Originally published at R.E.B.E.L. EM on March 25, 2019. Reposted with permission.
Follow Salim R. Rezaie at @srrezaie
Background: TXA is a synthetic lysine derivative that binds with the lysine site on plasminogen and inhibits fibrinolysis. TXA is not a new drug. Studies from the late 1960s and early 1970s have shown reduced bleeding and need for transfusions in many surgical and medical settings. Fast forward to today and we are finding all kinds of uses for TXA other than trauma including post-partum hemorrhage, epistaxis, hemoptysis, gastrointestinal hemorrhage, and many more.
Trauma
MATTERs (Military Application of Tranexamic Acid in Trauma Emergency Resuscitation Study) [1]
What They Did:
- This was a single center, retrospective, observational study at a regional hospital in Afghanistan, comparing TXA vs no TXA in patients receiving at least 1 unit of PRBCs. The study authors also evaluated patients receiving massive transfusion (≥10 units of PRBCs). The standard dosing regimen for TXA was 1g IV with repeated doses as determined by the treating physician.
Outcomes:
- The main (primary) outcomes were 24hr mortality, 48hr mortality, and 30-day mortality. The secondary outcomes of note were transfusion requirements and rate of thromboembolic complications.
Inclusion:
- Consecutive trauma patients, with combat-related injuries, receiving at least 1 unit of PRBCs within 24 hours of admission
Results:
- Trial included 896 patients with combat injuries, of which 293 (32.7%) received TXA within 1hr of injury
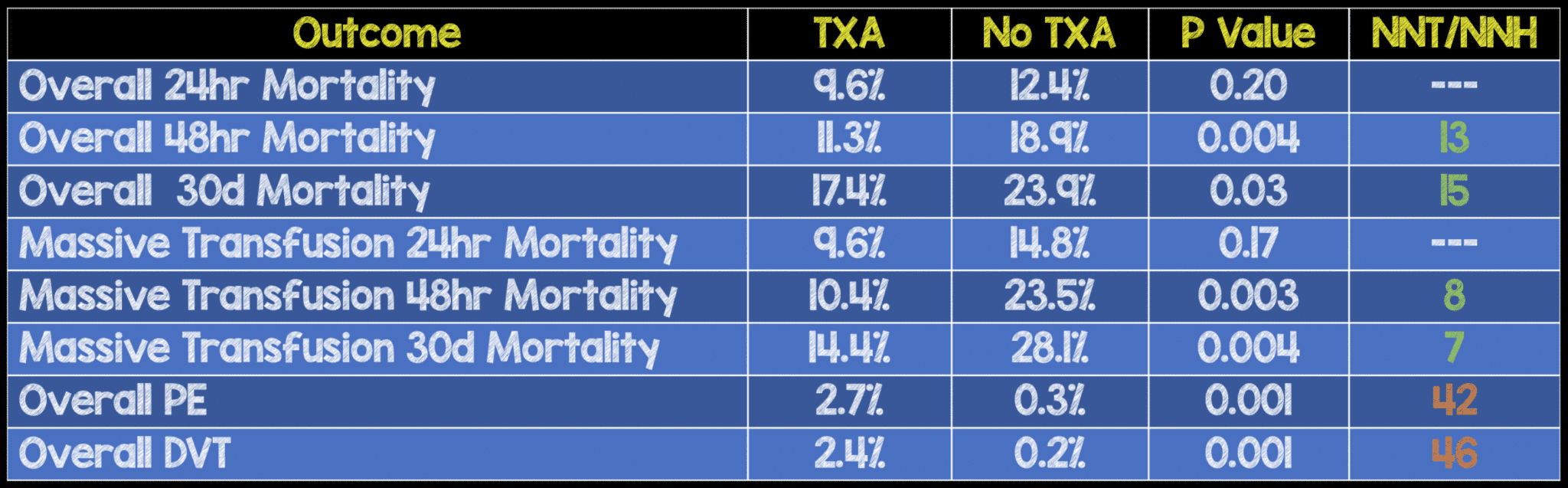
- TXA Independently Associated with Survival: OR 7.228; 95% CI 3.016 – 17.322
- NO FATALITIES from VTE
Strengths:
- First study to report on wartime injuries, which may differ from civilian injuries (i.e. Penetrating trauma vs blunt trauma)
- Consecutive patients included meaning all patients meeting criteria of inclusion were included in this study controlling for sampling bias (i.e. no missed patients that may occur in convenience sampling)
Limitations:
- Clinical practice guidelines, including the use of TXA, were not introduced until the later part of the study period, meaning there may have been slight variations in indications for use and dosing of the medication throughout the majority of the study.
