
Author: David Cisewski, MD (@PainProfiles – EM Resident Physician, Icahn School of Medicine at Mount Sinai) // Edited by: Manpreet Singh, MD (@MPrizzleER), Alex Koyfman, MD (@EMHighAK), and Brit Long, MD (@long_brit)
Welcome back to the Pain Profiles series from David Cisewski. Have you ever though of using subcutaneous opioids?

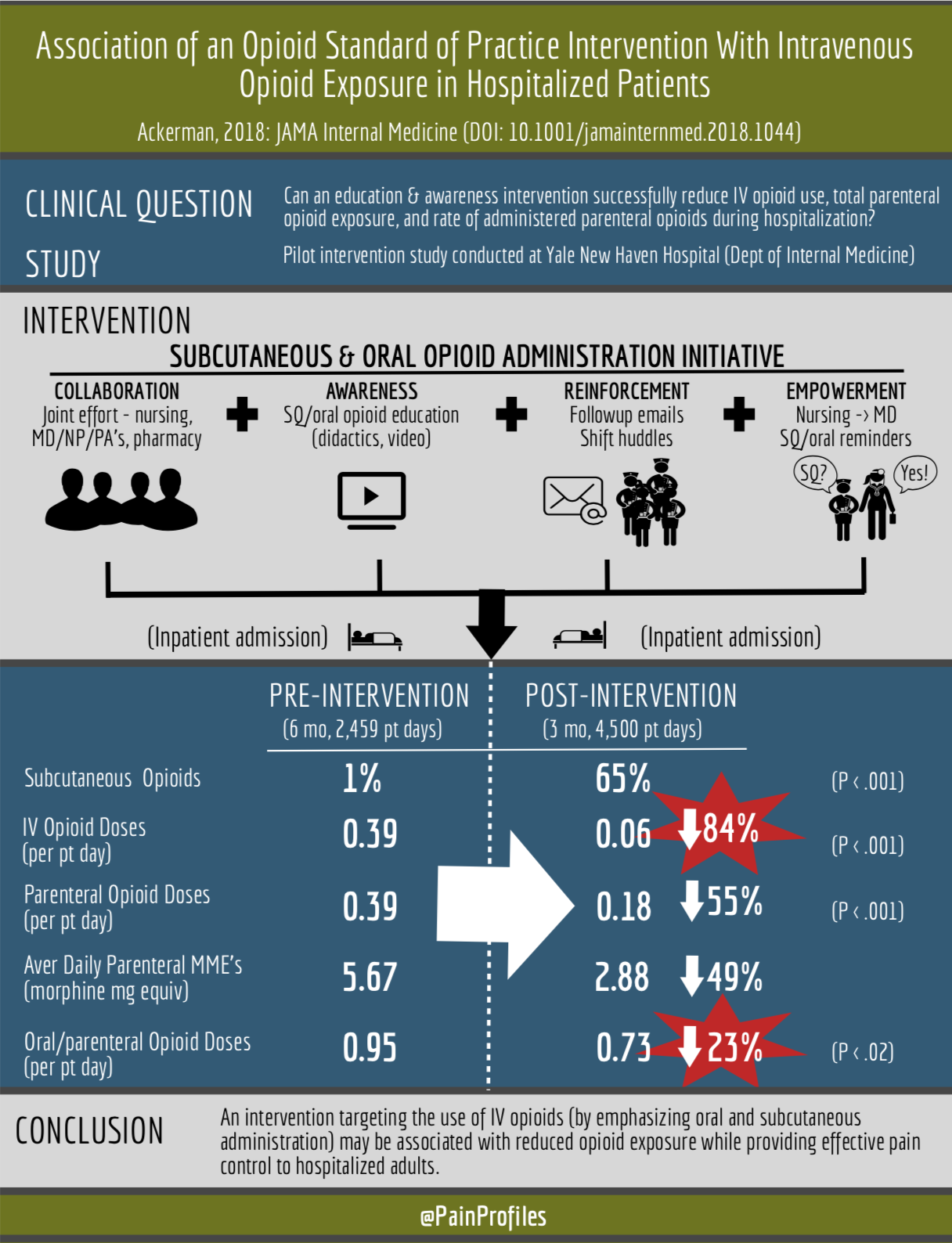
Ackerman, 2018: Association of an Opioid Standard of Practice Intervention With Intravenous Opioid Exposure in Hospitalized Patients (JAMA)
In the midst of our current opioid epidemic there is no shortage of headlines, research, white papers, and opinion pieces focusing on opioid-free analgesic modalities to ‘fight the crisis’. Ketamine? IV lidocaine? Nitrous oxide? Much of the analgesic research in 2018 focused on identifying an efficacious opioid alternative. Yet researchers out of Yale Hospital focused their clinical question not on what opioid alternative they could use to reduce opioid use, but whether a culture change focusing on alternative routes of administration could lessen overall consumption.
