Authors: Rachel Lynn Graves, MD (EM Resident Physician, University of Pennsylvania) and Kevin R. Scott, MD, MSEd (EM Assistant program director, Attending physician, University of Pennsylvania) // Reviewed by: Skyler Lentz, MD (@skylerlentz); Alex Koyfman, MD (@EMHighAK); and Brit Long, MD (@long_brit)
Case
A 62-year-old male with a past medical history of hypertension, hyperlipidemia, insulin-dependent diabetes mellitus, morbid obesity, obstructive sleep apnea, depression, and spastic quadriplegia due to a remote diving accident with resultant C7 spinal cord injury presents with chills, nausea, and headache. He has had three days of generalized weakness, fatigue, and poor appetite. Over the past day, he has also developed diaphoresis and lightheadedness. He denies abdominal pain and has been straight catheterizing at home without difficulty. Two weeks ago, he completed a 10-day course of Keflex for a community-acquired urinary tract infection. On exam, the patient is a pleasant, well-groomed, tired-appearing, male seated in a wheelchair. He has a temperature of 100.9F, blood pressure of 168/95, and a heart rate of 58. He has spastic quadriplegia with limited residual strength in the upper extremities and symmetric, bilateral lower extremity edema to the mid-calf. His abdomen is soft, non-tender, and non-distended.
What management steps should you take immediately? What disease processes should be included in your differential?
Spinal cord injury (SCI) is a common event with an incidence of traumatic SCI in the United States of approximately 54 per million persons per year.[1] Traumatic SCI primarily affects young adults under 40 years of age. The leading causes of traumatic SCI include motor vehicle collisions (40-50%), falls (20%), and violence (14%).[2] Alcohol plays a role in 25% of all SCI.[3] Patients with injuries below T1 are likely to retain independent function, while injury above C6 requires almost complete dependency.[4] The prospects for recovery from an acute SCI diminish after about six months, and there are currently no effective means to promote repair of injured spinal cord tissue.[5] SCI produces a wide variety of changes in systemic physiology that can lead to numerous complications that significantly impact quality of life and functional status.[6-8] As an emergency medicine physician, it is imperative to be able to anticipate, understand, recognize and treat common conditions that bring patients with SCI to the emergency department.
Evaluation
Traumatic SCI has widespread physiological effects beyond the disruption of sensory and motor function. Spinal cord lesions from any cause can result in focal autonomic deficits or autonomic hyperreflexia affecting bowel, bladder, sexual, temperature-regulation, and cardiovascular functions.[9] The specific pattern of physiologic disturbance depends on the location and severity of the injury (i.e. whether the injury is complete or incomplete). For example, patients with cervical and high thoracic SCIs are at increased risk for pulmonary infections due to impaired ability to mobilize respiratory muscles, while patients with injuries below this level are relatively spared this particular complication. Other issues, such as abnormal sexual, genitourinary, and bowel dysfunction are more ubiquitous among patients with SCI.
Changes in normal physiology among patients with SCI make the diagnosis of acute illness, including infection, more difficult. Perception of painful sensations arising from structures innervated below the level of spinal cord lesions is often blunted or absent. Dangerous increases or decreases in body temperature may result from an inability to sense heat or cold exposure or control peripheral vasoconstriction and sweating below the level of the spinal cord injury.[9] Unexplained fever, worsening spasticity, or deterioration in neurologic function should prompt a thorough search for infection, thrombophlebitis, or intraabdominal pathology.[5]
A thorough physical exam can help the emergency medicine physician to identify common illnesses in a timely fashion. Completely undressing and turning the patient is a critical component of the physical exam as it allows for complete examination of the skin.
Historical data is also especially useful and may affect management of patients with SCI. Prior culture data can inform the selection of antibiotics for acute infectious processes. Old notes may provide a baseline neurologic exam and baseline vital signs. Many acute illnesses in patients with SCI may manifest primarily as changes in neurologic exam (e.g. increased spasticity) or atypical vital sign abnormalities, as in the case of autonomic dysreflexia.
