
Author: Ava E. Pierce, MD, FACEP (Professor of Emergency Medicine, UT Southwestern Medical Center) // Edited by: Alex Koyfman, MD (@EMHighAK) and Brit Long, MD (@long_brit)
Case
A 39-year-old female with a history of diabetes presents to the ED with dizziness, weakness, and vomiting. She was discharged from another ED the day prior to arrival with a diagnosis of influenza and hyperglycemia. She returns today because her symptoms have worsened. She came to your ED rather than returning to the other hospital because her mother wanted her to get a second opinion at a different hospital since she has gotten worse and is so weak that she is unable to walk today.
Dizziness and vertigo account for approximately 4.4 million emergency department (ED) visits per year (approximately 4% of ED visits) (1).Emergency medicine physicians must distinguish the self-limiting causes of dizziness from the serious causes (2). Strokes are the final diagnosis for 3–5% of these ED visits for dizziness and vertigo (3).
How do you approach the weak and dizzy patient?
What do you think her diagnosis will be?
Introduction
Stroke is a leading cause of disability in the United States (1,4-6). Twenty percent of ischemic events in the brain involve the posterior circulation. Causes of posterior circulation ischemia include atherosclerosis, embolism, dissection, and dolichoectasia (elongation and tortuosity) of the vertebral and basilar arteries. Approximately one-third of posterior circulation strokes are caused by occlusive disease within the intracranial vertebral, basilar, and posterior cerebral arteries and the vertebral arteries in the neck and the innominate and subclavian arteries in the chest. (7-11). Patients with posterior circulation strokes are misdiagnosed more than twice as often as those with anterior circulation strokes (12).
Signs, Symptoms, and Differential Diagnosis
The differential diagnosis of dizziness can include (2,3,13-15):
- General Medical (including cardiovascular) Diagnoses (approximately 50%):
- Fluid and electrolyte disturbances
- Dehydration
- Cardiac arrhythmias
- ACS
- Anemia
- Hypoglycemia
- Adrenal Insufficiency
- Aortic Dissection
- Carbon Monoxide Intoxication
- Pulmonary Embolus
- Thiamine Deficiency
- Orthostatic Hypotension
- Medication Side Effects
- Otovestibular diagnoses (approximately 33%)
- Peripheral vestibular problems
- BPPV
- Meniere disease
- Vestibular Neuritis and Labyrinthitis
- Peripheral vestibular problems
- Neurologic diagnoses (approximately 11%)
- CVA
- TIA
- Migraine
- Posterior Fossa Mass
The presenting signs and symptoms of posterior circulation stroke are often non-specific and fluctuating, adding to the challenge in making the diagnosis (14). In 407 patients from the NEMC-PCR, the most frequent presenting symptoms were dizziness (47%), unilateral limb weakness (41%), dysarthria (31%), headache (28%) and nausea or vomiting (27%). The most frequent signs were unilateral limb weakness (38%), gait ataxia (31%), unilateral limb ataxia (30%), dysarthria (28%) and nystagmus (24%) (14,15).
The following increase the likelihood of a central causes of dizziness (16-22):
- History of previous stroke
- History of vascular disease
- Increasing age
- Complaint of ‘‘instability’’
- Abnormal gait
- Focal neurologic findings
The following increase the risk of a missed cerebellar stroke:
- Vertebral dissection
- Younger age (16,23–24)
Misdiagnosis of central versus peripheral vertigo is frequent. The traditional approach to evaluating patients with dizziness, relies on the description of the dizziness (i.e. vertigo, disequilibrium, lightheadedness, pre-syncope,) to help distinguish peripheral versus central causes of dizziness (16,25). The symptoms quality approach to dizziness is based on asking a patient to describe what he/she means by dizziness and then using those responses to guide the differential diagnosis and evaluation. This approach depends on patients being able to consistently choose only one dizziness type which can be linked with a given differential diagnosis. The descriptive words that patients use to describe dizziness are not diagnostically meaningful and should not be used to drive the evaluation. Using the traditional diagnostic approach of asking “What do you mean by ‘dizzy’?” may contribute to misdiagnosis (16,26).
The timing and triggers approach is more evidence-based and will lead to a more accurate differential diagnosis of dizziness (12,13,15).
