
Author: Matthew Streitz, MD (EM Resident at SAUSHEC, USAF) // Edited by: Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UTSW / Parkland Memorial Hospital) and Brit Long, MD (@long_brit, EM Chief Resident at SAUSHEC, USAF)
How many reproductive-aged women with abdominal pain does the average emergency physician see in a shift in the emergency department? The etiology of pelvic and abdominal pain in any female patient from the age of 10 to 60 years is vast and overlapping. How do you as an ED physician decide what is at the top of the differential? Is it age, pain onset, description, or quality of pain? Is she pregnant? Does she have vaginal bleeding? What are the diagnoses that cannot be missed? Most if not all would agree that list encompasses ectopic pregnancy, tubo-ovarian abscess, acute abruption, appendicitis, and ovarian torsion, the topic of this pitfall and pearls post.
Introduction
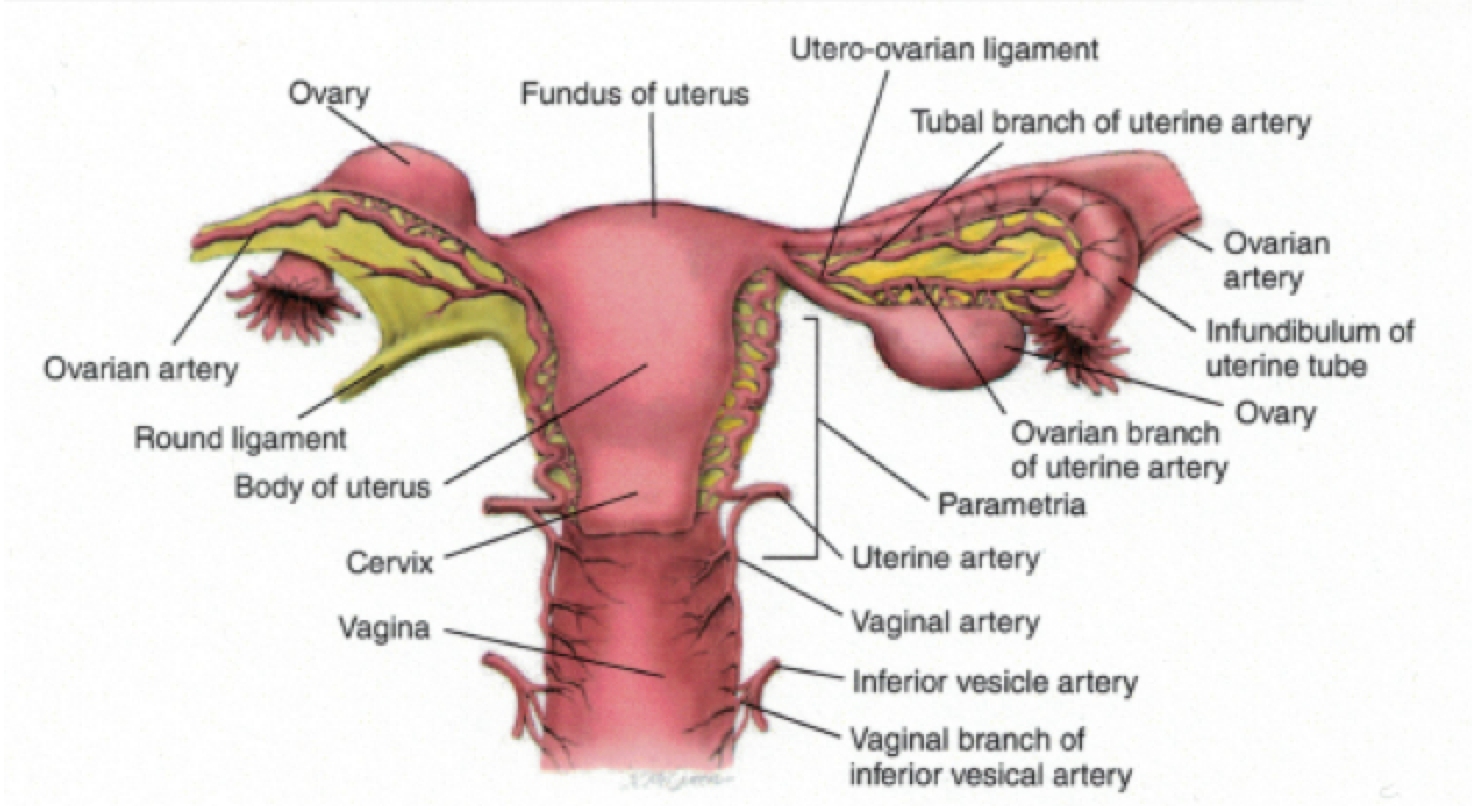
Ovarian torsion is one of the most common gynecologic emergencies encountered by Emergency Medicine physicians and remains a must not miss diagnosis. Ovarian torsion is the partial or complete rotation of the ovary on the ligamentous support (infundibulopelvic ligament and the utero-ovarian ligaments) within the abdomen, often critically limiting the blood supply to the ovary. [1] The goal of the ED physician is to diagnose torsion in a timely fashion in an attempt to preserve ovarian function and viability.