Diagnostic considerations and management
Infections/Sepsis
Individuals with SCI are at high risk for both community-acquired and healthcare-associated infections. Risk factors include frequent contact with the healthcare system and frequent and chronic use of invasive medical devices such as urinary and intravascular catheters.[10,11] Bloodstream infection, urinary tract infection, pneumonia, and skin and soft tissue infections are all common among patients with SCI. Pneumonia and bloodstream infections are the most common infectious causes of mortality in this population.[10] Diseases of the skin, including pressure ulcers, are the second most common etiology for rehospitalization among people with chronic SCI.[12]
Infections may be missed in patients SCI due to autonomic abnormalities resulting in atypical vital sign responses, altered sensory input, history of microbial colonization of chronic wounds, and chronic urinary tract infections. The SCI population is also particularly vulnerable to misdiagnosis and inadequate empiric therapy.[10] A thorough understanding of the underlying pathophysiology and chronic complications of SCI, a complete physical exam, and focused review of historical data are all crucial components in the identification and treatment of infection in patients with chronic SCI.
Urinary tract and catheter-related infections
The leading source of infection and cause for rehospitalization among people with traumatic SCI is disease of the genitourinary system, including urinary tract infections (UTIs).[6] UTIs represent the most frequent source of septicemia in SCI patients, which has a mortality rate of 15%.[8] Indwelling urinary catheters are almost always used in the acute phase of spinal cord injury, but are generally not recommended for long term use as they are one of the most prevalent risk factors for UTI in SCI patients.[12]
Bladder dysfunction, often referred to as neurogenic bladder, can result in a number of complications including infections, vesicoureteral reflux, renal failure, and renal calculi. As with other conditions, urinary complications may present atypically or be asymptomatic, even in ambulatory patients. Sensation of bladder fullness and motor control of bladder sphincter function are impaired in SCI which can result in a number of neuromuscular complications.
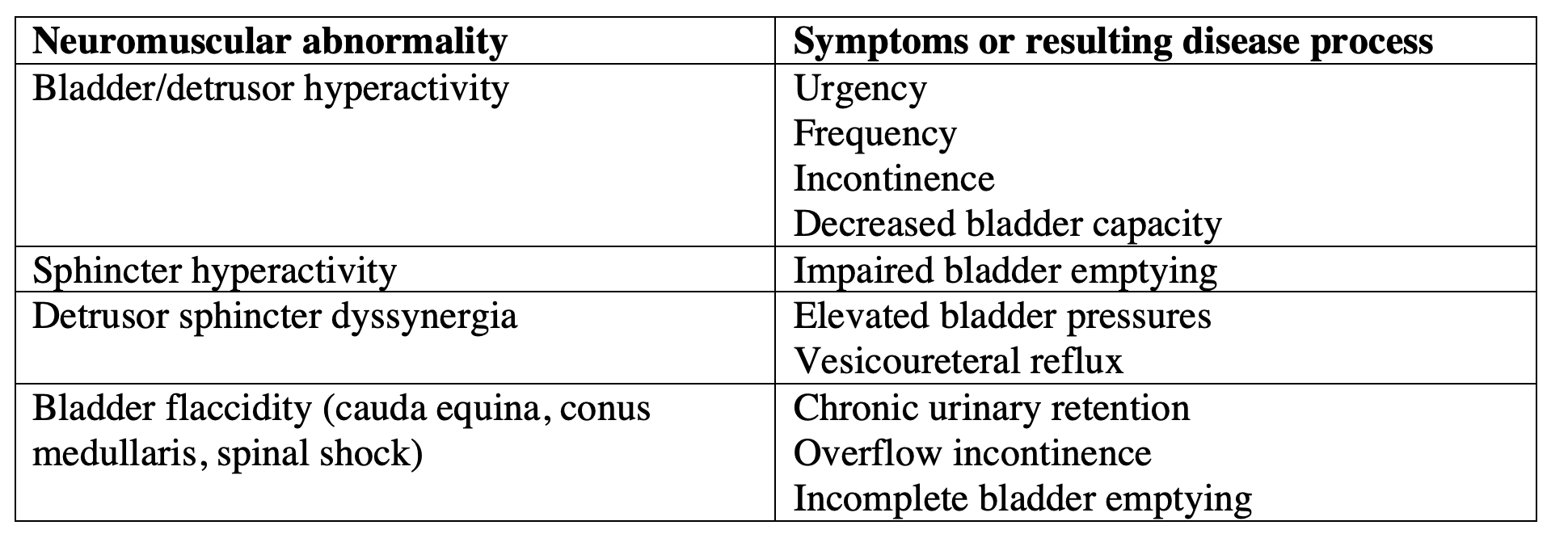
Most patients with neurogenic bladder are managed chronically with a combination of intermittent catherization and anticholinergic medications. Symptomatic UTIs should be treated early, and chronic bacterial colonization of the urinary tract is generally not treated at all.[1] Patients with neurogenic bladder, in particular those with indwelling Foley catheters, are often colonized with bacteria. Previous culture data from the patient’s medical chart can help distinguish between acute bacterial UTI and colonizing bacteria. Historical culture data also helps guide selection of antibiotics.