The mnemonic ATTEST can be used during the evaluation of patients with dizziness:
- A – Associated symptoms
- T – Timing
- T – Triggers
- E – bedside Examination
- S – Signs
- T – additional Testing as needed (16)
Dividing patients into three categories using timing and triggers can help to differentiate central versus peripheral lesions:
- Acute Vestibular Syndrome (AVS)
- Acute, continuous dizziness lasting days, accompanied by nausea, vomiting, nystagmus, head motion intolerance, and gait unsteadiness
- Physical examination differentiates vestibular neuritis from stroke
- Spontaneous Episodic Vestibular Syndrome (s-EVS)
- Episodic dizziness that occurs spontaneously, is not triggered, and usually last minutes to hours
- Associated symptoms help differentiate vestibular migraine from transient ischemic attack
- Physical examination is often no helpful in making the diagnosis
- Triggered Episodic Vestibular Syndrome (t-EVS)
- Episodic dizziness brought on by a specific, trigger (such as a change in head position or standing up), and usually lasting <1 min
- The Dix-Hallpike and supine roll test help differentiate benign paroxysmal positional vertigo from posterior fossa structural lesions (16).
A 3-step bedside oculomotor examination (HINTS: Head-Impulse, Nystagmus, Test-of-Skew) is helpful in making the diagnosis of stroke (27).

A 2009 study showed that the HINTS exam was more sensitive than MRI within the first 48 hours for differentiating neuritis from stroke (12). The horizontal head impulse test (h-HIT) of vestibulo-ocular reflex (VOR) function appears to be the most consistent bedside predictor of pseudolabyrinthine stroke in AVS (28). This test was first described in 1988 by Halmagyi and Curthoys as a bedside test for peripheral vestibular disease (28,29). A normal VOR by h-HIT strongly indicates a central localization. Some patients with abnormal h-HIT have lateral pontine strokes (29).
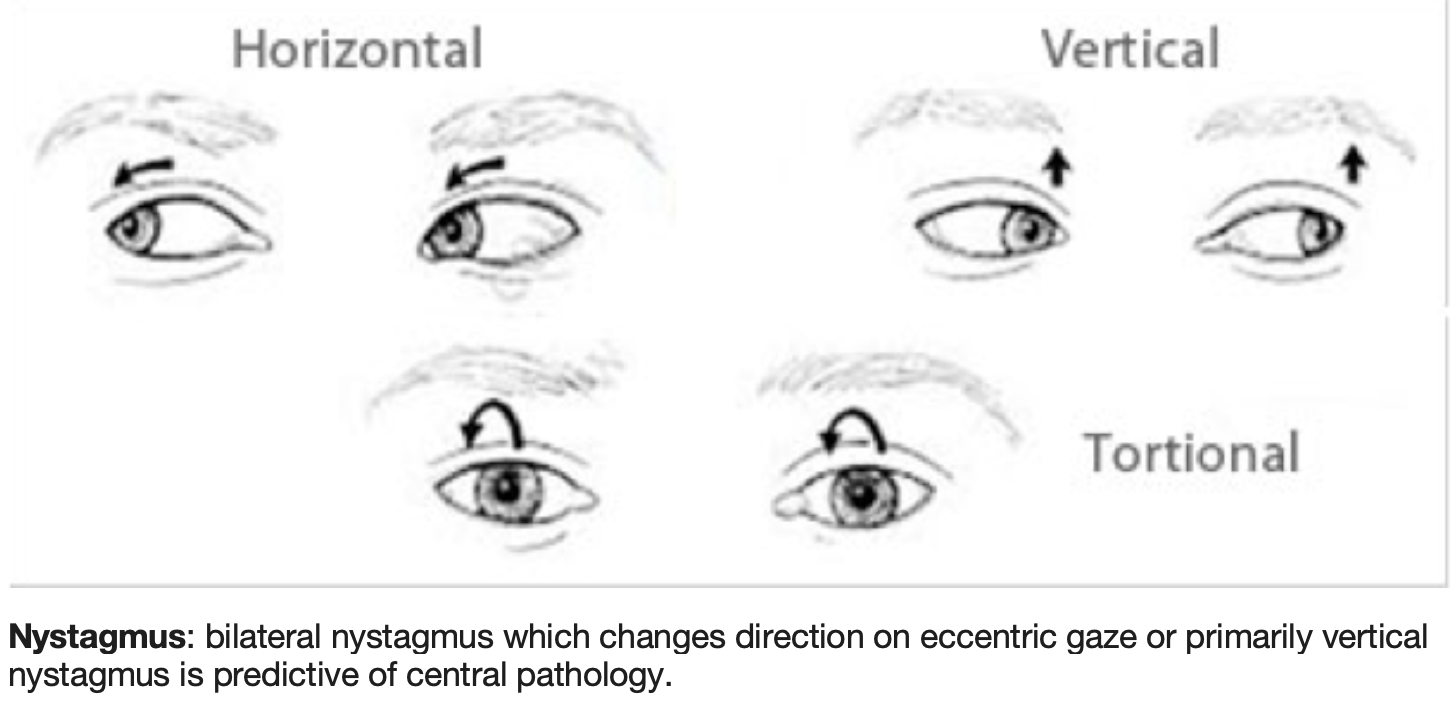
Another bedside predictor that a central cause is present in the acute vestibular syndrome is nystagmus, which changes direction on eccentric gaze. Vertical or torsional nystagmus suggests central pathology. Most strokes presenting an AVS picture have nystagmus with a predominantly horizontal vector that mimics APV. What sometimes distinguishes the nystagmus typical of central AVS from APV is a change in direction on eccentric gaze.
