Originally published at R.E.B.E.L. EM on November 1, 2015. Reposted with permission.
Follow Dr. Salim R. Rezaie on twitter @srrezaie
 ECG interpretation is one of the most important skills to master as an emergency physician, and its interpretation can be very complex and frustrating. ECG manifestations can be very subtle, and sometimes the earliest and only ECG change seen will be reciprocal changes alone. To further complicate this, many patients have the atypical symptoms of nausea/vomiting, weakness, or shortness of breath and not chest pain.
ECG interpretation is one of the most important skills to master as an emergency physician, and its interpretation can be very complex and frustrating. ECG manifestations can be very subtle, and sometimes the earliest and only ECG change seen will be reciprocal changes alone. To further complicate this, many patients have the atypical symptoms of nausea/vomiting, weakness, or shortness of breath and not chest pain.
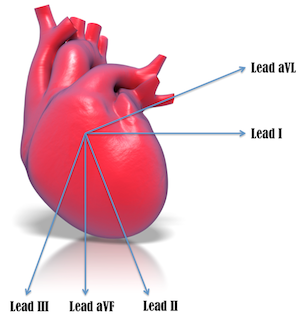
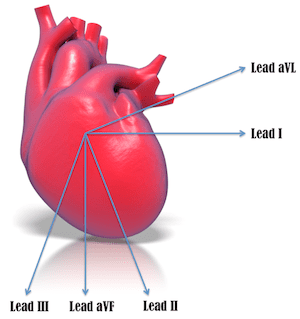 What is the anatomic location of aVL to the heart?
What is the anatomic location of aVL to the heart?
- aVL is the only lead facing the superior part of the left ventricle
- aVL is the only lead that is opposite the inferior wall of the heart (almost 180 degrees from lead III)
What is the differential diagnosis for reciprocal changes in aVL?
- Inferior acute myocardial infarction
- Anterior acute myocardial infarction
- Left ventricular hypertrophy
- Left bundle branch block
- Digitalis Use
How good are reciprocal changes in aVL in diagnosing myocardial infarction (MI)?
- 53.3% of patients with inferior wall MI had reciprocal changes ≥ ST elevation in inferior leads (Parale et al. 2004)*
- 70 – 97.2% of patients with inferior wall MI had reciprocal changes in aVL (Birnbaum et al. 1993)* (Morris and Brady 2002)*
- 30% of patients with anterior wall MI had reciprocal changes in aVL (Morris and Brady 2002)*
Can lead aVL give prognostic information for acute MI?
ST depression ≥0.1 mV in 2 or more lateral leads (I, aVL, V5, or V6) are more likely to:
- Die (14.9% vs 4.1%) (Barrabés et al. 2000)*
- Suffer severe heart failure (14.3% vs 4.1%) (Barrabés et al. 2000)*
- Have angina with ECG changes (20.0% vs 11.6%) (Barrabés et al. 2000)*
What is the most likely culprit artery in inferior MI?
- Right coronary artery (80% of cases): Most likely especially if:
- ST segment elevation lead III > lead II and ST segment depression in lead I and aVL (> 1 mm)
- Sens 90%, Spec 71%, PPV 94%, and NPV 70%) (Zimetbaum and Josephson 2003)*
- Left circumflex artery (20% of cases)

Conclusion
Reading of the ECG remains a crucial diagnostic and prognostic tool for acute MI, and the earliest finding of an acute MI may be reciprocal changes in lead aVL.