What did this study look at?
This was a pilot intervention study conducted at Yale New Haven Hospital (Dept of Internal Medicine). The authors attempted to identify whether the implementation of an education intervention and new hospital opioid standard of practice emphasizing the safety and efficacy of oral and subcutaneous opioid administration routes (over intravenous) would result in reduced (parenteral) opioid use compared to the traditional standard of practice.
Why is this important?
What we have been learning about opioid administration is that route matters in terms of safety, efficacy, and (possibly) addiction risk. Oral administration, for example, reduces the risk of nausea, hypotension, and euphoria compared to IV routes – much of which may contribute to addiction risk (as seen in animal models) (1). These authors sought to determine whether adopting a new standard of opioid therapy practice (oral and subcutaneous rather than IV) would result in reduced IV opioid exposure during inpatient admission and thus increase overall patient safety.
Who uses subcutaneous opioids?
Subcutaneous administration is an under-utilized method that has been used for decades (2). Although traditionally used for patients unable to tolerate oral administration, poor oral absorption, inability to obtain IV access, or in terminal cancer (3), its use may be expanding. It has been argued that subcutaneous administration may reduce the risk of bloodstream infections, increase time-to-analgesia, and is a preferred route by patients over intramuscular injections (4). This study by Ackerman, et al sought to expand on previous research that demonstrated the efficacious use of subcutaneous opioids for cancer pain (5).
What was the intervention?
Education initiatives including a 30 minute didactic presentation followed by a Q&A session and a follow-up email (at 2 and 4 weeks) to reinforce the new standard were provided to the 165-member hospital team (inpatient medical unit). Daily nursing huddles were also encouraged, as well as empowerment of nursing staff to remind prescribers of the new standard.
What were the results?
Opioid use among a 6-month pre-intervention group consisting of 127 admitted patients (2,459 patient-days) post-intervention were compared to a 3-month post-intervention group consisting of 287 admitted patients (4,500 patient days). Subcutaneous administration of parenteral opioids was utilized 1% pre-intervention vs 65% post-intervention. An 84% reduction in IV opioid use (primary outcome) was seen post-intervention (0.06 vs 0.39 doses per patient-day, P < .001). A 55% reduction in total parenteral opioid use (0.18 vs 0.39 doses per patient-day, P < .001), a 49% reduction in mean daily parenteral opioid exposure (2.88 [0.72] vs 5.67 [1.14] morphine-milligram equivalents [MMEs] per patient-day), and a 23% reduction in doses of opioid given either parenteral or oral (0.73 vs 0.95 doses per patient-day, P = .02) were also found. Mean pain scores were the same before and after new standard intervention.
Subcutaneous analgesia works and can be used in a 1:1 subcutaneous: intravenous conversion (listen to author interview below for more details). It was hypothesized that the pain reduction in the intervention group may have been improved by decreasing analgesic spikes associated with IV administration, offering more long-term, consistent pain control of oral and subcutaneous administration. The study also emphasizes the power of establishing a team-based interdisciplinary care team (nurses, pharmacy, ED, inpatient teams) in order to implement hospital culture change and targeted education strategies in implementing safe opioid utilization practices. Does this replace IV analgesics in the ED? No. Is this even ready for primetime in the ED? Still too soon to tell. Ultimately, severe pain presentations (eg, trauma, sickle cell crises) will still benefit from the quick-onset of IV opioid administration. But when possible, we should consider initiating subcutaneous and oral opioid analgesics in the ED (particularly during admissions) and encourage our inpatient colleagues to do the same.
Further Reading:
- Excellent interview with Dr. Ackerman (first author) and ZDoggMD (December, 2018) – CAN SUBCUTANEOUS NARCOTICS SOLVE THE OPIOID CRISIS?
- Yale News: Less is more when it comes to Rx opioids for hospital patients, study finds
- ACP Hospitalist: Shifting opioids from IV to subcu
References:
[1] Allain F, Minogianis EA, Roberts DC, Samaha AN. How fast and how often: The pharmacokinetics of drug use are decisive in addiction. Neurosci Biobehav Rev. 2015;56:166-79.
[2] Smith RF, Voss T, Klineberg P. Subcutaneous morphine. Anaesth Intensive Care. 1989;17:511-3.
[3] Campbell CF, Mason JB, Weiler JM. Continuous subcutaneous infusion of morphine for the pain of terminal malignancy. Ann Intern Med. 1983;98:51-2.
[4] Stoner KL, Harder H, Fallowfield LJ, Jenkins VA. Intravenous versus Subcutaneous Drug Administration. Which Do Patients Prefer? A Systematic Review. Patient. 2014.
[5] Radbruch L, Trottenberg P, Elsner F, Kaasa S, Caraceni A. Systematic review of the role of alternative application routes for opioid treatment for moderate to severe cancer pain: an EPCRC opioid guidelines project. Palliat Med. 2011;25:578-96.