A third bedside predictor of central pathology is skew deviation. Skew deviation is vertical ocular misalignment that results from a right–left imbalance of vestibular tone to the oculomotor system. Skew is generally detected by alternate cover testing. Skew has principally been identified as a central sign in those with posterior fossa pathology and is most commonly seen with brainstem strokes (28,30–32).
HINTS only applies to patients with s-AVS (or s-EVS while the patient remains acutely symptomatic), including spontaneous or gaze-evoked nystagmus; HINTS should not be used in patients who have other syndromes, particularly t-EVS, where normal head impulse test results would erroneously imply stroke in the majority with BPPV (33).
A 2020 systematic review and meta-analysis by Ohle documented that the HINTS exam performed by neurologists had a sensitivity of 96.7% and Specificity 94.8%; when performed by a cohort of physicians including both emergency physicians and neurologists the sensitivity was 83% and specificity 44%. He concluded that the HINTS exam when used in isolation by emergency physicians has not been shown to be sufficiently accurate to rule out a stroke in those presenting with AVS (34).
Edlow suggests performing the physical exam in the following order:
- Nystagmus testing
- Skew deviation/Test of Skew
- Head impulse test (HIT)
- General neurologic examination, focusing on cranial nerves, including hearing, cerebellar testing, and long-tract signs
- Gait testing (16)
Acute Vestibular Syndrome
Edlow suggest performing gaze testing first since nystagmus is part of the definition of AVS, and the diagnostic meaning of HIT differs dramatically in dizzy patients without nystagmus (16, 35).
Most patients with an AVS due to a peripheral vestibular cause will have nystagmus if they are examined within the first days, so its absence makes the diagnosis of vestibular neuritis unlikely. Nystagmus may be absent if vestibular suppressant medications, such as benzodiazepines, have been given (16,36).
Nystagmus can usually be seen with the naked eye, but normal visual fixation can completely suppress mild nystagmus in patients with vestibular neuritis (16,37).
To block visual fixation, EM physicians can place a piece of white paper close to the patient’s eyes, and then instruct them to ‘‘look through the paper’’ and examine for nystagmus from the side. If there is no nystagmus, an acute vestibular neuritis is very unlikely, and the HIT can yield false information (16,36). Thus, HIT should only be performed in patients with acute vestibular syndrome and nystagmus.
Two patterns suggest stroke for nystagmus:
1) Dominantly vertical or torsional nystagmus in any gaze position;
2) Dominantly horizontal nystagmus that changes direction in different gaze positions (e.g., bilateral, gaze-evoked nystagmus).
The most common pattern seen in stroke patients presenting with AVS is direction-fixed horizontal nystagmus (this is the same as that seen in acute vestibular neuritis), therefore further testing is often needed (16,38).
Skew deviation is a vertical misalignment of the eyes (16,39,40). Skew deviation is elicited using the ‘‘alternate cover’’ test. If skew deviation is present, each time the covered eye is uncovered, a slight vertical correction occurs (one side corrects upward and the other corrects downward). If no vertical movement occurs, there is no skew (horizontal movements do not count). A normal response is no vertical correction. An abnormal response suggests a stroke in an AVS presentation (16).

The next component is the HIT, a test of the vestibuloocular reflex (VOR). Standing in front of the patient, the examiner holds the patient’s head by each side, instructs the patient to focus on the examiner’s nose and to keep his/her head and neck loose. The examiner gently displaces the patient’s head 10–20 degrees from the midline to one side; the examiner then brings the head back toward the center position rapidly (>120 degrees/s) where it stops at the midline, while the examiner observes the eyes carefully. The normal response (normal vestibular function) is that the patient’s gaze remains locked on the examiner’s nose. If there is a corrective saccade (the eyes move with the head, then snap back in a fast corrective movement to again look at the examiner’s nose, as instructed) this is considered a ‘‘positive’’ test (abnormal VOR), which generally indicates a peripheral process, usually vestibular neuritis. The HIT is performed to one side then the other, and the absence of a corrective saccade on both sides suggests a central etiology in AVS (16,41).