- Due to the small number of VTE events it is unclear if the increased VTE rate with TXA is due to TXA itself or the burden of injury
- The authors were not able to elicit the exact cause or time of death in the patients that died. Some patients who died early in the course of their resuscitation are therefore included in the study, but many of these patients may not have been affected by any therapeutic intervention
Discussion:
- This was a fairly young cohort of patients with and average age of approximately 24 years and the majority of injuries were penetrating trauma not blunt trauma (i.e. almost 100% of the included participants). The patients in the TXA arm, in general, were sicker with higher mean injury severity scores (25.2 vs 22.5), GCS score ≤8 (63.3% vs 35.6%), SBP ≤90mmhg (22.8% vs 13.8%), and mean time in the OR (170min vs 115min), meaning this study most likely underestimated the beneficial effects of TXA. The higher VTE rate in the TXA group should be taken with a grain of salt as these patients also had higher injury burdens, which can also be associated with thrombotic events.
Author Conclusion: “The use of TXA with blood component-based resuscitation following combat injury results in improved measures of coagulopathy and survival, a benefit that is most prominent in patients requiring massive transfusion. Treatment with TXA should be implemented into clinical practice as part of resuscitation strategy following severe wartime injury and hemorrhage.”
Clinical Take Home Point: In patients with penetrating injuries, requiring blood transfusions within 1hr of presentation the use of TXA reduced overall mortality. This effect was even more pronounced in patients requiring massive transfusions (≥10 PRBCs). It is unclear from this study if the increased VTE events in the TXA arm is due to the TXA itself or the higher burden of injury. There were no fatalities due to VTE in this trial.
Clinical Randomisation of an Antifibrinolytic in Significant Haemorrhage 2 (CRASH – 2) [2]
What They Did:
- This was a multicenter, double-blind, randomized, placebo-controlled trial including 274 hospitals in 40 countries, including 20,211 adult trauma patients with or at risk of significant bleeding randomized within 8 hours of injury to either TXA (Loading dose 1g over 10 min, then infusion of 1g over 8hr) or placebo (0.9% Normal saline).
Outcomes:
- The primary outcome was all-cause mortality within 4 weeks of injury. Secondary outcomes included: vascular occlusive events (AMI, stroke, PE, and DVT), surgical intervention, receipt of blood transfusion, and units of blood products transfused
Inclusion:
- Adult trauma patients
- Significant hemorrhage (SBP <90mmHg or HR >110BPM or both)
- At risk of significant hemorrhage
- Within 8 hours of injury
Results:
- 20,211 patients were randomized to TXA (10,060 patients analyzed) or placebo (10,067 patients analyzed).

- No differences in number of blood products transfused or need for any surgery
- Patients with SBP <75mmHg had the largest benefit from TXA (RR 0.87; 95% CI 0.76 – 0.99)
Strengths:
- All participants and investigators were blinded to treatment allocation eliminating conscious and unconscious biases that could potentially affect the trial
- All findings were recorded as intention-to-treat which is based on the initial treatment assignment and not whether or not the patient actually received the treatment.
- The statistical analysis plan was sent to the ethics committee and regulatory agencies prior to unblinding of the results
- Funders of the study had no role in the study design, data collection, data analysis, data interpretation, or writing of the report ensuring no big pharma influences in the results
- The inclusion criteria for this trial did not depend on the results of laboratory tests, making the results of this study applicable in a real world setting
Limitations:
- The number of patients in the early category (≤1hr) was low and therefore subgroup estimates in this group were not accurate.
- Just like the MATTERs trial the number of vaso-occlusive events was so small that the possibility that TXA increases these events cannot be excluded
Discussion:
- Almost 2/3rds of patients were randomized ≤3hrs from their injury and had blunt trauma not penetrating trauma. Also compared to the MATTERs trial this patient population also did not appear to be as sick with >2/3rds of the patients having SBP ≥90mmHg and GCS of 13 – 15. Finally, the number of patients with traumatic brain injury was very small in this study (270 patients), therefore limiting any conclusions in this patient population.
