Authors: Joseph R. Peters, DO, RDMS and Jeremy Owens, DO (Department of Emergency Medicine, OSF St Francis Medical Center, University of Illinois College of Medicine, Peoria, IL) // Reviewed by: Stephen Alerhand, MD (@SAlerhand), Brit Long, MD (@long_brit)
Introduction
Acute Aortic Dissection (AAD) is a life-threatening emergency requiring rapid diagnosis and treatment. AAD is an uncommon condition with an incidence of 1– 4/100,000 per year (1). Acutely, the mortality approaches 1–2% per hour over the first 24 – 48 h in Stanford type A dissection. (1) More than 90% of aortic dissections present with acute pain. (7) In one study, the most common misdiagnosis was acute coronary syndrome (6). Neurologic deficits have been reported to occur in 13–42% of patients with AAD; ischemic stroke being the most frequent complication, occurring in 6–32% of patients. (3) Point of care ultrasound (POCUS) is a bedside diagnostic modality that Emergency Physicians (EPs) can incorporate into crisis care presentations, providing the ability to more rapidly differentiate critical illnesses, mobilize consultants, and implement accurate decision-making during patient care.
Case
A 54-year-old female with no past medical history arrived in the ED unresponsive, post seizure, hypotensive. The patient was found by EMS on the floor of her office unresponsive to verbal stimuli, demonstrating a fixed leftward gaze of both eyes and dense paralysis of her right arm and leg. The patient seized during transport just before arriving at the emergency department. Field glucose was 122mg/dl. Vital signs on arrival T 98.1, BP 78/48, HR 105, RR 10, 96% on room air.
In the ED, the patient was not responsive to verbal interaction, but she did withdraw her left arm and leg when noxious stimuli were applied. Her right arm and leg were flaccid on exam. EMS personnel emphasized their concern for acute stroke; however, coworkers had also reported to them that the patient “cried out” she was experiencing chest pain before collapsing unresponsive. Further exam revealed the patient lacked palpable pulses in either radial artery, the right ankle, or right foot, but was found to have a strong pulse in the left ankle and left foot. Although bilateral arm blood pressures indicated hypotension, blood pressure was 235/96 in the left leg.
The patient was intubated, and a POCUS echocardiogram was performed. The parasternal long axis view identified a dilated aortic root, measuring 5cm. (Img. 1) This finding prompted EPs to ultrasound the aortic arch, the carotid arteries, and the abdominal aorta in search of dissection flaps. Dissection flaps were visualized in the aortic arch and in the right common carotid artery. The descending abdominal aorta could not be visualized due to bowel gas conditions, likely related to bag-valve-mask therapy in route. A cardiothoracic surgeon was consulted immediately and met the patient at the CT scanner within minutes of her arrival.
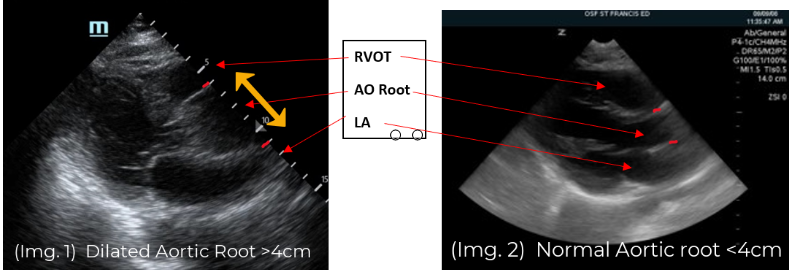
(Img. 1) PSLAX aortic root ~5cm. (Img. 2) Normal aortic root appearance.
Discussion
As is often the case in crisis-care presentations, the differential diagnosis in this patient was extensive and included multiple etiologies: massive pulmonary embolism, cardiac arrest, acute stroke, a postictal state with Todd’s paralysis, AAD, syncope with brain injury from fall. Limited history in combination with blood pressure atypical for a stroke presentation (hypotension) created a high-stakes, diagnostic challenge. Point-of-care ultrasound (POCUS) identified the etiology of this stroke presentation within minutes of arrival. CT angiogram subsequently confirmed the POCUS findings of a Stanford type A aortic dissection involving the aortic arch, with extension to the right brachiocephalic artery, right subclavian artery, right common carotid artery, left subclavian artery, and left common carotid with thrombus occlusion at its origin. Additionally, it revealed a 5.2cm ascending thoracic aneurysm and a 4.7 cm infrarenal abdominal aneurysm. (Img. 3) The AAD had diminished blood flow to both arms, the right leg, and caused complete occlusion of left common carotid artery resulting in a massive left hemispheric ischemic stroke. CT brain was negative for hemorrhage.