The HIT is only useful in patients with AVS (with nystagmus). A HIT done in a patient without nystagmus will be normal and, therefore, misleading. Cerebellar stroke patients typically have a negative (normal) HIT, because the circuit of the VOR does not loop through the cerebellum (42,43).
Occasional patients with posterior circulation stroke will have a falsely ‘‘positive’’ (abnormal) HIT, usually from an infarct involving the region where the vestibular nerve enters the brainstem or a stroke of the inner ear itself (labyrinthine stroke) (44). When abnormal HITs occur in stroke, hearing is often affected because blood supply to both structures is generally from the anterior inferior cerebellar artery (AICA), which also supplies the cochlea (45). Adding a bedside test of hearing (‘‘HINTS plus’’) helps to diagnose these patients (46). It is frequently thought that coincident hearing loss and dizziness will be peripheral, but a combined audiovestibular loss is often a sign of stroke (47,48). Patients with the AVS who have worrisome nystagmus, skew deviation, or a bilaterally normal HIT have a presumed stroke and should receive neurology consultation and admission (16).
Patients with lateral medullary stroke (Wallenberg’s syndrome) present with acute dizziness and may also have dysarthria, dysphagia, or hoarseness. They may have Horner’s syndrome with ptosis and anisocoria only evident in dim light (the normal larger pupil fully dilates, accentuating the difference in pupil size) (49). You should also test for pain and temperature sensation to diagnose hemi-facial decreased pain and temperature sensation (16).
If the four examination components (nystagmus, skew deviation, HIT, and targeted neurologic examination) are benign, you should test for gait ataxia or truncal ataxia. Patients who cannot walk or sit up unassisted are more likely to have a central cause of dizziness and require further evaluation (16).
Spontaneous Episodic Vestibular Syndrome
The spontaneous episodic vestibular syndrome (s-EVS) is marked by recurrent, spontaneous episodes of dizziness that lasts from seconds to days. Many of these patients are asymptomatic when they present to the emergency department. The dizziness cannot be triggered at the bedside, so the evaluation usually relies on the history. Perfusion-based imaging (perfusion-weighted MRI) may help diagnose some cerebrovascular causes when examination and history are inconclusive (50).
The most common dangerous cause is posterior circulation TIA (16).
Dizziness is the most common symptom in basilar artery occlusion, occurring without other neurologic symptoms in 20% (51). Dizziness is the most common presenting symptom of vertebral artery dissection, which affects younger patients, mimics migraine, and is easily misdiagnosed (52).
Triggered Episodic Vestibular Syndrome
Patients with triggered episodic vestibular syndrome (t-EVS) have brief episodes of dizziness lasting seconds to minutes, where there is a specific trigger that consistently causes dizziness.
The most common etiologies are BPPV and orthostatic hypotension, but there are central mimics of BPPV.
The diagnosis is confirmed by reproducing symptoms using canal-specific positional testing maneuvers and identifying a canal-specific nystagmus. If the Dix-Hallpike maneuver does not reproduce the symptoms, the supine head roll test can be attempted to diagnose horizontal canal BPPV.
Once the correct canal is identified, bedside treatment with canal repositioning maneuvers can follow (Epley maneuvers) (16,53).
Central mimics of BPPV (central paroxysmal positional vertigo [CPPV]) caused by posterior fossa neoplasm, infarction, hemorrhage, and demyelination are rare.
Orthostatic dizziness without systemic orthostatic hypotension has been reported with hemodynamic TIA (due low flow across a vascular stenosis) and in patients with intracranial hypotension (54,55).
Findings that suggest a central cause of dizziness (16):
- Nystagmus that is dominantly vertical or torsional or dominantly horizontal, direction changing on left/right gaze – More than half of posterior fossa strokes will have direction-fixed horizontal nystagmus that alone, cannot be distinguished from that typically seen with vestibular neuritis.