Author Conclusion: “Tranexamic acid safely reduced the risk of death in bleeding trauma patients in this study. On the basis of these results, tranexamic acid should be considered for use in bleeding trauma patients.”
Clinical Take Home Point: The use of TXA in trauma patients with “significant bleeding” reduces all-cause mortality without an increase in thromboembolic events. This effect seems to be greatest in the subset of patients with severe shock (SBP ≤70mmHg) and when given ≤3 hours from time of injury (This final point was confirmed in the meta-analysis of the CRASH-2 and WOMAN trial [6].
Clinical Bottom Line: In trauma patients, requiring blood products (i.e. massive transfusion protocol), the use of TXA as a 1g bolus given over 10 minutes, followed by 1g over 8hrs, in ≤3 hours from time of injury, reduces all-cause mortality without an increase in thromboembolic events.
TBI
Meta-Analysis of TXA for Traumatic Brain Injury [3]
What They Did:
- This was a meta-analysis and systematic review of RCTs or quasi-RCTs comparing TXA vs placebo in patients with TBI and evaluating their outcomes.
Outcomes:
- The main outcomes of interest included mortality, neurological function, hematoma expansion, and adverse effects all of which are patient oriented outcomes.
Results:
- Two high-quality RCTs with, 510 patients having TBI, met inclusion criteria for this review.TXAs effect on the outcomes mentioned above were as follows:

- No serious adverse effects were associated with TXA
Strengths:
- Both trials included in this meta-analysis were high quality of evidence (i.e. double blinded, intention-to-treat analysis, randomized, and >92% follow-up)
Limitations:
- The largest limitation of this meta-analysis and systematic review is the fact that only 2 RCTs could be found and that neither of these was adequately powered to detect clinical outcomes. Secondly, patients enrolled from CRASH-2 had significant extracranial injuries and not just isolated TBIs. Therefore, it is feasible that the trend toward mortality benefit with TBI could be due to improvement in hemorrhage control from the extracranial injuries and not from the improving intracranial hematoma expansion.
Author Conclusion:“Pooled results from the two RCTs demonstrated statistically significant reduction in intracranial hemorrhage progression with TXA and a non-statistically significant improvement of clinical outcomes in ED patients with TBI. Further evidence is required to support its routine use in patients with TBI.”
Clinical Take Home Point: The results of this study should be evaluated carefully as there was a statistically significant decrease in intracranial hematoma expansion, this did not lead to a statistically significant mortality benefit or improved neurological functional status.
Tranexamic Acid for Hyperacute Primary IntraCerebral Haemorrhage (TICH-2) [4]
What They Did: This was an international, randomized, double-blind, placebo-controlled, parallel group, phase 3 trial of adults with intracranial hemorrhage from acute stroke across 124 hospitals (12 countries). Patient were randomized in a 1:1 fashion to receive either 1g IV TXA bolus followed by an 8hr infusion of 1g of TXA or a matching placebo within 8 hours of symptom onset.
- Intervention: 1g TXA in 100mL of NS infused over 10min followed by another 1g in 250mL of NS infused over 8hrs
- Placebo: 100mL of NS infused over 10min followed by another 250mL of NS infused over 8hrs
Outcomes:
- Primary: Functional status at day 90, defined as an ordinal shift in the modified Rankin Scale (mRS)
- Secondary:
- Neurological impairment at day 7 or discharge (whichever came first) assessed by NIHSS
- Activities of daily living according to the Barthel index
- Costs including length of hospital stay
- Change in hematoma volume from baseline to 24hrs
- Safety outcomes up to day 90
- Death
- VTE
- Ischemic events (Stroke, TIA, MI, ACS, PAD)
- Seizures
Inclusion:
- Adults with ICH
- Admitted to a participating hospital within 8hrs of stroke symptom onset (or time last seen well)
Exclusion:
- ICH secondary to anticoagulation, thrombolysis, trauma, or known underlying structural abnormality
- Contraindication to TXA
- Prestroke dependence (mRS >4)
- Life expectancy <3 months
- GCS <5
Results:
- 2325 patients enrolled
- 1161 randomized to TXA
- 1150 received intervention
- 1152 analyzed at day 90 ITT analysis
- 1164 randomized to placebo
- 1157 received
- 1155 analyzed at day 90 ITT analysis
- Median time from stroke onset to randomization = 3.6hrs
- Median time from randomization to treatment = 21min
- 36% of patients recruited within 3hrs
- 1161 randomized to TXA
- Primary Outcome: Functional Status at Day 90:
- No difference between groups
- aOR 0.88; 95% CI 0.76 – 1.03; p = 0.11
- No difference when mRS dichotomized at mRS 0-3 vs 4-6 (aOR 0.82; 95% CI 0.65 – 1.03), p=0.08).