Skin/soft tissue infections and osteomyelitis
Pressure ulcers commonly develop on areas overlying bony prominences such as the sacral prominence and heels.[5] Shear forces, friction, poor nutrition, and changes in skin physiology below the level of the spinal cord lesion also contribute to the development of pressure ulcers.[1] Denervated skin is prone to the development of pressure necrosis.[13] Pressure ulcers have an estimated prevalence rate of 30 percent at 20 years following SCI.[14] Pressure ulcers are first colonized with skin flora, which is rapidly replaced by bacteria from the local environment and the urogenital or gastrointestinal tracts, often from direct contamination.[15] Almost all pressures ulcers are polymicrobial. Predominant organisms include Enterobacter species, staphylococci, streptococci, Proteus mirabilis, and anaerobes.[16]
The approach to evaluation and management of pressure ulcers depends on whether infection is superficial or deep.
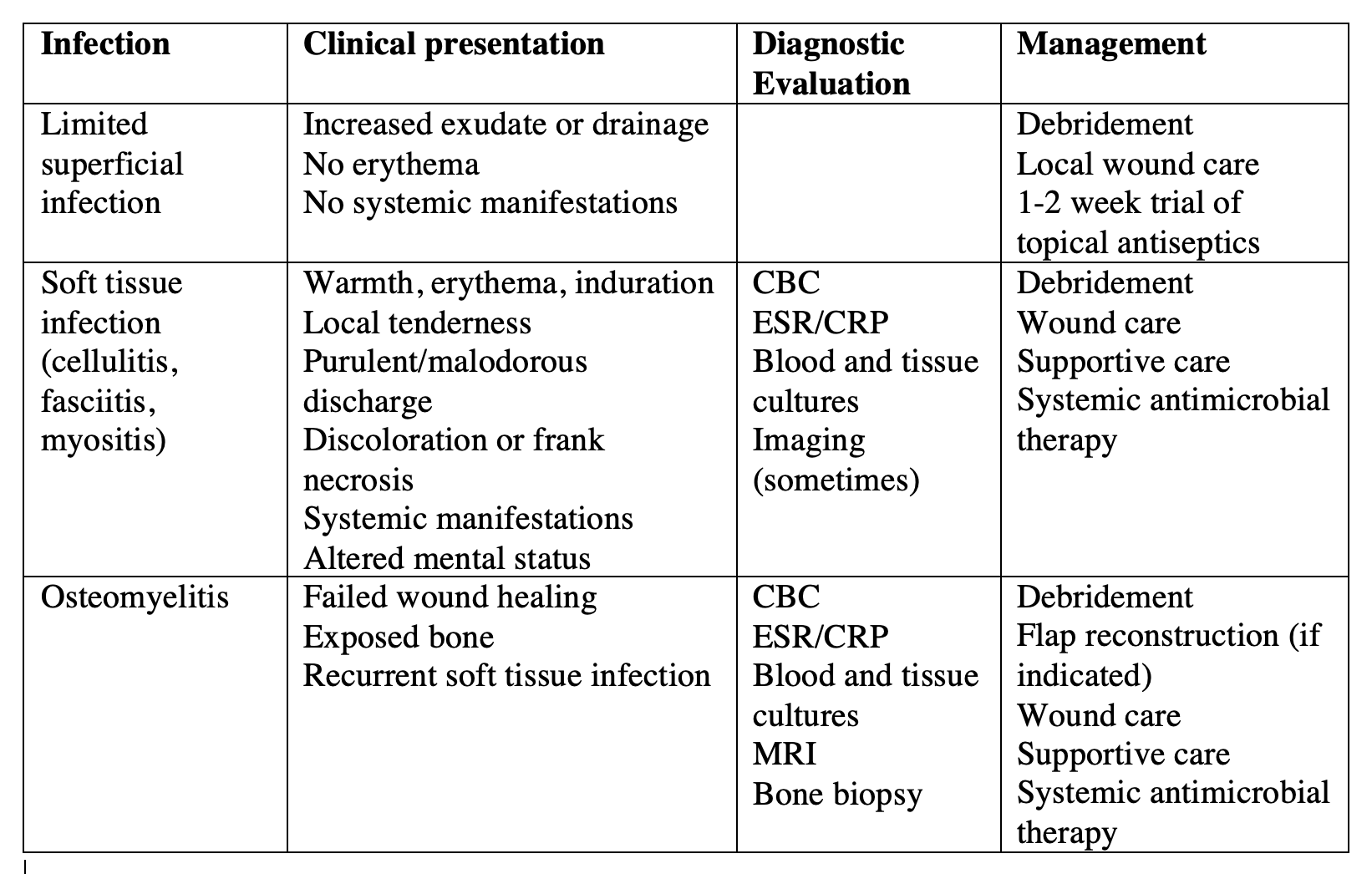
A higher index of suspicion is necessary in cases where the ulcer and surrounding tissue have not significantly worsened, but the patient has symptoms of systemic infection or sepsis. Microbiologic evaluation, including tissue and blood cultures, should be performed in these cases. The most useful specimen for culture is a biopsy of the deepest tissue involved in the ulcer, which can be obtained during debridement. Swab cultures reflect surface colonization rather than infection and are not recommended, though they are often obtained.[17]
Not all patients with skin/soft tissue infections need radiologic imaging, but it should be considered in patients with systemic manifestations of infection, positive blood cultures, indwelling medical devices (cardiac valves or implantable electronic cardiac devices, vascular grafts, prosthetic joints), and patients in whom osteomyelitis is suspected. MRI