- Test of Skew with Skew deviation (small vertical correction on uncovering the eye)
- Head Impulse Test bilaterally normal (no corrective saccade) in a patient with acute vestibular syndrome
- Presence of limb ataxia, dysarthria, diplopia, ptosis, anisocoria, facial sensory loss (pain/temperature), unilateral decreased hearing
- Unable to walk unassisted or sit up in stretcher without holding on or leaning against bed or rails
- Dix-Hallpike test findings that suggest a central cause
- Variable direction (usually pure downbeat or horizontal; almost never upbeat or torsional)
- Variable duration (often persists >90 s if position is held; rarely varies significantly in intensity)
- Supine roll test findings that suggest a central cause
- Variable direction (usually pure downbeat or horizontal; rarely upbeat or torsional)
- Variable duration (often persists >90 s if position is held; rarely varies significantly in intensity
- Symptoms or signs that are not seen in BPPV
- Abnormal cranial nerve or cerebellar function
- Diplopia
- Headache
- Atypical nystagmus characteristics or symptoms during positional tests
- Poor response to therapeutic maneuvers
Additional Symptoms
Headache occurs in 8-27% of ischemic strokes and is more common in posterior circulation strokes. Headache and neck pain are often present in vertebral artery dissection (12).
Vomiting is a risk factor for misdiagnosis as it may be severe enough to be a distract from concomitant symptoms of dizziness and headache (56). 27% of the 407 patients in the New England posterior circulation stroke registry has nausea or vomiting (12,57).
Sensory Symptoms
Negative sensory symptoms such as numbness, hearing loss, or loss of sight are more often associated with ischemia (12,58). Thalamic strokes can be an exception to that rule as they can present with positive symptoms – pain and hemiballismus (12).
Altered Mental Status
Acute posterior circulation stroke patients can present with altered mental status. Artery of Percheron strokes can present with decreased mental alertness, limitation of lateral gaze, confusion, and psychiatric symptoms such as apathy, aggression, confabulation, perseveration, and hallucinations (12, 59, 60)). Basilar stroke patients are obviously ill and often have prodromal dizziness and headache and anisocoria and gaze palsies (12,61-62).
Visual Symptoms
Nystagmus, Horner’s syndrome, diplopia, and visual field cuts can be helpful in making the diagnosis of posterior circulation stroke (12).
Language and Speech Deficits
Slurred speech and dysarthria are more common with cortical PCA infarcts. A quick way to test for dysarthria is having the patient say, “Pawtucket” because it tests sounds made using three different parts of the tongue and mouth (12).
Cranial Nerve Deficits
Loss of pain and temperature is seen in lateral medullary infarcts. Cranial nerve symptoms can be seen in small brain stem strokes (12).
Neuroimaging
CT and MRI may be normal during the first 48 hours of ischemic symptoms. CT angiography can show dissection and obstructive lesions at the origin of the vertebral artery (63). Magnetic resonance imaging with diffusion-weighted images (MRI-DWI) misses 15% to 20% of posterior fossa infarctions in the first 24 hours (64). MRI-DWI has maximal sensitivity for brain stem stroke at 72 to 100 hours after infarction (65). If the physical examination suggests that the diagnosis is stroke, do not use a negative MRI result to exclude the diagnosis (26).
Conclusion
Approximately 5% of TIA patients suffer a stroke within 48 hours, so prompt diagnosis is critical. Patients with posterior circulation TIA may have a higher stroke risk than those with anterior circulation TIA. Patients with missed strokes are at risk of having another stroke that could be prevented with secondary prophylaxis, and those with missed posterior circulation strokes can develop posterior fossa edema, which can be fatal.
Case Outcome
After hydration and normalization of her hyperglycemia, the patient remains unable to walk. An MRI is ordered and reveals a CVA. Neurology is consulted, and the patient is admitted.
Take Home Points
- Consider stroke at the most likely diagnosis for abrupt onset of neurologic symptoms
- The timing and triggers diagnostic approach for patients with dizziness is helpful in reducing misdiagnosis and decreasing diagnostic test overuse.
- Fewer than 20% of stroke patients that present with AVS have focal neurological signs
- NIH stroke scales of 0 occur with posterior circulation strokes. Performing the HINTS exam and targeted neurologic exam of the visual fields, cranial nerves, and cerebellar function including and evaluation of gait and truncal ataxia can help reduce misdiagnosis.
- Early brain imaging is frequently non-diagnostic
- Findings that suggest Central Causes of Dizziness:
- Nystagmus that is dominantly vertical or torsional or dominantly horizontal, direction changing on left/right gaze
- Test of Skew with skew deviation
- Head Impulse Test – bilaterally normal (no corrective saccade)
- Limb ataxia, dysarthria, diplopia, ptosis, anisocoria, facial sensory loss (pain/temperature), unilateral decreased hearing
- Ataxia
- Dix-Hallpike test findings that suggest a central cause
- Variable direction
- Variable duration
- Supine roll test findings that suggest a central cause
- Variable direction
- Variable duration
- Abnormal cranial nerve or cerebellar function
- Diplopia
- Headache
References/Further Reading:
- Saber Tehrani AS, Coughlan D, Hsieh YH, et al. Rising annual costs of dizziness presentations to U.S. emergency departments. Acad Emerg Med. 2013;20:689-696.