- Hematoma Expansion at Day 2
- TXA: 25%
- Placebo: 29%
- aOR 0.80; 95% CI 0.66 – 0.98; p = 0.0300
- Mean Hematoma Volume Expansion from Baseline to 24hr (mL)
- TXA: 3.72
- Placebo 4.90
- Adjusted mean difference -137mL; 95% CI -2.71 – -0.04; p = 0.0432
- Death by Day 7
- TXA: 9%
- Placebo 11%
- OR 0.73; 95% CI 0.53 – 0.99; p = 0.0406
- Death by Day 90
- TXA: 22%
- Placebo 21%
- HR 0.92; 95% CI 0.77 – 1.10; p = 0.37
- No difference in neurological impairment (mean NIHSS score at day 7), 90-day functional outcomes, length of hospital stay, discharge disposition, venous thromboembolic events, or arterial occlusions
Strengths:
- Asks a clinically important question
- Multicenter, international, randomized, double-blind, placebo-controlled, parallel group trial. All the things we like to see in a trial.
- Treatment allocation was concealed from patients, outcome assessors, and all other health-care workers involved in the trial
- Pre-specified secondary and safety outcomes prior to start of the trial
- Groups were balanced in baseline characteristics
- High protocol adherence of 95% receiving all of the randomized treatment
- Broad inclusion criteria which increases generalizability into practice
Limitations:
- Screening logs were not collected therefore no data on eligibility
- Wide inclusion criteria also led to a heterogenous population with more severe strokes, larger hematoma volumes and a greater proportion of lobar hematomas and intraventricular hemorrhage which may have diluted any potential treatment effect
- Most patients were enrolled >3hrs after the onset of ICH, which may be another reason why no benefit was seen with TXA, as previous studies in trauma have shown that TXA prior to 3 hours is required for mortality improvement
Discussion:
- Some major reasons why this trial didn’t show any benefit:
- Although it has been shown in the trauma literature that ≤3 hours is an important window period for the effectiveness of TXA, this trial chose to use 8hrs as their treatment window to maintain consistency with prior trials of TXA in traumatic ICH. Future trials should target a window of <3hrs, which is the window in which most hematoma growth occurs.
- Broad inclusion criteria are great from a generalizability standpoint, but ultimately ended up being a major limitation in this study. Future trials should consider excluding patients with non-survivable ICH or who won’t clinically benefit from further hematoma growth
- Although there was no difference in the primary outcome, there may be some signal in all the noise. There were reductions in early death by day 7 and hematoma expansion, but both of these should be taken as hypothesis generating at this time
- I have never understood the fear of venous thromboembolism with TXA as this is an anti-fibrinolytic agent not a prothrombotic agent. This study once again shows no increase in VTEs in the TXA group.
- An important point is patients with SBP ≤170mmHg did better than patients with SBP >170mmHg. Blood pressure lowering has been the only intervention to date to improve functional outcomes in patients with ICH, therefore early blood pressure control is a key factor to improve patient outcomes
Author Conclusion: “Functional status 90 days after intracerebral haemorrhage did not differ significantly between patients who received tranexamic acid and those who received placebo, despite a reduction in early deaths and serious adverse events. Larger randomized trials are needed to confirm or refute a clinically significant treatment effect.”
Clinical Take Home Point: In this trial TXA was given >3hrs after stroke onset, patients had more severe strokes, and larger hematoma volumes (>60mLs) than prior studies and therefore there is no surprise in the fact that there was no difference in 90-day functional outcomes in patients with spontaneous ICH receiving TXA compared to placebo.
Clinical Bottom Line:TXA cannot be recommended at this time in clinical practice for spontaneous ICH based on the results of these trials, however some hypothesis generating outcomes included reductions in early death by day 7 and hematoma expansion, and hopefully future research will try and answer these questions.