is the study of choice, but CT may be obtained if MRI is not feasible. Plain radiography has a limited role in the diagnosis and management of pressure-ulcer-associated osteomyelitis since bone changes due to osteomyelitis may be not distinguishable from those due to soft tissue infection alone.[17]
Systemic antimicrobial therapy should be initiated in all patients with soft tissue infections beyond the limited superficial infection. Selection of antibiotics should take into account local prevalence and resistance patterns, previous culture results and susceptibilities, risk factors for antibiotic-resistant organisms (residence in hospital, nursing home, or institutional setting), and whether or not pseudomonal coverage is needed. Selected antibiotics should provide MRSA, streptococcal, enteric gram-negative, and anaerobic coverage.[17]
Pulmonary infections
Patients with SCI are predisposed to pulmonary infection by virtue of their abnormal respiratory mechanics. Patients with cervical and high thoracic SCIs have respiratory muscle weakness, resulting in low tidal volume, high respiratory rate, dyspnea, exercise intolerance, and frank ventilatory failure.[18] These patients also have impaired cough and difficulty mobilizing lung secretions, which increases their risk for lower respiratory tract infections.[1,18,19,20] Pneumonias in SCI patients tend to be due to typical organisms associated with community-acquired pneumonia in the general population.[21]However, as with other infectious illnesses, the presentations are often atypical or more subtle, which can delay recognition.[10] As in the case of all infections, the emergency medicine physician should maintain a high degree of suspicion, and have a low threshold to obtain diagnostic imaging such as lung ultrasound or chest radiographs in patients with respiratory symptoms, vital sign changes, or an abnormal pulmonary exam.