- Newman-Toker DE, Hsieh YH, Camargo CA Jr, et al. Spectrum of dizziness visits to US emergency departments: cross-sectional analysis from a nationally representative sample. Mayo Clin Proc. 2008;83:765–75.
- Newman-Toker DE, Edlow JA. TiTrATE: a novel, evidence-based approach to diagnosing acute dizziness and vertigo. Neurol Clin. 2015;33:577–99.
- Jauch, E. (2019). Ischemic Stroke: Practice Essentials, Background, Anatomy. Emedicine.medscape.com. Available at: https://emedicine.medscape.com/article/1916852-overview.
- S. Centers for Disease Control and Prevention and the Heart Disease and Stroke Statistics – 2007 Update, published by the American Heart Association. Available at http://www.strokecenter.org/patients/stats.htm.
- Towfighi A, Saver JL. Stroke declines from third to fourth leading cause of death in the United States: historical perspective and challenges ahead. Stroke. 2011 Aug. 42(8):2351-5.
- Caplan, L. (2019). UpToDate. [online] Uptodate.com. Available at: https://www.uptodate.com/contents/posterior-circulation-cerebrovascular-syndromes.
- Caplan LR, Wityk RJ, Glass TA, et al. New England Medical Center Posterior Circulation registry. Ann Neurol. 2004; 56:389.
- Savitz SI, Caplan LR. Vertebrobasilar disease. N Engl J Med. 2005; 352:2618.
- Caplan, L. (2019). UpToDate. [online] Uptodate.com. Available at: https://www.uptodate.com/contents/posterior-circulation-cerebrovascular-syndromes
- Caplan L. Posterior circulation ischemia: then, now, and tomorrow. The Thomas Willis Lecture-2000. Stroke. 2000; 31:2011.
- Gurley K, Edlow J. Avoiding Misdiagnosis in Patients With Posterior Ciruculation Ischemia: A Narrative Review. Academic Emergency Medicine. 2019;00:1-12.
- Edlow JA. A New Approach to the Diagnosis of Acute Dizziness in Adult Patients. Emerg Med Clin North Am.2016 Nov;34(4):717-742. doi: 10.1016/j.emc.2016.06.004. Epub 2016 Sep 7.
- Schulz UG, Fischer U. Posteriorcirculation cerebrovascular syndromes: diagnosis and management. J Neurol Neurosurg Psychiatry. 2017 Jan;88(1):45-53. doi: 10.1136/jnnp-2015-311299. Epub 2016 Apr 12.
- Searls DE, Pazdera L, Korbel E, et al. Symptoms and signs of posterior circulation ischemia in the New England medical center posterior circulation registry. Arch Neurol. 2012;69:346–51.
- Edlow JA, Gurley KL, Newman-Toker DE. A New Diagnostic Approach to the Adult Patient with Acute Dizziness. J Emerg Med.2018 Apr;54(4):469-483. doi: 10.1016/j.jemermed.2017.12.024. Epub 2018 Feb 1.
- Newman-Toker DE, Hsieh YH, Camargo CA Jr, Pelletier AJ, Butchy GT, Edlow JA. Spectrum of dizziness visits to US emergency departments: cross-sectional analysis from a nationally representative sample. Mayo Clin Proc. 2008;83:765–775.
- Navi BB, Kamel H, Shah MP, et al. Rate and predictors of serious neurologic causes of dizziness in the emergency department. Mayo Clin Proc. 2012;87:1080–8.
- Chase M, Joyce NR, Carney E, et al. ED patients with vertigo: can we identify clinical factors associated with acute stroke? Am J Emerg Med. 2012;30:587–91.
- Moubayed SP, Saliba I. Vertebrobasilar insufficiency presenting as isolated positional vertigo or dizziness: a double-blind retrospective cohort study. 2009;119:2071–6.
- Kerber KA, Meurer WJ, Brown DL, et al. Stroke risk stratification in acute dizziness presentations: A prospective imaging-based study. Neurology. 2015;85:1869–78.
- Navi BB, Kamel H, Shah MP, et al. Application of the ABCD2 score to identify cerebrovascular causes of dizziness in the emergency department. Stroke. 2012;43:1484–9
- Masuda Y, Tei H, Shimizu S, Uchiyama S. Factors associated with the misdiagnosis of cerebellar infarction. J Stroke Cerebrovasc Dis. 2013;22:1125–30.