PPH
WOMAN Trial [5]
What They Did:
- Randomized, double-blind, placebo-controlled trial, of women ≥16 years of age with post-partum hemorrhage after vaginal delivery or caesarean section from 193 hospitals in 21 countries
- Randomized to TXA 1g IV vs matching placebo
- If bleeding continued after 30 minutes or stopped and restarted within 24hrs, a second dose of 1g of TXA or placebo was given
Outcomes:
- Original Primary: Composite outcome of all-cause mortality and/or hysterectomy within 42 days of giving birth
- Final Primary Outcome: Death from PPH
Exclusion:
- Clinician was certain that TXA would either be beneficial or not appropriate
Results:
- 20,060 women randomized
- TXA arm: 10,036 included in analysis
- Placebo arm: 9,985 included in analysis

Strengths:
- Large, multicenter, multinational trial
- Participants, care givers, and those assessing outcomes blinded to allocation
- 74% follow up
- Pharma (Pfizer) did help fund the study but had no role in study design, data collection, data analysis, data interpretation or writing of the final manuscript
Limitations:
- Patients were enrolled in the study if clinicians were uncertain if they would benefit from TXA.This could underestimate the benefit of tXA in PPH
- Primary endpoint was altered after initiation of the trial
- Diagnosis of PPH made clinically and no assessment of inter-rater reliability in making this determination
Discussion:
- Primary endpoint was changed during the study. The investigators learned that the decision to perform a hysterectomy was most commonly made at the time of randomization, and thus, could not be affected by the intervention. However, the change in the primary endpoint was performed prior to any data analysis or unmasking of data
- As with the CRASH-2 study, the data showed a consistent association of delayed administration of TXA with no benefit
Author Conclusion: “Tranexamic acid reduces death due to bleeding in women with post-partum haemorrhage with no adverse effects. When used as a treatment for postpartum haemorrhage, tranexamic acid should be given as soon as possible aftr bleeding onset.”
Clinical Take Home Point:TXA may or may not be beneficial in preventing death from bleeding in patients with PPH without increasing the risk of VTE. It is difficult to draw definitive conclusions from this trial as the NNT was still large (i.e. ≈250) and the study had a fragility index of 0.
Meta-Analysis of CRASH-2 and WOMAN Trial [6]
What They Did:
- This was an individual patient-level data meta-analysis of 2 randomized trials done with more than 1000 patients each that assessed the effects of antifibrinolytics in acute severe bleeding.
Outcomes:
- The primary outcome was absence of death from bleeding and secondary outcomes of vascular occlusive fatal and non-fatal events (MI, stroke, PE, and DVT).
Inclusion:
- The authors randomized placebo-controlled trials done with more than 1000 patients that assessed the effects of antifibrinolytics in acute severe bleeding
Exclusion:
- Trials were excluded if they were ongoing trials without complete data or were not a randomized placebo-controlled trial with >1000 patients
Results:
- 40,138 patients from two randomized trials of TXA in acute severe bleeding (traumatic and post-partum hemorrhage) were included in the analysis. The CRASH-2 (Trauma) Trial with 20,127 patients and the WOMAN (Post-partum hemorrhage) Trial with 20,011 patients. In total there were 3,558 total deaths in both studies. 1,408 (40%) of deaths were due to bleeding and 884 of these deaths (63%) occurred within 12 hours of onset.