Autonomic dysfunction
Patients with SCI often experience loss of normal autonomic and cardiovascular control. Injury at or above T6 segregates spinal sympathetic neurons from supraspinal modulation which can result in a syndrome known as autonomic dysreflexia (AD).[20,22] AD is an exaggerated sympathetic response which includes a rise in systolic blood pressure 20 mmHg above the patient’s baseline and is caused by noxious, often unperceived stimuli such as bladder distention, bowel impaction, pressure ulcers, ingrown toe nails, and occult visceral disturbances.[23] A concomitant parasympathetic response occurs which produces bradycardia and vasodilation above the level of the lesion.[1] Chronic AD occurs in at least a quarter of SCI patients with injuries at or above T5 and tends to be more common after more complete injuries.[24]
Clinical manifestations of AD include headache, diaphoresis, hypertension, flushing, piloerection, blurred vision, anxiety, and nausea. The severity of attacks ranges from asymptomatic hypertension to hypertensive crisis complicated by profound bradycardia, cardiac arrest, intracranial hemorrhage, and seizures.[1]
Initial management includes raising the head of the bed, removing all tight-fitting garments, and irrigating indwelling catheters to make sure there is no kink or obstruction. Consider bladder scanning to assess for urinary retention and perform a rectal exam to assess for impacted stool in the rectal vault if indicated.[25] Blood pressure should be assessed every five minutes. If blood pressure remains elevated, short-acting antihypertensives should be used as pharmacotherapy.[25]
Non-infectious pulmonary disease
The extent of respiratory complications from SCI depends on the level of SCI and the degree of motor impairment. In general, the higher the level of SCI, the more likely the patient is to have compromised respiratory physiology and require ventilatory support.[18] SCI often leads to respiratory dysfunction, including insufficiency of respiratory muscles, reduction in vital capacity, ineffective cough, reduction in lung and chest wall compliance, and excess oxygen cost of breathing.[26] As discussed above, pneumonia is a common complication of cervical and high thoracic SCI. Deep venous thrombosis (DVT) and pulmonary embolism (PE) are common early complications of SCI while pleural effusion, pneumothorax, and hemothorax are less common overall.[1,27]
Gastrointestinal disease
SCI at any level has the potential to impact the gastrointestinal (GI) tract. GI illness accounts for 10% of deaths following SCI and often present atypically.[19] Key symptoms include shoulder pain, nausea, anorexia, and changes in spasticity. Paralytic ileus, constipation, gastric atony, and upper GI bleeding are all common after SCI.[13,19] Peptic ulcer disease is particularly common in patients with cervical SCI.[3]
Neurogenic bowel affects nearly half of patients with SCI and is generally divided into two categories: upper motor neuron bowel syndrome and lower motor neuron bowel syndrome, corresponding to injuries above or at/below the conus medullaris respectively.[28] Injuries above the conus medullaris do not damage neural connections between the spinal cord and colon. The preserved neural connections can result in hyperreflexia of the pelvic muscles, which leads to constipation and fecal retention.[1,12] Bowel regimens and disimpaction are necessary in most of these patients to ensure at least biweekly evacuation and avoid colonic distention or obstruction.[5] Injuries below the conus medullaris damage neural connections between the spinal cord and colon, resulting in areflexic bowel. This may manifest as slowed transit, decreased sphincter tone, and frequent incontinence.[1,12]
Chronic pain and psychiatric co-morbidities
Despite the loss of sensory function, many patients with spinal cord injury experience chronic pain sufficient to diminish their quality of life.[5,12,29,30] Central sensitization to nociceptive input and enhanced sensory input caused by extensive alterations in primary sensory neurons likely both contribute mechanistically to chronic pain in these individuals.[31] The back, buttocks, hips, and lower extremities are commonly cited as sources of chronic pain among patients with SCI.[30]
Chronic pain can be divided into two major classes. The first in nociceptive pain, which is generated by direct stimulus of primary sensory neurons and occurs secondary to many sequelae of SCI that affect the musculoskeletal system, including overuse of the upper body, muscle weakness, poor posture, and spasticity. Nociceptive pain also includes pain generated in the skin and the viscera as well as headaches.[31] The second class of chronic pain is neuropathic pain, defined as pain caused by damage or disease of the nervous system. Unlike nociceptive pain, which can be protective, neuropathic pain is purely pathologic.[31] Neuropathic pain occurs in at least half of all SCI patients and is generally permanent and refractory to treatment.[32]
Chronic pain is directly related to co-morbid psychiatric disease among patients with SCI. Psychosocial complications associated with SCI include depression, suicide, substance use disorders, and divorce.[33] Between 20 and 45 percent of patients are depressed after traumatic SCI, and patient with SCI have a 4 to 5 times higher rate of suicide than age-matched population samples.[33,34] Although estimates of the prevalence of depression among patients with SCI vary widely, they are certainly greater than among the general population. Chronic pain and depression can compound physiological complications related to SCI. Emergency medicine physicians should inquire about these issues when patients present to the emergency room as part of their overall assessment and management.