- Newman-Toker DE, Moy E, Valente E, Coffey R, Hines AL. Missed diagnosis of stroke in the ED: a cross-sectional analysis of a large population based sample. Diagnosis (Berl) 2014 1(2): 155–166. doi: 10.1515/dx-2013-0038
- Kerber KA, Newman-Toker DE. Misdiagnosing Dizzy Patients: common pitfalls in clinical practice. Neurol Clin. 2015;33:565–75.
- Edlow J. Diagnosing Patients With Acute-Onset Persistent Dizziness. Ann Emerg Med. 2018;71(5):625-631. doi:10.1016/j.annemergmed.2017.10.012
- Newman-Toker D, Kattah J, Talkad A, Wang D, HsiehI.N.T.S. to Diagnose Stroke in the Acute Vestibular Syndrome—Three-Step Bedside Oculomotor Exam More Sensitive than Early MRI DWI, Stroke. 2009 N Y, ov; 40(11): 3504–3510. doi: 10.1161/STROKEAHA.109.551234
- Kattah J, Talkad A, Wang D, Hsieh Y, Newman-Toker D. HINTS to Diagnose Stroke in the Acute Vestibular Syndrome. Stroke. 2009;40(11):3504-3510. doi:10.1161/strokeaha.109.551234
- Halmagyi GM, Curthoys IS. A clinical sign of canal paresis. Arch Neurol. 1988; 45: 737–739.
- Brodsky MC, Donahue SP, Vaphiades M, Brandt T. Skew deviation revisited. Surv Ophthalmol. 2006; 51: 105–128.
- Newman-Toker DE, Kattah JC, Alvernia JE, Wang DZ. Normal head impulse test differentiates acute cerebellar strokes from vestibular neuritis. Neurology. 2008;70:2378 –2385.
- Newman-Toker DE, Curthoys IS, Halmagyi GM. Diagnosing stroke in acute vertigo: the HINTS family of eye movement tests and the future of the ‘‘Eye ECG.’’ Semin Neurol. 2015;35:506–21.
- Saber Tehrani A, Kattah J, Kerber K et al. Diagnosing Stroke in Acute Dizziness and Vertigo. Stroke. 2018;49(3):788-795. doi:10.1161/strokeaha.117.016979
- Ohle R, Montpellier RA, Marchadier V, Wharton A, McIsaac S, Anderson M, Savage D. Can emergency physicians accurately rule out a central cause of vertigo using the HINTS exam? A systematic review and meta-analysis. Acad Emerg Med.2020 Mar 13. doi: 10.1111/acem.13960.
- Newman-Toker DE, Kattah JC. In reply. Acad Emerg Med. 2014; 21:348–9.
- Taylor RL, McGarvie LA, Reid N, Young AS, Halmagyi GM, Welgampola MS. Vestibular neuritis affects both superior and inferior vestibular nerves. Neurology. 2016;87:1704–12.
- Newman-Toker DE, Sharma P, Chowdhury M, Clemons TM, Zee DS, Della Santina CC. Penlight-cover test: a new bedside method to unmask nystagmus. J Neurol Neurosurg Psychiatry. 2009;80:900–3.
- Tarnutzer AA, Berkowitz AL, Robinson KA, Hsieh YH, Newman-Toker DE. Does my dizzy patient have a stroke? A systematic review of bedside diagnosis in acute vestibular syndrome. CMAJ. 2011;183:E571–92.
- Kerber KA, Meurer WJ, Brown DL, et al. Stroke risk stratification in acute dizziness presentations: A prospective imaging-based study. Neurology. 2015;85:1869–78.
- Lavalle´e PC, Meseguer E, Abboud H, et al. A transient ischaemic attack clinic with round-the-clock access (SOS-TIA): feasibility and effects. Lancet Neurol. 2007;6:953–60.
- Halmagyi GM, Curthoys IS. A clinical sign of canal paresis. Arch Neurol. 1988;45:737–9.
- Lee H, Sohn SI, Cho WY, et al. Cerebellar infarction presenting with isolated vertigo: frequency and vascular topographical patterns. Neurology. 2006;67:1178–83.
- Newman-Toker DE, Kattah JC, Alvernia JE, Wang DZ. Normal head impulse test differentiates acute cerebellar strokes from vestibular neuritis. Neurology. 2008;70:2378–85.
