
Author: Bo Burns, DO, FACEP (George Kaiser Foundation Chair in Emergency Medicine, Associate Professor and Program Director, Department of Emergency Medicine, University of Oklahoma School of Community Medicine) // Edited by: Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UT Southwestern Medical Center / Parkland Memorial Hospital) and Brit Long, MD (@long_brit)
“Remember that patient that you saw? The patient with gastroenteritis? Well they came back with a perforated appendicitis and overwhelming sepsis. Wow, you really dropped the ball didn’t you?” Those words that we as educators may utter possess great power, most of the time don’t need to be said, and along with the related clinical experience might have a lasting negative impact that could influence that particular care team for quite some time. That experience might shape both the immediate feelings/perceptions through what is known as the ‘second victim’ phenomenon but can help to form unhealthy negative coping mechanisms and emotions with less job satisfaction and increased feelings of burnout over time. “Second victims” are health care providers who have been involved with patient adverse events and who subsequently develop difficulty coping with their emotions. This has received well-deserved attention, but the interaction of mindset and how it impacts the second victims is yet to be determined. (Suggested reading on Second Victims below).
As educators our learners will experience mistakes, setbacks, fatigue, burnout, bias, adverse events, a missed MI, failed airways, unexpected patient deaths, missed fractures, and applying incorrect diagnoses. These experiences come by many names, but it is an inevitable part of our training (and professional life). For many of us in medical education the first time that our residents experience this is in the post-graduate training phase. Not only are they caring for patients (even though supervised) in a more independent fashion, this may be the first time that many of our very driven, goal oriented high achievers make a mistake or experience a significant life setback.
Over the past decade interacting with many EM residents at various levels of training, I have witnessed many mistakes and setbacks of varying severity and clinical relevance. With time, I have come to embrace these moments as a time to build trust, provide support, listen, and help gain insight into the mindset of the resident. I will admit, when I first became Program Director I dealt with these type of situations in more of a punitive fashion. (“Let’s talk about what you did wrong.”) The understanding of the Mindset concept has helped me a great deal to open up a meaningful dialogue and gain understanding, then to provide support and instruction.
The students and residents who we mentor and teach are very gifted and have much more experience with success and accolades than failure. These difficult situations may represent uncharted waters and will require dedicated time and attention on our part to ensure that these events are approached, understood, and ultimately resolved in the healthiest way possible.
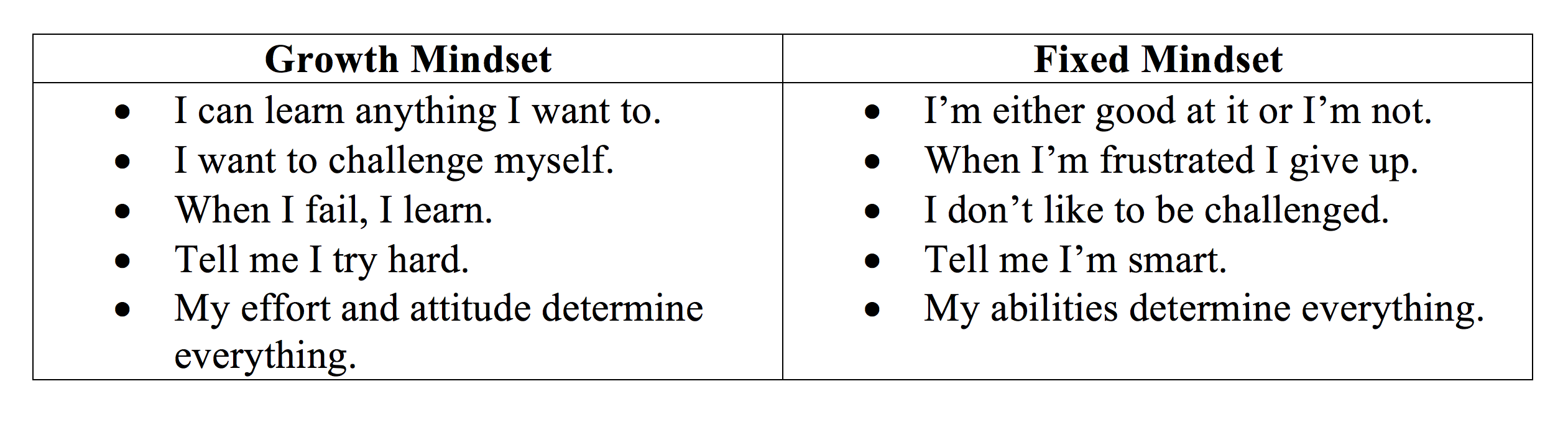
In her book Mindset: The New Psychology of Success, Dr. Carol Dweck explains how the Mindset of the individual can be a great determinant of their success. She makes the distinction between what is referred to as the ‘Fixed’ vs a ‘Growth’ mindset. This book and the concepts discussed therein have helped me on numerous occasions to have more meaningful interactions with my students and residents (and Faculty) and has helped me to understand how to help our trainees navigate and work through a setback in a much more meaningful way. Dr. Dweck discusses that praising learners for their talent instead of hard work does not build mental toughness or build confidence or help to develop resiliency and can actually be counterproductive. This is albeit a much shorter review and description of the significance of the impact mindset can have during the evaluation and feedback process than is discussed in the book.