Pathogenesis
The mechanism of ovarian torsion involves the twisting of the ovary on its ligamentous support within which the blood supply rests. The ovary is suspended within the abdomen by the suspensory ligament of the ovary, also known as the infundibulopelvic ligament, which is not a fixed structure. The length of the ligament varies with age and gets shorter as women age. [2,3] The blood supply to the ovary is found within the ligaments and includes the tubal and ovarian branches of the uterine artery.
The most likely predisposing factor for torsion in an adult woman is an adnexal mass, either a physiologic cyst or a neoplasm. The presence of an ovarian mass increases the likelihood of torsion up to a certain size of the mass. Once a mass is large enough, the incidence of torsion actually will decrease due to decreased maneuverability and possibly secondary to adhesions as is the case with malignant masses within the ovaries. In addition the right ovary is more likely to develop ovarian torsion, possibly due to the presence of the sigmoid colon on the left side.
Normal ovaries are also at risk for torsion, which is more likely to occur with premenarchal females likely secondary to anatomy. The infundibulopelvic ligament is elongated early on and shortens with age and as girls progress through puberty. [2,3]
Once the ovary has torsed the blood supply can be diminished. The likely sequence of events is due to anatomical function and development with the venous supply, or the venous outflow limited secondary to the compressibility of veins. As time progresses and the venous congestion accumulates, the swelling and enlargement of the ovary leads to arterial compression and worsening of the condition and outcome. If allowed to progress to tissue necrosis, sepsis and peritonitis can develop. This is often very late in the course of events and is rare.
Comprehensive Gynecology, 5th Ed. Katz, et al.
Epidemiology
The true incidence of ovarian torsion is unknown. Ovarian torsion is described as the 5th leading cause of gynecologic emergencies and represents about 15% of surgically treated adnexal masses. [4] An adnexal mass, typically with a diameter of 5 cm or greater, is the greatest risk factor for torsion although in one case series the mass size associated with torsion ranged from 1 cm to 30 cm with an average size of 9.5 cm. In premenarchal females, a case series reported over 50% of girls with torsion had normal anatomy (i.e. no mass). [4,5,6,7,8,9] Ovarian torsion can also occur in the pregnant female, with the greatest incidence between 10 and 17 weeks although possible in all three trimesters. In pregnancy the masses most likely to torse were 6 to 8 cm, with larger masses less likely to develop torsion. [7,8,9,10]
Another important population to consider the diagnosis of ovarian torsion is the patient undergoing reproductive and infertility evaluations and using ovulation induction agents. These patients are at risk for ovarian hyperstimulation syndrome, and in one case series, 8% of patients developed torsion from physiologic cysts. [11]
Other risk factors include polycystic ovarian syndrome and tubal ligation, possibly secondary to adhesions. As with any condition or disease process those with prior history are at risk for repeat occurrence. In patients with prior ovarian torsion, 11% were likely to recur, and of those, women with normal anatomy are at greater risk. [5,6]
Clinical Presentation
The classic presentation of ovarian torsion includes acute onset of moderate to severe pain with nausea and vomiting in a patient with a prior history of an adnexal mass. Nausea typically occurs at the onset of pain. Fever and chills can occur but are more likely to occur with premenarchal females since their course is typically slower at onset with later presentation to the ED for care. They are more likely to present with fever and diffuse pain, rather than focused right or left lower quadrant pain.
The most common presenting symptom is pelvic pain followed by the history of or a palpable adnexal mass on physical exam. Patients typically present 1 to 3 days after onset, although patients with intermittent torsion can present at any time. Abdominal pain can be characterized as sharp, stabbing, and colicky, and it can possibly radiate to the flank, back, or into the pelvis and upper thigh. [5,12,13]
Evaluation in the ED – History and Physical
As with the vast majority of patient encounters, the history and physical can yield significant value to the ED physician. Important questions regarding medical history include the presence of adnexal mass, gynecologic or obstetric diseases, pregnancy, ongoing infertility treatment, and prior adnexal mass. Was there a history of recent vigorous activity, which can be seen at the onset of ovarian torsion?
Physical examination should include vital signs, which can show tachycardia, hypertension, hypotension, or even fever. Abdominal and pelvic examination (speculum and bimanual) should be performed on all sexually active females and in some cases of virginal patients. In cases of adolescent females, care should be taken to fully explain the exam to alleviate concerns and to fully explain the rationale and importance of the exam in helping with the diagnosis of torsion and other etiologies of pelvic and abdominal pain. Consent should be obtained as necessary.