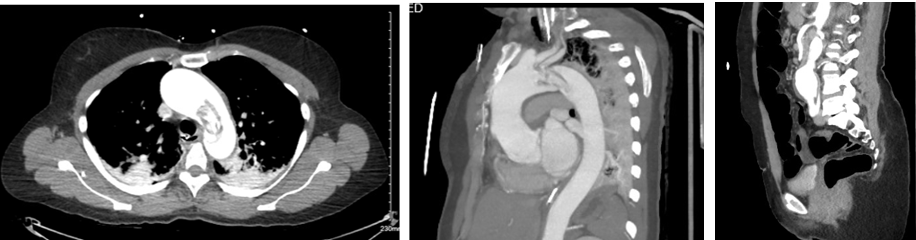
(Img. 3) CT scan acute aortic dissection, thoracic aneurysm and infrarenal AAA.
Classic AAD symptoms have been described as severe (90%), abrupt (84-90%), sharp or tearing (64%), retrosternal or interscapular (50%), migrating (16%), down the back (46%) and maximal at onset. (8) Not all cases of AAD present with classic symptoms, however, making the diagnosis challenging (2). Remarkably, chest pain is not an obligatory symptom of AAD and the frequency of pain-free dissections range between 5 to and 15%; especially in AADs with neurological sequelae. (5) In one study, 29% of patients presenting with AAD complained of neurologic symptoms including ischemic stroke (16%), spinal cord symptoms (1%), ischemic neuropathy (11%), hypoxic encephalopathy (2%), syncope (6%) and seizures (3%). (4) Of these patients, one-third of the ischemic stroke patients did not have pain. (4) In 50% of these patients the neurologic symptoms were transient. (4) In addition, altered consciousness, alterations of speech or language may prevent recognition of pain as a symptom. (8) Although AAD has been described as a less frequent cause of ischemic stroke, when present, right hemispheric strokes predominate related to the greater proximity of the right carotid axis with the aortic root, and bilateral strokes have been described (8).
FOCUS findings in AAD
Ascending aortic dilation identified by Focused Cardiac Ultrasound (FOCUS) is approximately 70% sensitive for AAD, which outperforms the findings of aortic insufficiency on cardiac auscultation (44%), pulse deficit (19%), chest radiograph with wide mediastinum (62%) or electrocardiogram (ECG) findings (17-25%). (9) In one study, combining FOCUS with abdominal aorta POCUS identified 96.4 % of patients who presented with an aortic dissection. (10) In this study, three signs from FOCUS to suggest AAD included: the presence of either a pericardial effusion, an intimal flap, or an aortic outflow track diameter greater than 3.5cm. (10) Investigators in this study also performed an abdominal aorta POCUS with the goal of identifying an undulating echogenic line (intimal flap) suggesting AAD. These 4 criteria showed a sensitivity of 96.4% and specificity of 90.8% for AAD. (10) FOCUS identifies multiple signs of AAD including dilated aorta, the presence of an intimal flap, pericardial effusion, and acute aortic regurgitation. (8) A small case study also identified the presence of the Mercedes Benz sign of the aortic root identified on the subxiphoid view of the heart in patients presenting with AAD. (12)
POCUS reduces door-to-diagnosis time.
POCUS decreases door-to-diagnosis time of AAD. (11) Wang et al. evaluated 172 patients presenting to emergency departments (EDs). In this study, 72 patients received EP performed FOCUS exam and 55 patients in the control group did not. They found a door-to-diagnosis time of 10.5 minutes in EP FOCUS group vs 79.0 minutes in the control group, with no adverse effect on door-to-targeted treatment or door-to-CTA times. (11) In our stroke patient, EUS identified a dilated aortic root, an intimal flap in the aortic arch, and the right carotid artery. Diagnosis of AAD was made within minutes of arrival, prior to CT scanning or the administration of thrombolytic therapy. Thrombolysis is an established therapy for selected patient with acute ischemic stroke within the narrow time window of 4.5 hours from onset of symptoms. (8) AAD is an absolute contraindication for administration of thrombolytics with a 71% mortality in patients receiving TPA. (8) EUS signs of AAD whether direct (intimal flap) or indirect (dilated aortic root, pericardial effusion, acute aortic regurgitation) are findings EPs can rapidly identify at the bedside with ultrasound.
