
Author: Kristine Jeffers, MD (Emergency Medicine Resident at San Antonio Military Medical Center) // Edited by: Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UT Southwestern Medical Center / Parkland Memorial Hospital) and Brit Long, MD (@long_brit)
 Eero Mäntyranta, born in 1937, was one of Finland’s most successful Olympic skiers. He competed in 4 Olympic Games between 1960 and 1972 and won a total of 7 medals, three of which were gold. Part of Mäntyranta’s success came from winning the genetic lottery in endurance sports. He had primary familial and congenital polycythemia which caused an increase in the number of red blood cells, red blood cell mass, and ultimately his oxygen carrying capacity.1
Eero Mäntyranta, born in 1937, was one of Finland’s most successful Olympic skiers. He competed in 4 Olympic Games between 1960 and 1972 and won a total of 7 medals, three of which were gold. Part of Mäntyranta’s success came from winning the genetic lottery in endurance sports. He had primary familial and congenital polycythemia which caused an increase in the number of red blood cells, red blood cell mass, and ultimately his oxygen carrying capacity.1
Erythrocytosis, also known as polycythemia, refers to an increase in red blood cell mass. It can be relative or absolute. In relative polycythemia there is a decrease in plasma volume making it appear that there is an increase in red blood cells. There are three categories of absolute polycythemia.2,3
-Primary Polycythemia: Occurs when there is an inherited or acquired mutation in erythroid progenitors that lead to proliferation. This can be seen in polycythemia vera (PV), a myeloproliferative disorder, or in rare polycythemias that lead to an activation of the erythropoietin (EPO) receptor like in primary familial and congenital polycythemia as in the case of Mäntyranta.2,4
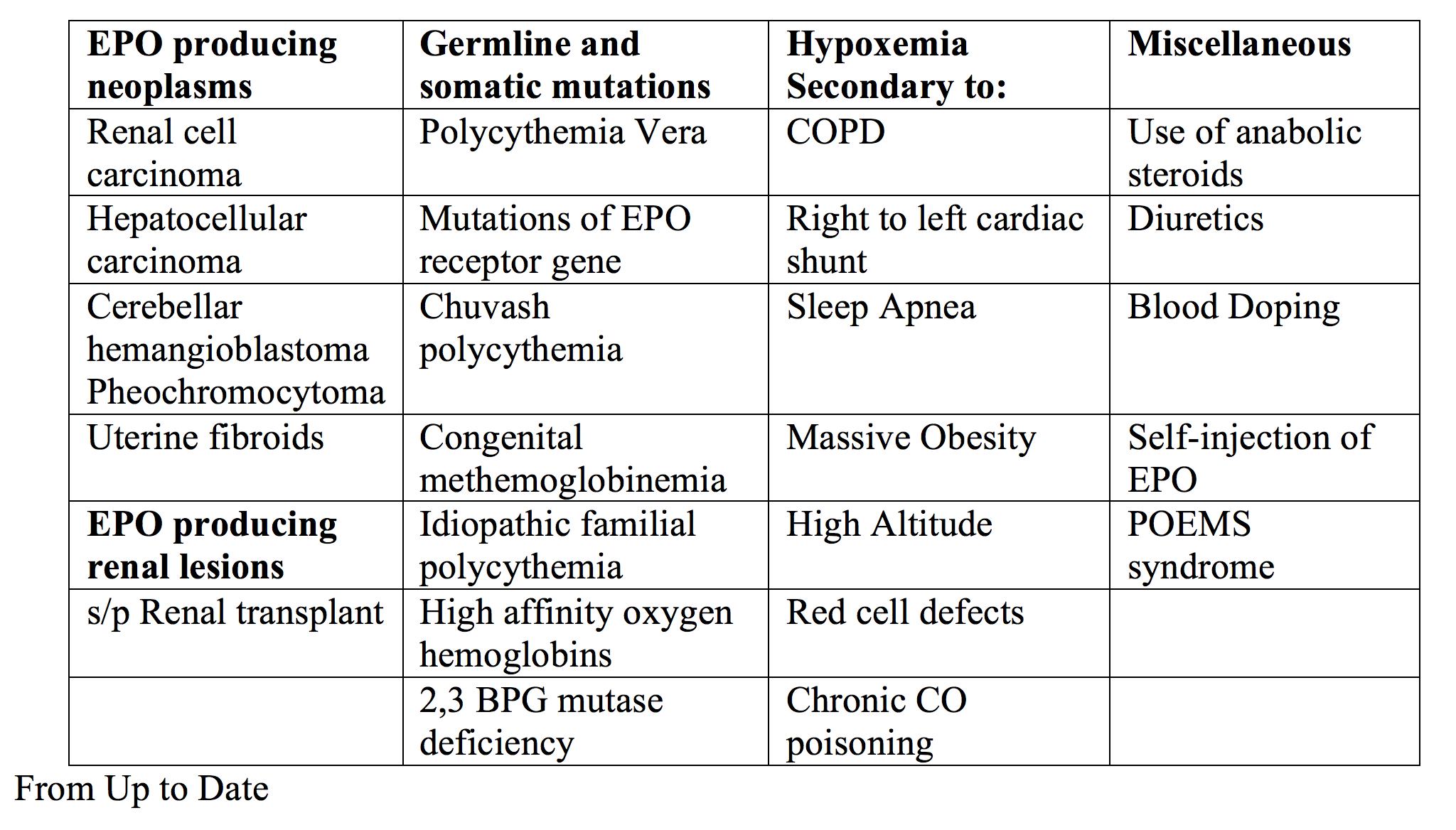
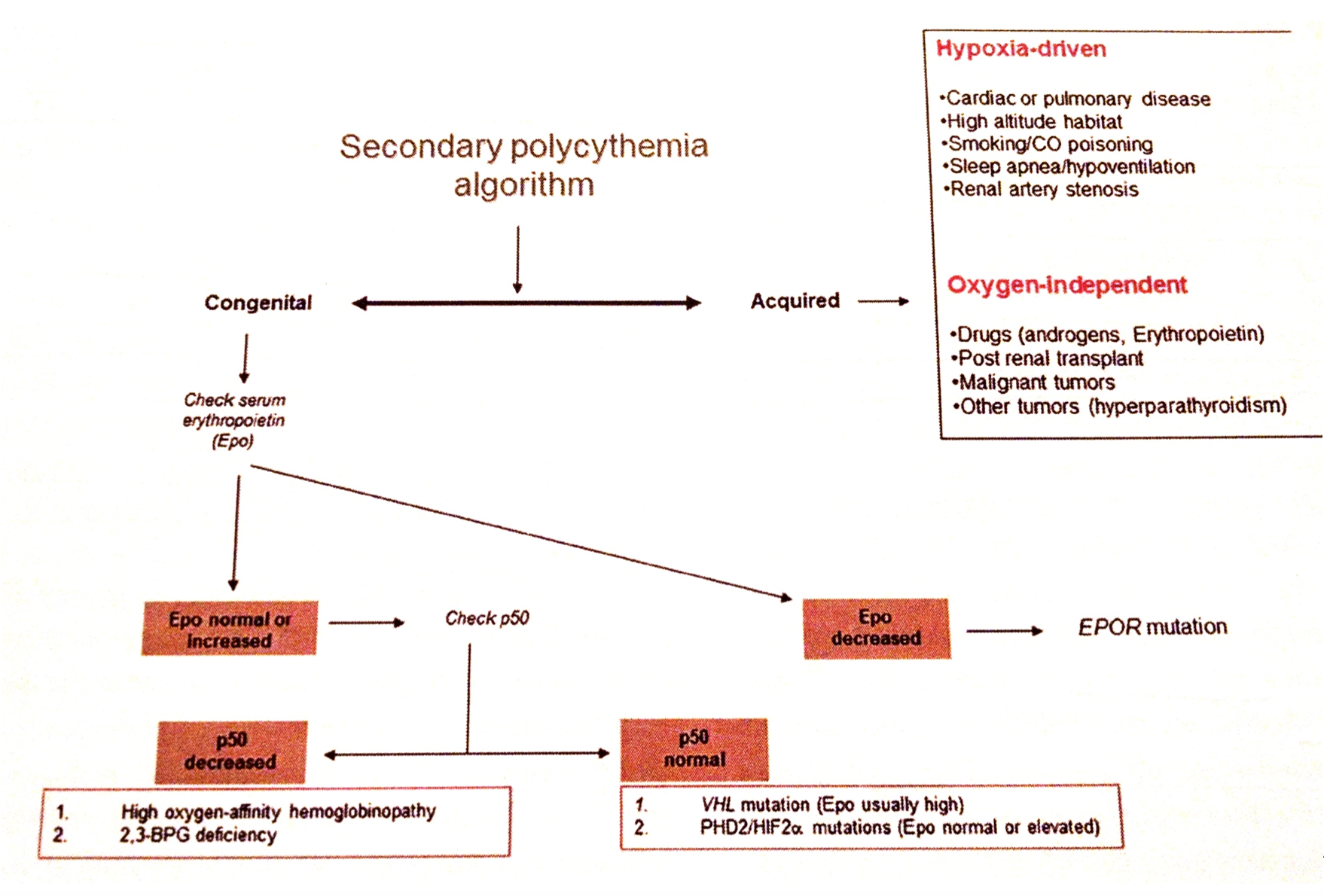
-Secondary Polycythemia: Occurs when there are increased levels of EPO circulating that stimulate erythroid progenitors. This can further be divided into two groups.
