Rifkin SI, Mcfarren C, Juvvadi R, Weinstein SS. Prolonged hemodialysis for severe metformin intoxication. Ren Fail. 2011;33(4):459-61.
- http://www.ncbi.nlm.nih.gov/pubmed/26241713
- http://www.ncbi.nlm.nih.gov/pubmed/18571361
- http://www.ncbi.nlm.nih.gov/pubmed/20887905





4 thoughts on “Metformin Associated Lactic Acidosis (MALA): ED-focused management”
Overall nice summary, however, I paused at these lines: “Metformin-associated lactic acidosis may happen with therapeutic doses or after an acute overdose. Currently the data is mixed as to which situation leads to a more severe pattern of illness.”
A very thorough 2010 Cochrane Review (http://www.ncbi.nlm.nih.gov/pubmed/20393934) looked at therapeutic metformin use and risk of lactic acidosis, and concluded:
“Pooled data from 347 comparative trials and cohort studies revealed no cases of fatal or nonfatal lactic acidosis in 70,490 patient-years of metformin use or in 55,451 patients-years in the non-metformin group. Using Poisson statistics the upper limit for the true incidence of lactic acidosis per 100,000 patient-years was 4.3 cases in the metformin group and 5.4 cases in the non-metformin group. There was no difference in lactate levels, either as mean treatment levels or as a net change from baseline, for metformin compared to non-metformin therapies…There is no evidence from prospective comparative trials or from observational cohort studies that metformin is associated with an increased risk of lactic acidosis, or with increased levels of lactate, compared to other anti-hyperglycemic treatments.”
It honestly doesn’t seem mixed to me.
Overall nice summary, however, I paused at these lines: “Metformin-associated lactic acidosis may happen with therapeutic doses or after an acute overdose. Currently the data is mixed as to which situation leads to a more severe pattern of illness.”
A very thorough 2010 Cochrane Review (http://www.ncbi.nlm.nih.gov/pubmed/20393934) looked at therapeutic metformin use and risk of lactic acidosis, and concluded:
“Pooled data from 347 comparative trials and cohort studies revealed no cases of fatal or nonfatal lactic acidosis in 70,490 patient-years of metformin use or in 55,451 patients-years in the non-metformin group. Using Poisson statistics the upper limit for the true incidence of lactic acidosis per 100,000 patient-years was 4.3 cases in the metformin group and 5.4 cases in the non-metformin group. There was no difference in lactate levels, either as mean treatment levels or as a net change from baseline, for metformin compared to non-metformin therapies…There is no evidence from prospective comparative trials or from observational cohort studies that metformin is associated with an increased risk of lactic acidosis, or with increased levels of lactate, compared to other anti-hyperglycemic treatments.”
It honestly doesn’t seem mixed to me.
Pingback: emDOCs.net – Emergency Medicine EducationEM Educator Series: MALA exists and is bad for you! - emDOCs.net - Emergency Medicine Education
Pingback: Week 39 – Endocrine – EM Ninja