- Newman-Toker DE, Curthoys IS, Halmagyi GM. Diagnosing stroke in acute vertigo: the HINTS family of eye movement tests and the future of the ‘‘Eye ECG.’’ Semin Neurol. 2015;35:506–21.
- Hausler R, Levine RA. Auditory dysfunction in stroke. Acta Otolaryngol. 2000;120:689–703.
- Newman-Toker DE, Kerber KA, Hsieh YH, et al. HINTS outperforms ABCD2 to screen for stroke in acute continuous vertigo and dizziness. Acad Emerg Med. 2013;20:986–96.
- Lee H, Kim JS, Chung EJ, et al. Infarction in the territory of anterior inferior cerebellar artery: spectrum of audiovestibular loss. Stroke. 2009;40:3745–51.
- Lee SH, Kim JS. Acute diagnosis and management of stroke presenting dizziness or vertigo. Neurol Clin. 2015;33:687–98. xi.
- Kim JS. Pure lateral medullary infarction: clinical-radiological correlation of 130 acute, consecutive patients. Brain. 2003;126: 1864–72.
- Choi JH, Park MG, Choi SY, et al. Acute transient vestibular syndrome: prevalence of stroke and efficacy of bedside evaluation. Stroke. 2017;48:556–62.
- Fisher CM. Vertigo in cerebrovascular disease. Arch Otolaryngol. 1967;85:529–534.
- Gottesman RF, Sharma P, Robinson KA, et al. Clinical characteristics of symptomatic vertebral artery dissection: a systematic review. Neurologist. 2012;18:245–254.
- Fife TD, von Brevern M. Benign Paroxysmal positional vertigo in the acute care setting. Neurol Clin. 2015;33:601–617. viii_ix.
- Stark RJ,Wodak J. Primary orthostatic cerebral ischaemia. J Neurol Neurosurg Psychiatry. 1983;46:883–891.
- Blank SC, Shakir RA, Bindoff LA, Bradey N. Spontaneous intracranial hypotension: clinical and magnetic resonance imaging characteristics. Clin Neurol Neurosurg. 1997;99:199–204.
- Calic Z, Cappelen-Smith C, Anderson CS, Xuan W, Cor-dato DJ. Cerebellar infarction and factors associated withdelayed presentation and misdiagnosis. Cerebrovasc Dis. 2016;42:476–84.
- Searls ED, Pazdera L, Korbel E, Vysata O, Caplan LR.Symptoms and signs of posterior circulation ischemia inthe New England Medical Center posterior circulation registry. Arch Neurol. 2012;69:346–51.
- Fernandes PM, Whiteley WN, Hart SR, Al-Shahi SalmanR.Strokes: mimics and Pract Neurol. 2013;13:21–8
- Schmahmann JD. Vascular syndromes of the thalamus. Stroke. 2003;34:2264–78
- Caruso P, Manganotti P, Moretti R. Complex neurologicalsymptoms in bilateral thalamic stroke due to Percheronartery occlusion. Vasc Health Risk Manag. 2017;13:11–4.
- Schonewille WJ, Wijman CA, Michel P, et al. Treatment and outcomes of acute basilar artery occlusion in the Basi-lar Artery International Cooperation Study (BASICS): aprospective registry study. Lancet. 2009;8:724–30.
- Mattle HP, Arnold M, Lindsberg PJ, Schonewille WJ,Schroth Basilar artery occlusion. Lancet Neurol. 2011;11:1002–14.
- Caplan L. UpToDate. Uptodate.com. https://www.uptodate.com/contents/posterior-circulation-cerebrovascular-syndromes. Published 2019.
- Newman-Toker DE, Della Santina CC, Blitz AM. Vertigo and hearing loss. Handb Clin Neurol. 2016;136:905–921. doi: 10.1016/B978-0-444-53486-6.00046-6.
- Axer H, Grässel D, Brämer D, Fitzek S, Kaiser WA, Witte OW, et al. Time course of diffusion imaging in acute brainstem infarcts. J Magn Reson Imaging. 2007;26:905–912. doi: 10.1002/jmri.21088.
- Shah KH, Kleckner K, Edlow JA. Short-term prognosis of stroke among patients diagnosed in the emergency department with a transient ischemic attack. Ann Emerg Med. 2008;51:316–323.
- Flossmann E, Rothwell PM. Prognosis of vertebrobasilar transient ischaemic attack and minor stroke. 2003;126:1940–1954.
- Gulli G, Khan S, Markus HS. Vertebrobasilar stenosis predicts high early recurrent stroke risk in posterior circulation stroke and TIA. Stroke. 2009;40:2732–2737.