- TXA Increased Overall Survival form Bleeding:
- TXA: 96.6%
- Placebo: 96.0%
- ARR: 0.6%
- NNT = 167
- OR 1.20; 95% CI 1.08 – 1.33; p = 0.001
- No Increase in Vascular Occlusive Events with TXA:
- TXA: 0.2%
- Placebo: 0.3%
- OR 0.73; 95% CI 0.49 – 1.09
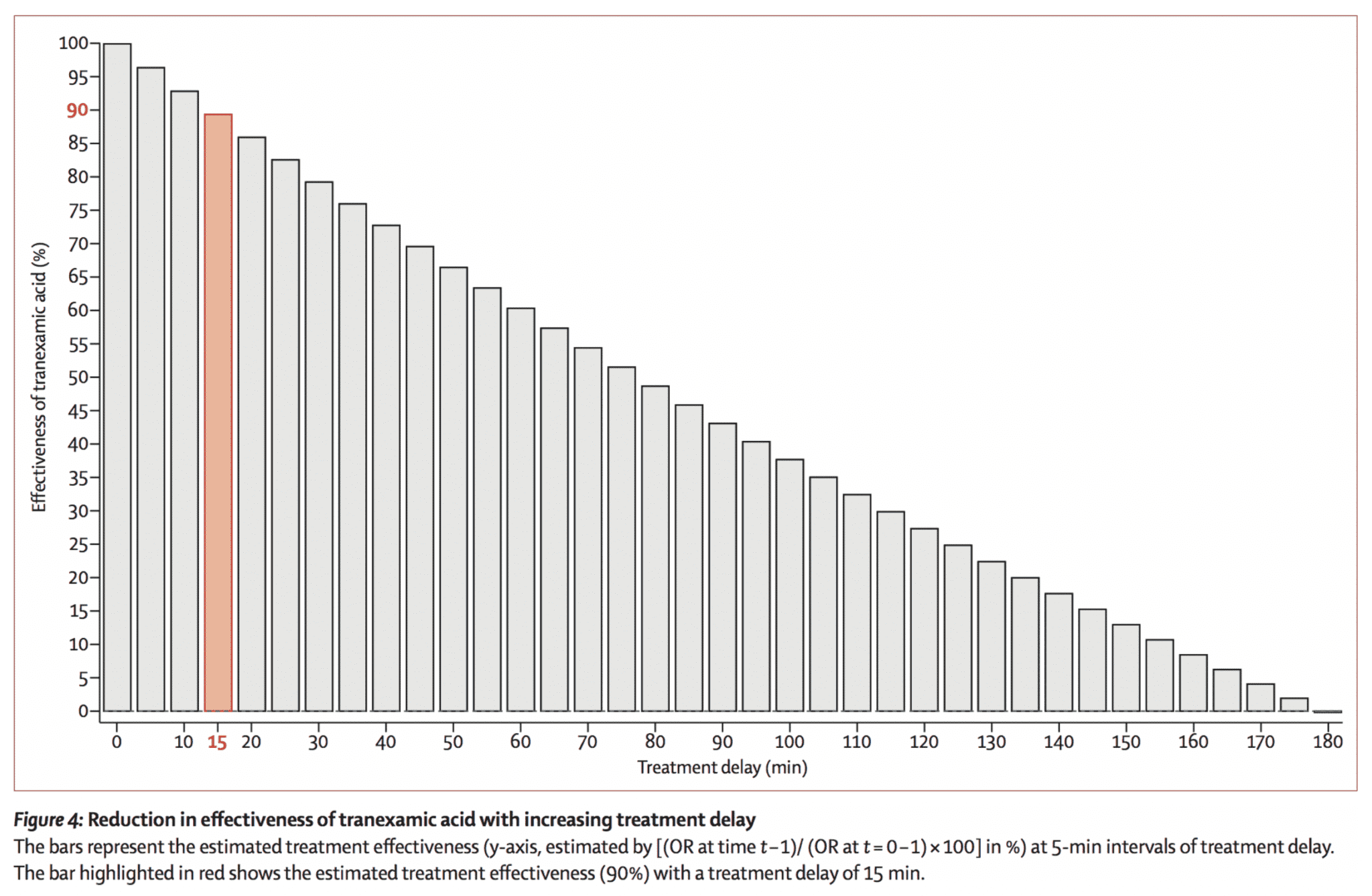
- Effect of Treatment Delay on Survival:

Survival Benefit Decreased by 10% for Every 15min of Treatment Delay Until 3hr, After Which There was NO BENEFIT
Strengths:
- The biggest strengths of this meta-analysis were the inclusion of high-quality placebo controlled, RCTs that had over 1000 patients which helped reduce selection bias and the primary outcome, which was death due to bleeding and not all-cause mortality, as antifibrinolytics would not affect other causes of death.
Limitations:
- The biggest limitation in both of these trials was the exact onset of bleeding was really unknown. In CRASH-2 this may have underestimated the effectiveness of TXA and in WOMAN this may have potentially overestimated the effectiveness of TXA as time of birth was used as the onset of bleeding.
Discussion:
- The authors of this paper also evaluated the relative treatment benefit observed by 60-minute intervals of treatment delay from time of onset of bleeding. There appears to be no additional benefit when TXA was given in the first hour, but it also important to mention that a higher proportion of penetrating injuries are seen and treated in this time period, and many of them may have been unsurvivable injuries, therefore making the effect seem non-beneficial during this hour.
Author Conclusion: “Death from bleeding occurs soon after onset and even a short delay in treatment reduces the benefit of tranexamic acid administration. Patients must be treated immediately. Further research is needed to deepen our understanding of the mechanism of action of tranexamic acid.”