Take Home Points
- As an emergency medicine physician, it is imperative to be able to anticipate, understand, recognize and treat common conditions that bring patients with SCI to the emergency department.
- Patients with chronic SCI often present atypically due to alterations in normal physiology.
- For all patients with SCI, complete a thorough physical exam, including disrobing and rolling the patient for a complete examination of the skin.
- The most common sources of infection among patients with chronic SCI are UTIs and skin/soft tissue infections; review historical data when possible to inform treatment decisions and antimicrobial selection.
- Chronic pain and psychiatric co-morbidities are common among patients with SCI. Perform screening for these issues as part of your overall assessment of the patient with chronic SCI.
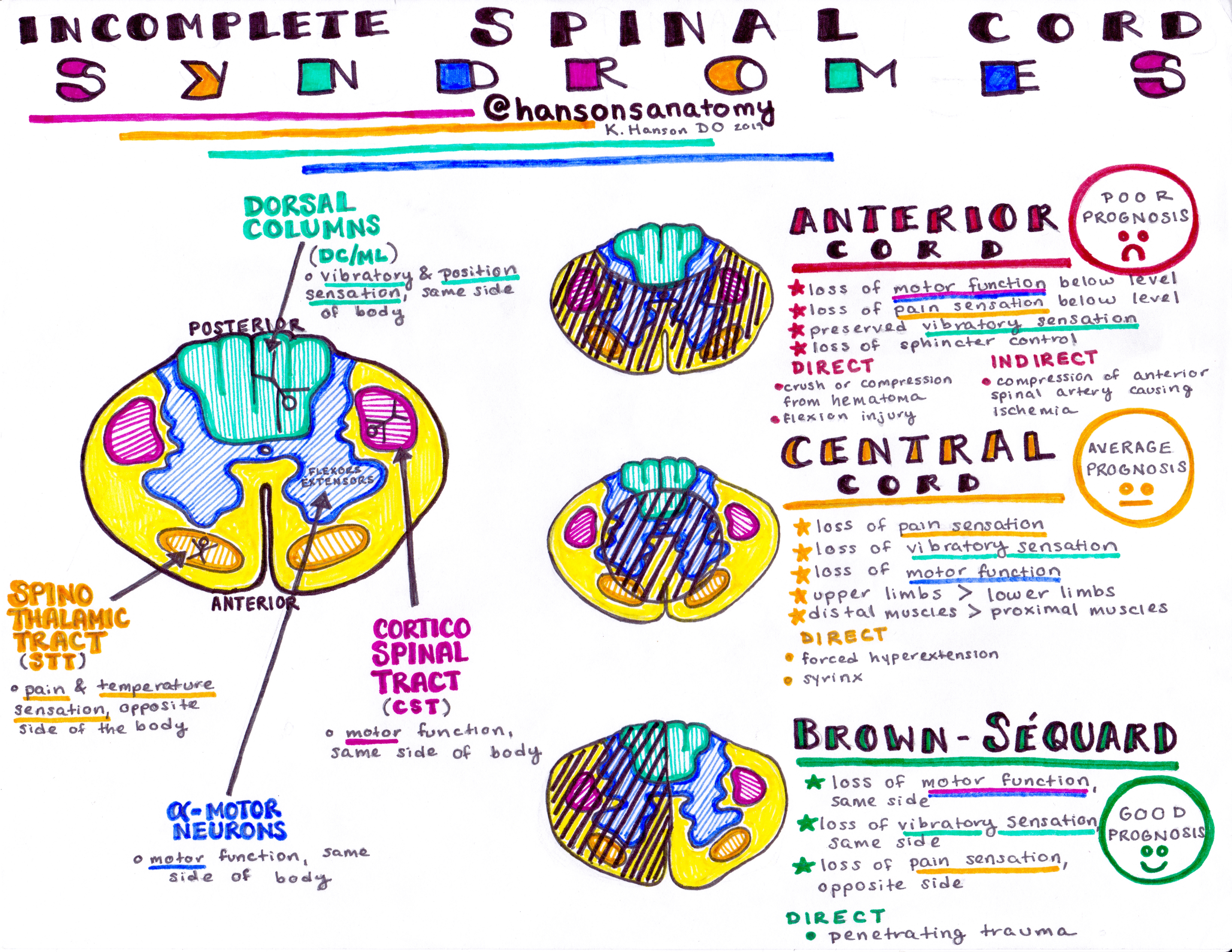
From Dr. Katy Hanson at Hanson’s Anatomy:
References
- Abrams GM, Wakasa M. Chronic Complications of Spinal Cord Injury and Disease. UpToDate. https://www.uptodate.com/contents/chronic-complications-of-spinal-cord-injury-and-disease?search=chronic%20spinal%20cord%20injury&source=search_result&selectedTitle=1~24&usage_type=default&display_rank=1#H10148218. Published August 19, 2019. Accessed June 14, 2020.
- Dhawan V, Ullman JS. Traumatic brain and spinal cord injury. In: Mitra R. eds. Critical Care. McGraw-Hill. Accessed July 03, 2020: https://accessmedicine-mhmedical-com.proxy.library.upenn.edu/content.aspx?sectionid=143519430&bookid=1944#143937301.
- Sweis R, Biller J. Systemic complications of spinal cord injury. Curr Neurol Neurosci Rep. 2017;17(8).
- Siroky MB. Pathogenesis of bacteriuria and infection in the spinal cord injured patient. Am J Med. 2002;113 Suppl 1A:67S.