-Compensatory: This occurs when hypoxia stimulates EPO production and therefore red blood cell production. Many conditions and diseases contribute like pulmonary disease (COPD, OSA), cyanotic heart lesions, altitude, and carbon monoxide poisoning to name a few.
– Paraneoplastic: This occurs when EPO or an EPO like substance is produced by some other process. Most commonly this is the result of a malignancy (like renal cell carcinoma).2,3
-Disorders of hypoxia sensing: As the name states, this type of polycythemia results when there is a problem with hypoxia sensing that leads to increase red blood cells. It can have characteristics of both primary (increased sensitivity to EPO) and secondary polycythemia (increased EPO levels). These include Chuvash polycythemia and von Hippel Lindau gene mutations.4
Initial Evaluation of polycythemia
The initial evaluation of a patient presenting with polycythemia focuses on identifying the cause and determining whether the patient has primary or secondary polycythemia. Polycythemia should be considered in patients presenting with symptoms and evidence of erythrocytosis on laboratory evaluation.
History:
-On of the most common causes of polycythemia identified on history is hypoxia secondary to lung disease.
-History of travel to altitude for extended periods of time, cardiac defects, renal transplant, and use of O2 at home or smoking should also be elicited.
-Common presenting symptoms include chest and abdominal pain, myalgias, weakness, fatigue, headache, and slowed mentation.5 Patients may also present with pulmonary complaints to include shortness of breath, chronic cough, or hypersomnolence.
-Symptoms that are more predictive of PV include pruritus after bathing, erythromelalgia, gout, arterial and venous thrombosis, hemorrhage, and early satiety from splenomegaly. 2
Physical Exam:
-Vital signs including pulse ox, signs of cyanosis in lips, fingers, clubbing, murmur, or bruits. Patients may also have plethoric facies or hepatosplenomegaly.2
Laboratory Evaluation:
-CBC with indices.
-UA- looking for microscopic hematuria, which could be seen in setting of renal cell carcinoma.
-LFTs to evaluate for hepatocellular carcinoma, cirrhosis, hepatitis, or hemochromatosis.
-Consider CO test for CO poisoning.
-Chest X-ray looking for causes of erythrocytosis (COPD, pulmonary hypertension, AV malformations).
Other testing (not required in the ED):
-Serum EPO- low is relatively specific for diagnosis of PV but may also be seen in blood doping.
– If elevated, erythrocytosis is likely secondary.
-JAK2 mutation testing.
-Bone Marrow aspiration/biopsy.2
Treatment:
Treatment of secondary polycythemia is twofold. Primarily the underlying cause should be removed if possible (excision of tumor, stopping steroids, removing CO exposure, etc.). If removing the cause is not possible or is ineffective, limited phlebotomy is done for symptom relief. Treatment of polycythemia vera (the most common cause of primary erythrocytosis) is discussed below.6
Polycythemia Vera
Polycythemia vera affects an estimated 100,000 people in the United States, and those affected have an increased mortality most often from complications related to thromboembolic or hemorrhagic events. Risk factors include age >60 years, history of thrombosis, and hematocrit >45%.5-7
Pathogenesis: PV develops from a point mutation in the JAK-2 leading to tyrosine kinase activation. The mutated tyrosine kinase leads to growth factor independent proliferation of red blood cells.2,3
Diagnostic Criteria: The WHO diagnostic criteria for PV include three major and one minor criterion. You may have all three major or the first two major and one minor criterion.
Major Criteria:
-Hemoglobin > 16.5 g/dL in men (> 16 g/dL in women) or hematocrit >49% in men (48% women) or red cell mass >25% above the mean.
-Bone marrow tri-lineage myeloproliferation with pleomorphic mature megakaryocytes.
– JAK2 mutation.
Minor Criteria:
-Subnormal serum erythropoietin level.2, 7
You should consider PV in patients presenting with the following symptoms and an elevated hemoglobin/hematocrit on lab analysis.
Common Symptoms: pruritus, headache, fatigue, difficulty thinking or sleeping, dizziness, hyperuricemia, and bleeding or thrombotic complications.
Treatment: All patients with PV are treated with phlebotomy to a hematocrit level of 45% (creates an iron deficient anemia) and low dose aspirin. Further pharmacological treatment is based on risk stratification and lack of symptom control with the above mentioned. Other options for cytoreductive therapy include:6-8
-Hydroxyurea: First line medication for cytoreductive therapy. About 25% of people will become resistant or intolerant during the course of treatment.