POCUS AAD evaluation in stroke and chest pain presentations
Aortic-focused transthoracic echocardiography and abdominal aorta ultrasonography have been proposed as a rapid and noninvasive method to rule in AAD when considering fibrinolysis in suspected acute stroke or myocardial infarction presentations. (8) Roudaut et al. investigated 763 patients with suspicion of AAD with transthoracic echocardiography (TTE). Investigators diagnosed 128 cases of AAD confirmed by angiography, CT, surgery, or autopsy. Two echocardiographic features were found to strongly suggest the diagnosis of thoracic aortic dissection included dilation of any segment of the thoracic aorta visualized, yielding a sensitivity of 95% and a specificity of 51%; and visualization of an intimal flap, which had a sensitivity of 67% and a specificity of 100%. (12, 13) The views used were parasternal long and short axis, apical views, and the suprasternal notch view. Aneurysmal dilation of the aorta is frequently present in AAD, with approximately 90% of AAD patients having dilation of the aorta greater than 4 cm at the time of diagnosis. (9) When aortic dissection is suspected, POCUS of the thoracic aorta, the carotid arteries, and the abdominal aorta may provide EPs signs of AAD as demonstrated in our case.
Echo Window: Parasternal long axis view (PSLAX)
The PSLAX view of the heart is a standard echocardiographic window used in EUS. The aortic root is identified at the basilar center of the heart, imaging well in this view. (Img. 2) The PSLAX is performed by placing the transducer over the long axis of the heart, in the 3rd-5th parasternal rib space. The aortic outflow tract is visualized exiting the heart superiorly between the two neighboring basilar structures, the right ventricular outflow tract (RVOT) and the left atrium (LA) (Img. 2). A normal aortic outflow tract measures < 3.8 cm (12) and appears similar in diameter to the RVOT and the LA by comparison. (Img. 2) When the aortic outflow tract grossly appears to be the largest of the three basilar structures of the heart (Img. 1), the presence of thoracic aneurysm is considered, and the aortic root is scanned thoroughly for visualization of an intimal flap. Intimal flaps appear as an undulating echogenic (white) line within the lumen of the aorta. When present, intimal flaps can be visualized in both the long and short axis views of the aortic root as demonstrated in this 71-year-old patient with anterior chest pain and posterior interscapular pain. (Vid. 1) When imaging the aortic root, cautious interpretation is required to avoid mistaking the motion of the aortic valve leaflets as dissection flaps. In our stroke patient, the aortic root was approximately 5cm in diameter and no intimal flap was identified. (Vid. 2)

(Vid. 1) Aortic root intimal flaps. (Vid. 2) Dilated AO root, no flap. Our case.
The PSLAX view of the heart additionally provides the opportunity to visualize the descending thoracic aorta in the far field of the same image (Vid. 3). The descending thoracic aorta normally appears as an oval anechoic structure located in the far field of the PSLAX view of the heart and can be assessed for the presence of an intimal flap. This is an important area to image when considering Stanford Type B dissection, as it originates distal to the left subclavian artery and an intimal flap would not be present in the region of the more proximal aortic root, arch, or common carotid arteries.

(Vid. 3) PSLAX descending thoracic Aorta (Img. 4) Probe position suprasternal notch.
Suprasternal Notch Window
The suprasternal notch window (aortic arch view) allows for the identification of an intimal flap in the thoracic aortic arch. This view is obtained by placing the transducer in the suprasternal notch, rotating the length of the probe between the left sternocleidomastoid muscle and the right clavicular head. The ultrasound beam is then directed downward into the chest while gradually fanning the tail of the probe toward the patient’s right (US beam left), which directs the ultrasound beam to transect the long axis of the aortic arch in its anatomical leftward location. Often the patient’s chin must be rotated to the right or left to accommodate the tail of the US probe. (Img. 4) The normal aortic arch and its branches (the right brachiocephalic artery, the left common carotid artery, and the left subclavian artery) appear as anechoic tubular structures. (Vid. 4) In Type A dissections an intimal flap appears as a pulsatile echogenic linear line visible within the aortic arch. (Vid. 5) A diseased aortic arch may not image as succinctly as a healthy aortic arch due to tortuous changes; however, as seen in our patient, the intimal flap is clearly recognizable. (Vid. 5)
(Vid. 4) Normal aortic arch and branches. (Vid. 5) Our patient with aortic arch intimal flap.