- Hauser SL. Diseases of the spinal cord. In: Mitra R. eds. Harrison’s Principles of Internal Medicine, 20e. Accessed July 03, 2020: https://accessmedicine-mhmedical-com.proxy.library.upenn.edu/content.aspx?sectionid=192532889&bookid=2129#243600766
- Cardenas DD, Hoffman JM, Kirshblum S, McKinley W. Etiology and incidence of rehospitalization after traumatic spinal cord injury: A multicenter analysis. Arch Phys Med Rehabil. 2004;85:1757-63.
- Frankel HL, Coll JR, Charlifue SW, et al. Long-term survival in spinal cord injury: a fifty year investigation. Spinal Cord. 1998;36:255-274.
- Siroky MB. Pathogenesis of bacteriuria and infection in the spinal cord injured patient. Am J Med. 2002;113 Suppl 1A:67S.
- Gibbons CH, Engstrom JW. Disorders of the autonomic nervous system. In: Mitra R. eds. Harrison’s Principles of Internal Medicine, 20e. McGraw-Hill. Accessed July 03, 2020: https://accessmedicine-mhmedical-com.proxy.library.upenn.edu/content.aspx?sectionid=192532741&bookid=2129#196899597
- Garcia-Arguello LY, O’Horo JC, Farrell A et al. Infections in the spinal cord-injured population: a systematic review. Spinal Cord. 2016;55:526-534.
- Evans CT, LaVela SL, Weaver FM et al. Epidemiology of hospital-acquired infections in veterans with spinal cord injury and disorder. Infect Control Hosp Epidemiol. 2008;29:234-242.
- Sing R, Rohilla RK, Sangwan K, Siwach R et al. Bladder management methods and urological complications in spinal cord injury patients. Indian J Orthop. 2011;45:141-147.
- Stone C, Humphries RL. Eds. CURRENT Diagnosis & Treatment: Emergency Medicine, 8e. McGraw-Hill; Accessed July 03, 2020. https://accessmedicine-mhmedical-com.proxy.library.upenn.edu/content.aspx?bookid=2172§ionid=165055921
- McKinely WO, Jackson AB, Cardenas DD, DeVivo MJ. Long-term medical complications after traumatic spinal cord injury: a regional model systems analysis. Arch Phys Med Rehabil. 1999;80(11):1402.