Laboratory and Radiologic Imaging
Laboratory testing is not especially helpful except in determining if the patient is pregnant. Hemoglobin, white blood cell count, urinalysis, type and screen, and tests for sexually transmitted infections are all common tests that are collected during an evaluation of women with abdominal and pelvic pain where torsion is a leading diagnosis.
The preferred modality of imaging in the female with pelvic and abdominal pain is ultrasound with the use of Doppler flow studies to aid in the diagnosis of ovarian torsion. Ultrasound is also helpful in ruling out other causes of pain such as tubo-ovarian abscess, appendicitis, and ectopic pregnancy. [14,15,17]
Sonographic findings associated with ovarian torsion include a rounded and enlarged ovary on the ipsilateral side with pain. Ovarian mass, heterogeneous stroma of the ovary on the side of pain as well as an abnormal location of the ovary can all be seen in ovarian torsion. [17] Ovaries with torsion can frequently be anterior to the uterus. Decreased or absent Doppler flow is also seen with ovarian torsion, and the finding of decreased flow in the setting of pelvic pain and adnexal mass is 100% sensitive and 97% specific for torsion. [16,17]
CT and MRI are helpful for determining other causes of pelvic and abdominal pain and may show signs consistent with ovarian torsion, which include an enlarged and edematous ovary, abnormal location of an ovary, pelvic free fluid, and lack of IV contrast enhancement due to the occlusion of ovarian vessels. [18]
Diagnosis of Ovarian Torsion
A definitive diagnosis of ovarian torsion is made upon direct visualization of a rotated ovary during surgical evaluation. In a patient with an adnexal mass, acute pelvic pain, and ultrasound findings consistent with torsion, the diagnosis can be presumed. If the patient underwent CT instead, the findings discussed above with a good history for torsion warrant further evaluation by Gynecology. It is important to note that the absence of an adnexal mass does not exclude torsion. All patients with pelvic pain where ovarian torsion is high on the differential should have a Gynecologic consultation and evaluation in the Emergency Department, despite what the ultrasound demonstrates.
Differential Diagnosis
In women with acute pelvic and lower abdominal pain, ectopic pregnancy, ruptured ovarian cyst, and tubo-ovarian abscess should be on the differential when a mass is present. The most important aspect of differentiating conditions includes the pregnancy test, so this should be one of the first laboratory tests obtained. This greatly changes the differential diagnosis. It is important to keep your differential broad and to include gynecologic as well as gastrointestinal causes of pain while simultaneously ruling out all of the life threats.
Management
The management of ovarian torsion is to mitigate the effects of the decreased blood flow to the ovary with reversal of the torsion. Preservation of ovarian function and the prevention of complications including sepsis, peritonitis, and the possibility of infertility secondary to adhesions and scarring are the main goals of management. Management of fluid and electrolyte abnormalities should be addressed immediately; antibiotics in the setting of sepsis should cover anaerobes and aerobes. Adequate treatment would include broad-spectrum antibiotics, and the patient should be typed and screened or cross-matched for blood depending on the presence of hemodynamic instability and hemoglobin levels. Ultimately surgical correction is the definitive treatment, with early surgical consultation.
References / Further Reading
- McWilliams GD, Hill MJ, Dietrich CS 3rd. Gynecologic emergencies. Surg Clin North Am 2008; 88:265.
- Germain M, Rarick T, Robins E. Management of intermittent ovarian torsion by laparoscopic oophoropexy. Obstet Gynecol 1996; 88:715.
- Buss JG, Lee RA. Sequential torsion of the uterine adnexa. Mayo Clin Proc 1987; 62:623.
- Bouguizane S, Bibi H, Farhat Y, et al. [Adnexal torsion: a report of 135 cases]. J Gynecol Obstet Biol Reprod (Paris) 2003; 32:535.
- Houry D, Abbott JT. Ovarian torsion: a fifteen-year review. Ann Emerg Med 2001; 38:156.
- Tsafrir Z, Hasson J, Levin I, et al. Adnexal torsion: cystectomy and ovarian fixation are equally important in preventing recurrence. Eur J Obstet Gynecol Reprod Biol 2012; 162:203.
- Anders JF, Powell EC. Urgency of evaluation and outcome of acute ovarian torsion in pediatric patients. Arch Pediatr Adolesc Med 2005; 159:532.
- Tsafrir Z, Azem F, Hasson J, et al. Risk factors, symptoms, and treatment of ovarian torsion in children: the twelve-year experience of one center. J Minim Invasive Gynecol 2012; 19:29.