-Interferon alpha: Associated with clinical benefit and normalized blood counts. It may become toxic especially at high doses.
-Ruxolitinib: JAK1/JAK2 inhibitor approved by the FDA for use in patients with PV that have failed hydroxyurea and studies have shown it to be better than the best available treatments when it came onto the market.7

Hyperviscosity Syndrome:
Hyperviscosity syndrome presents with a triad of bleeding, visual disturbances, and focal neurologic signs and can be a complication of erythrocytosis.9 Bleeding is often seen from mucosal surfaces (epistaxis, gums, GI). Retinopathy is caused by thrombosis and microhemorrhages. Neurologic complications can include a wide range of symptoms from headache to stupor, vertigo, or coma.10 It should be considered in the emergency department in three settings: when the patient presents with the classic triad, critically ill patients with laboratory abnormalities that are indicative of hyperviscosity, and in patients with known hematologic disease and new decline. It occurs more frequently in diseases of hyperproteinemia but can also be seen in the setting of erythrocytosis.
Treatment resolves around early consultation to hematology and aggressive supportive resuscitation with hydration and avoidance of diuretics.9-11 Rapid reduction of offending agent is accomplished with plasmapheresis or plasma exchange. Definitive care is accomplished with chemotherapeutic management.
Summary:
–Consult hematology early for recommendations, further evaluation, and definitive treatment.
-Secondary erythrocytosis is from numerous causes; a good history and physical will discover most of them! EPO level may be helpful for differentiation.
-Treatment of secondary erythrocytosis includes removal of offending cause and possibly phlebotomy.
-Consider PV in setting of elevated hemoglobin/hematocrit + symptoms (pruritus, headache, fatigue, difficulty thinking or sleeping, dizziness, hyperuricemia, and bleeding or thrombotic complications) especially in persons >60 years old.
-Initial treatment of PV includes phlebotomy (consult your specialist) and low-dose aspirin.
-Hyperviscosity syndrome: triad of bleeding, visual disturbances, and focal neurologic signs. Mainstay of treatment is hydration and hematology consult.
References/Further Reading
- Eero Mantyranta. (2017, January 14). Retrieved May 03, 2017, from https://en.wikipedia.org/wiki/Eero_M%C3%A4ntyranta
- Tefferi, A. (2017, February 15). Diagnostic Approach to the patient with Polycythemia (S. Schrier, Ed.). Retrieved April 5, 2017, from https://www.uptodate.com/contents/diagnostic-approach-to-the-patient-with-polycythemia?source=search_result&search=polycythemia%20adult&selectedTitle=1~150
- Robbins, S. L., Cotran, R. S., & Kumar, V. (2010).Robbins and Cotran pathologic basis of disease (8th ed.). Philadelphia, PA: Saunders/Elsevier.
- Prchal, J. (2016, August 08). Molecular pathogenesis of congenital polycythemic disorders and polycythemia vera (S. Schrier, Ed.). Retrieved April 5, 2017, from https://www.uptodate.com/contents/molecular-pathogenesis-of-congenital-polycythemic-disorders-and-polycythemia-vera?source=machineLearning&search=primary%20familial%20and%20congenital%20polycythemia&selectedTitle=1~8§ionRank=1&anchor=H17#H17
- Wang, Eurnice; Berliner, Nancy. Clonal Disorders of the Hematopoietic Stem Cell. In: Cecil Essentials of Medicine, Eighth Edition. 2010: 507-508.
- Tefferi, A. (2016, July 11). Prognosis and treatment of polycythemia vera (S. Schrier, Ed.). Retrieved April 5, 2017, from https://www.uptodate.com/contents/prognosis-and-treatment-of-polycythemia-vera?source=search_result&search=polycythemia%20adult%20treatment&selectedTitle=1~150
- Tefferi, A., & Barbui, T. (2017). Polycythemia vera and essential thrombocythemia: 2017 update on diagnosis, risk-stratification, and management. American Journal of Hematology,95, 95-108.
- Gerds, A., & Dao, K. (2017). Polycythemia Vera Management and Challenges in the Community Health Setting.Oncology,92, 179-189.
- Meier, B., & Burton, J. (2014). Myeloproliferative Disorders. Emergency Medicine Clinical Journal of North America,32, 597-612.
- Adams, B., Baker, R., Lopez, A., & Spencer, S. (2009). Myeloproliferative Disorders and the Hyperviscosity Syndrome. Emergency Medicine Clinical of North America, 27, 459-476.
- Blackburn, Paul. Emergency complications of Malignancy. In: Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, Seventh Edition. 2011:1514.
- Hackett, Peter; Hargrove, Jenny. High-Altitude Medical Problems. In: Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, Seventh Edition. 2011:1409.