- Thomas DR. Prevention and treatment of pressure ulcers: what works? what doesn’t? Cleve Clin J Med. 2001;68(8):704.
- Wall BM, Mangold T, Huch KM, Corbett C, Cooke CR. Bacteremia in the chronic spinal cord injury population: risk factors for mortality. J Spinal Cord Med. 2003;26(3):248.
- Tleyjeh IM, Berlowitz D, Baddour LM. Infectious complications of pressure-induced skin and soft tissue injury. UpToDate. https://www.uptodate.com/contents/infectious-complications-of-pressure-induced-skin-and-soft-tissue-injury?search=pressure%20ulcers&source=search_result&selectedTitle=2~150&usage_type=default&display_rank=2#H621893729. Published November 04, 2019. Accessed July 03, 2020.
- Grippi MA, Elias JA, Fishman JA et al. eds. Fishman Pulmonary Diseases and Disorders, Fifth Edition. McGraw-Hill; Accessed July 04, 2020: https://accessmedicine-mhmedical-com.proxy.library.upenn.edu/content.aspx?bookid=1344§ionid=79339192
- McKinley WO, Gittler MS, Kirshblum SC et al. Spinal cord injury medicine. 2. Medica. Complications after spina. Cord injury: Identification and management. Arch Phys Med Rehabil. 2002;83:S58-S64, S90-S98.
- Popa C, Popa F, Grigorean VT, et al. Vascular dysfunctions following spinal cord injury. J Med Life. 2010;3(3):275-285.
- Burns SP, Weaver FM, Parada JP et al. Management of community-acquired pneumonia in persons with spinal cord injury. Spinal Cord. 2004;42:450-458.
- Eldahan KC, Rabchevsky AG. Autonomic dysreflexia after spinal cord injury: systemic pathophysiology and methods of management. Auton Neurosci. 2018;209:59-70.
- Camune BD. Challenges in the management of the pregnant woman with spinal cord injury. J Perinat Neonat Nurs.2013;27(3):225-231.
- K Furusawa et al. Incidence of symptomatic autonomic dysreflexia varies according to the bowel and bladder management techniques in patients with spinal cord injury. Spinal Cord. 2011;49:49-54.
- DiTommaso C, Kopp FS, Linville CR. General topics in inpatient rehabilitation. In: Mitra R. eds. Principles of Rehabilitation Medicine. McGraw-Hill; Accessed July 02, 2020: https://accessmedicine-mhmedical-com.proxy.library.upenn.edu/content.aspx?bookid=2550§ionid=206764359
- Brown R, DiMarco AF, Hoit JD, Garshick E. Respiratory dysfunction and management in spinal cord injury. Respir Care. 2006;51:853-868.
- Winslow C, Rozovsky J. Effect of spinal cord injury on the respiratory system. Am J Phys Med Rehabil. 2003;82:803-814.
- Sezer N, Akkus S, Ugurlu FG. Chronic complications of spinal cord injury. World J Orthop. Jan 18, 2015;6(1):24-33.
- Muller R, Landmann G, Bechir M et al. Chronic pain, depression, and quality of life in individuals with spinal cord injury: Mediating role of participation. J Rehabil Med. 2017;49(6):489-496.
- Thapa S, Kitrungrote L, Damkliang J. Chronic pain experience and pain management in persons with spinal cord injury in Nepal. Scand J Pain. 2018;18(2):195-201.
- Walters ET. How is chronic pain related to sympathetic dysfunction and autonomic dysreflexia follow spinal cord injury? Autonomic Neuroscience. 2018;209:79-89.
- Finnerup NB, Basstrup C. Spinal cord injury pain: mechanisms and management. Curr Pain Headache Rep.2012;16:207-216.
- Hagen EM, Lie SA, Rekand T, Gilhus NE, Gronning M. Mortality after traumatic spinal cord injury: 50 years of follow-up. J Neurol Neurosurg Psychiatry. 2010;81(4):368.
- Kirshblum SC, Priebe MM, Ho CH, Scelza WM et al. Spinal cord injury medicine. 3. Rehabilitation phase after acute spinal cord injury. Arch Phys Med Rehabil. 2007;88(3 Suppl 1):S62.