- Worthington-Kirsch RL, Raptopoulos V, Cohen IT. Sequential bilateral torsion of normal ovaries in a child. J Ultrasound Med 1986; 5:663.
- Schmeler KM, Mayo-Smith WW, Peipert JF, et al. Adnexal masses in pregnancy: surgery compared with observation. Obstet Gynecol 2005; 105:1098.
- Gorkemli H, Camus, M, Clasen K. Adnexal Torsion after gonadotropin ovulation induction for IVF or ICSI and its conservative treatment. Arch Gynecol Obstet 2002; 267:4.
- Huchon C, Panel P, Kayem G, et al. Does this woman have adnexal torsion? Hum Reprod 2012; 27:2359.
- Ashwal E, Hiersch L, Krissi H, et al. Characteristics and Management of Ovarian Torsion in Premenarchal Compared With Postmenarchal Patients. Obstet Gynecol 2015; 126:514.
- Anthony EY, Caserta MP, Singh J, Chen MY. Adnexal masses in female pediatric patients. AJR Am J Roentgenol 2012; 198:W426.
- Wilkinson C, Sanderson A. Adnexal torsion — a multimodality imaging review. Clin Radiol 2012; 67:476.
- Nizar K, Deutsch M, Filmer S, et al. Doppler studies of the ovarian venous blood flow in the diagnosis of adnexal torsion. J Clin Ultrasound 2009; 37:436.
- Mashiach R, Melamed N, Gilad N, et al. Sonographic diagnosis of ovarian torsion: accuracy and predictive factors. J Ultrasound Med 2011; 30:1205.
- Haque TL, Togashi K, Kobayashi H, et al. Adnexal torsion: MR imaging findings of viable ovary. Eur Radiol 2000; 10:1954.
- http://www.ncbi.nlm.nih.gov/pubmed/23810116
- http://www.ncbi.nlm.nih.gov/pubmed/23558274





4 thoughts on “Ovarian Torsion: Pearls and Pitfalls”
Pingback: Global Intensive Care | Ovarian Torsion: Pearls and Pitfalls
Great article!
Just a clarification regarding the following statement: “Decreased or absent Doppler flow is also seen with ovarian torsion, and the finding of decreased flow in the setting of pelvic pain and adnexal mass is 100% sensitive and 97% specific for torsion.”
In the study cited by Nizar et al., in their study population of 199 patients, they give the following Sensitivity and Specificity for these ultrasound findings for the diagnosis of ovarian torsion:
Tissue edema: 21% and 100%
Absence of intra-ovarian vascularity: 52% and 91%
Absence of arterial flow: 76% and 99%
Absence or abnormal VENOUS flow: 100% and 97%
This means that, yes, decreased arterial or venous flow are highly SPECIFIC, meaning good for ruling IN torsion. Abnormal venous flow is very SENSITIVE, meaning good for ruling OUT torsion. However, absent ARTERIAL flow is poorly sensitive, only 76% in this study. This means you CAN NOT rule out torsion if you see normal arterial flow. There are many documented cases of patients with normal arterial blood flow who are found to have torsion in the OR. I think this is the major pitfall in the diagnosis of torsion: reliance on the ultrasound finding of decreased ARTERIAL blood flow to the ovary. If unsure, consider OB consult and admit for serial exams and serial ultrasound and possibly exploratory laparotomy if not improving. 🙂
Great article!
Just a clarification regarding the following statement: “Decreased or absent Doppler flow is also seen with ovarian torsion, and the finding of decreased flow in the setting of pelvic pain and adnexal mass is 100% sensitive and 97% specific for torsion.”
In the study cited by Nizar et al., in their study population of 199 patients, they give the following Sensitivity and Specificity for these ultrasound findings for the diagnosis of ovarian torsion:
Tissue edema: 21% and 100%
Absence of intra-ovarian vascularity: 52% and 91%
Absence of arterial flow: 76% and 99%
Absence or abnormal VENOUS flow: 100% and 97%
This means that, yes, decreased arterial or venous flow are highly SPECIFIC, meaning good for ruling IN torsion. Abnormal venous flow is very SENSITIVE, meaning good for ruling OUT torsion. However, absent ARTERIAL flow is poorly sensitive, only 76% in this study. This means you CAN NOT rule out torsion if you see normal arterial flow. There are many documented cases of patients with normal arterial blood flow who are found to have torsion in the OR. I think this is the major pitfall in the diagnosis of torsion: reliance on the ultrasound finding of decreased ARTERIAL blood flow to the ovary. If unsure, consider OB consult and admit for serial exams and serial ultrasound and possibly exploratory laparotomy if not improving. 🙂
[…] Credit to : http://www.emdocs.net/ovarian-torsion-pearls-and-pitfalls/ […]