Common Carotid Windows
Whether stroke symptoms are present or not, imaging the common carotid arteries offers another routine area to identify intimal flaps. EPs are typically familiar with the appearance of the common carotid arteries given these are imaged routinely during insertion of ultrasound guided internal jugular central venous catheters. The common carotid arteries are imaged with the linear probe in short axis, sliding the probe from the clavicle to the angle of the jaw. Normal common carotid artery lumens appear anechoic, but in the presence of an intimal flap, an echogenic pulsatile line is visible, as imaged in the right common carotid artery of our stroke patient. (Vid. 6) Although an intimal flap was present in the right carotid artery, our patient had no left sided stroke findings.
EPs should also be aware that intimal flaps can be visualized in the common carotid arteries of patients diagnosed with AAD yet lacking stroke symptoms. This 56-year-old male complained of less than 5 minutes of sudden intense pain that radiated through his neck, chest, and abdomen to his right thigh. He was pain free in the ED and stated his visit was prompted by the fact the episode made him transiently near syncopal. POCUS evaluation of his heart, aortic arch, carotid arteries, and abdominal aorta identified a dilated aortic root and arch, an intimal flap in the right carotid artery with thrombus, and an intimal flap in the abdominal aorta. (Vid. 7) The 71-year-old patient previously discussed with the dissection flaps identified in the aortic root also lacked stroke symptoms, however an intimal flap was present in his left common carotid artery. (Vids. 8,1)
(Vid. 6) Right Carotid Intimal Flap. (Vid. 7) Intimal Flap Rt Carotid and Abdominal Aorta
Abdominal Aorta Window
POCUS of the abdominal aorta for the identification of abdominal aneurysm (AAA) is a commonly performed exam in the ED. The abdominal aorta is typically imaged in both the long and short axis from the proximal celiac trunk to the distal aortic bifurcation. Both Stanford type A and B dissections have the potential to dissect through the abdominal aorta and as a result, the abdominal aorta is another location to identify intimal flaps. An abdominal aorta intimal flap is visible in this Type A dissection of a 64-year-old male who had sudden onset chest and back pain with non-ischemic ECG. POCUS of the heart and the aortic arch were difficult to image due to his COPD hyperinflated lungs. No intimal flaps were identified in his carotid arteries. An intimal flap was discovered in his abdominal aorta and visible in both the long and short axis views. (Vid. 9) In the Type B dissection of this 49-year-old female, an irregular appearing intimal flap is identified in the abdominal aorta proximal to the celiac trunk. (Vid. 10) Given her writhing-pain appearance and young age, POCUS was utilized initially to evaluate for hydronephrosis of her left kidney but was not identified. Subsequent imaging of the abdominal aorta revealed an intimal flap in her proximal abdominal aorta. This finding immediately changed therapy and a contrast CT scan of the chest and abdomen revealed a Type B aortic dissection determined to be the sequela of chronically uncontrolled hypertension and use of cocaine. (Img. 5)
(Vid. 8) Left Carotid Artery Dissection Flap (Vid. 9) Type A dissection abdominal aorta
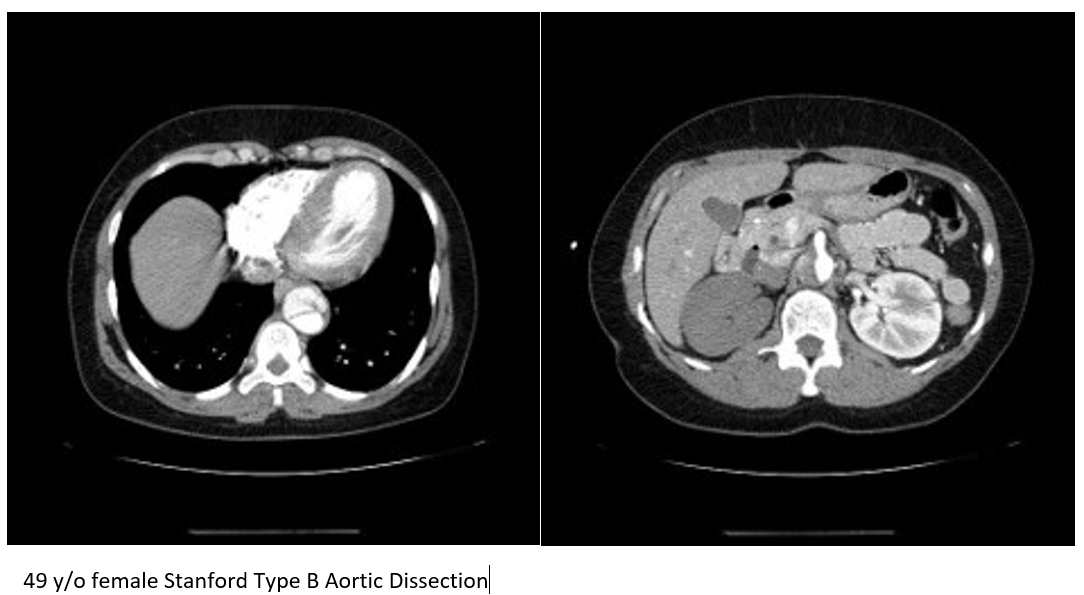
(Vid. 10) Type B dissection abdominal aorta. (Img. 5) Type B dissection abdominal aorta.