I suspect that many of us in medical education might recognize some examples of a Fixed mindset or that pivotal moment when the mindset of the learner is revealed. The defensive pushback we encounter when we discuss a “miss” or the frustration/anger that is voiced from a learner after critical feedback received from an evaluation. If you witness a learner push back, become defensive, and seem to give up with this type of feedback, this should be an indication to us of the mindset (at that time) of the learner. This reflects the belief that their intelligence and talent are fixed, and no amount of effort or energy can change or improve these qualities. As you can imagine, the quality and content of the conversation will improve as the distance increases from an emotional event.
Producing a growth mindset in your learners (and yourself) will take time and effort on our part. We should view these tough conversations as wonderful opportunities to build trust with our learners and demonstrate to them that their intelligence and talent are not fixed qualities and do not determine their worth. The Growth Mindset is one that welcomes challenges and opportunities as opposed to the Fixed, which places more value on praise and accolades. This mindset believes that the most basic qualities of the learner, like talent and intelligence, can be improved upon by dedication and hard work.
After reading existing work on this concept, I have tried to incorporate these concepts into our resident and student curriculums. I no longer try “to win” these crucial (non-behavioral) conversations that I have with my students and residents but simply listen to understand, to make sure that they are listened to and to gain insight into their mindset. We must recognize these times of stress and setbacks as great opportunities to help our learners navigate successfully and lay the framework for their future. Just as a novice learner requires our direct training initially, they recall it more over time as competence develops. This same principle applies to the development of Mindset, and part of how we do that is to help identify characteristics of the type of mindset they possess at that particular time. I have witnessed on many occasions that a learner who at a time displays characteristics of a Fixed Mindset will not internalize feedback as well as the Growth Mindset. The defenses that are ‘up’ prevent the introspection necessary to make the steps to objectively consider the feedback, evaluate the situation, review the event in question, or to discuss that mistake.
We introduce these concepts to our students and residents, at regular intervals outside of crucial or difficult conversations. The hope is that this training, coupled with resiliency development, and overall wellness will produce physicians much more comfortable with challenges and self-evaluation who are less likely to suffer from burnout.
Suggested Reading
- Mindset: The New Psychology of Success. Dweck, C.
- Mira JJ, Lorenzo S, Carrillo I, et al. Interventions in health organisations to reduce the impact of adverse events in second and third victims. BMC Health Services Research. 2015;15:341. doi:10.1186/s12913-015-0994-x.
- Burlison JD1, Quillivan RR, et al. The Effects of the Second Victim Phenomenon on Work-Related Outcomes: Connecting Self-Reported Caregiver Distress to Turnover Intentions and Absenteeism. J Patient Saf. 2016 Nov 2. PMID: 27811593
- Grissinger M. Too Many Abandon the “Second Victims” Of Medical Errors. Pharmacy and Therapeutics. 2014;39(9):591-592.