Summary
AAD with neurologic symptoms at onset is an uncommon presentation in the ED. The neurologic symptoms may be transient, and up to one-third of these patients may present without pain. (4) Stroke is a dreaded complication of AAD and can present with altered mental status or aphasia making the expression of pain impossible. (8) Patients presenting with stroke symptoms or thoracic pain demonstrating unusual combinations of vital signs or exam findings may harbor AAD as the etiology of their condition. POCUS demonstrates the ability to rapidly rule in AAD in these patients via the identification of an intimal flap in any of the multiple locations the major arteries can be visualized: the aortic root, aortic arch, common carotid arteries, the descending thoracic aorta, and abdominal aorta. A dilated aorta or pericardial effusion may represent an indirect sign that an AAD is present. POCUS of the heart, the thoracic aortic arch, the carotid arteries, and abdominal aorta revealing these signs expedites advanced imaging, consultant mobilization, and accurate decision-making in the care of patients with AAD.
References
- Fojtik JP, Costantino TG, Dean AJ. The diagnosis of aortic dissection by emergency medicine ultrasound. J Emerg Med. 2007;32(2):191-196.
- Woo KM, Schneider JL. High-Risk Chief Complaints I: Chest Pain—The Big Three. Emerg Med Clin N Am 2009; 27:685-712.
- Kamouchi, M. Aortic Dissection as a Possible Underlying Cause of Acute Ischemic Stroke. Circulation. 2015;79: 1697-1698.
- Gaul C, Dietrich W, Friedrich I, Sirch J, Erbguth FJ. Neurological symptoms in type A aortic dissections. Stroke 2007; 38: 292–297.
- Gaul C, Dietrich W, Erbguth FJ. Neurological symptoms in aortic dissection: A challenge for neurologists. Cerebrovasc Dis 2008; 26: 1–8.
- Hansen MS, Nogareda GJ, Hutchison SJ. Frequency of and inappropriate treatment of misdiagnosis of acute aortic dissection. Am J Cardiol. 2007 Mar 15;99(6):852-6.
- Braverman AC. Aortic dissection: prompt diagnosis and emergency treatment are critical. Cleve Clin J Med. 2011 Oct;78(10):685-96.
- Alonso JV, Martin D, Kinderman H, Farhad I, Swallow P, Siggers A. Acute ischemic stroke what is hidden behind? J Cardiol Cases. 2017 Aug 30;16(5):174-177.
- Pare JR, Liu R, Moore CL, Sherban T, Kelleher MS Jr, Thomas S, Taylor RA. Emergency physician focused cardiac ultrasound improves diagnosis of ascending aortic dissection. Am J Emerg Med. 2016 Mar;34(3):486-92.
- Gibbons R, Smith D, Mulflur M, Dai T, Satz W, Goett H, et al. 364 Point-of-Care Ultrasound for the Detection of Aortic Dissections in the Emergency Department. Annals of Emergency Medicine. 2017;70:S143.
- Wang Y, Yu H, Cao Y, Wan Z. Early Screening for Aortic Dissection With Point-of-Care Ultrasound by Emergency Physicians: A Prospective Pilot Study. J Ultrasound Med. 2020 Jul;39(7):1309-1315.
- Blaivas M, Sierzenski PR. Dissection of the proximal thoracic aorta: a new ultrasonographic sign in the subxiphoid view. Am J Emerg Med. 2002 Jul;20(4):344-8.
- Roudaut RP, Billes MA, Gosse P, Deville C, Baudet E, Fontan F, Besse P, Bricaud H, Dallocchio M. Accuracy of M-mode and two-dimensional echocardiography in the diagnosis of aortic dissection: an experience with 128 cases. Clin Cardiol. 1988 Aug;11(8):553-62.





2 thoughts on “POCUS for aortic dissection in the clinical presentation of ischemic stroke”
Pingback: Zedu Weekly Wrap - 18 November 2022
Pingback: Quiz 168, November 18th, 2022 – The FOAMed Quiz