Clinical Take Home Point: In patients with massive bleeding from trauma or post-partum hemorrhage, giving TXA as soon as bleeding is suspected, reduces mortality from bleeding. Most deaths, in trauma and postpartum, from hemorrhage, occur within hours of bleeding onset. The mortality benefit of TXA appears to diminish over time and is lost at 3 hours after major hemorrhage begins. In this trial, there was no evidence of adverse effects (vascular occlusive events) associated with TXA treatment.
GIB
TXA for GIB Cochrane Review [7]
What They Did:
- Systematic review and meta-analysis of trials using TXA vs no intervention, placebo, or other antiulcer drugs for upper GIB
Outcomes:
- Primary: all-cause mortality and adverse events
- Secondary: Rebleeding and surgery
Inclusion:
- Randomized, parallel-arm, controlled trials with suspected or endoscopically verified upper GIB, irrespective of the bleeding source
Exclusion:
- Previous or ongoing thromboembolic disease
- Chronic kidney disease
- Pregnant patients
Results:
- 8 RCTs
- 7 trials vs placebo
- 1 trial vs no intervention
- 2 trials vs antiulcer drugs
- All-Cause Mortality (8 trials with 1700 pts):
- TXA: 42/851 (4.9%)
- Placebo: 71/850 (8.4%)
- RR 0.60
- 95% I 0.42 – 0.87
- P = 0.007
- Rebleeding (7 trials with 1650 pts):
- TXA: 117/826 (14.2%)
- Placebo: 146/825 (17.7%)
- RR 0.80
- 95% CI 0.64 – 1.00
- P = 0.07
- No difference in thromboembolic events (only evaluated in 4 trials)
Strengths:
- Contacted study investigators to request missing data
- Assessed clinical and statistical heterogeneity
- Included admitted patients with suspected upper GIB confirmed by endoscopy or clinically through gastric lavage, hematemesis or melena
- 7 out of 8 trials were double blind with a placebo control
Limitations:
- Many patients assigned to randomization were subsequently excluded in some studies (5 out of 8 trials). This will lead to an attrition bias, making the current overall quality of evidence as moderate to low.
- Trials included were small (i.e. Range: 47 – 204 patients) making it difficult to draw absolute conclusions and overall the median number of patients per study was 204 patients)
- Only three trials included participants with “severe” bleeding which may underestimate the total effect size of TXA, as 5 studies were in patients without “severe” bleeding
- One trial administered TXA as IV only, 3 trials administered TXA PO, and remaining trials administered TXA IV followed by PO administration
- Total daily dose of TXA ranged from 4 – 8g and ranged from 2 – 7 days, which is not realistic of what happens in an acute emergency setting
- Only 2 trials used endoscopic therapy as treatment for upper GIB. In these trials there was no clear benefit on bleeding.
- In several trials variceal bleeding was an exclusion criterion, making it difficult to draw strong conclusions in this patient population
Discussion:
- Currently, the HALT-IT trial is underway which will be a RCT of 12,000 patients with upper GIB comparing TXA 1g IV vs placebo, followed by 3g TXA infused over 24hrs vs placebo infusion
- Transfusion requirements could not be studied as the necessary data required could not be identified
- One reason we may see a mortality benefit and no benefit in bleeding is that TXA may only be beneficial in patients with “severe” bleeding and not all upper GIB patients
Author Conclusion: “This review found that tranexamic acid appears to have a beneficial effect on mortality, but a high dropout rate in some trials means that we cannot be sure of this until the findings of additional research are published.”
Clinical Take Home Point: Based on the best available evidence, it appears that TXA in upper GIB may benefit mortality in the sickest patients. (i.e. massive bleeding, hemodynamic compromise, patients requiring blood transfusions, etc…). Further high-quality evidence is required to confirm or refute these findings.
Epistaxis
Zahed et al 2017 [8]
What They Did:
- This study was a randomized, parallel group clinical trial conducted out of 2 emergency departments. A total of 124 patients taking antiplatelet drugs (Aspirin, clopidogrel or both) were randomized to receive topical TXA (500mg in 5mL) or anterior nasal packing.
Outcomes:
- The primary outcome of interest was the proportion of patients whose bleeding stopped at 10 minutes. Secondary outcomes were re-bleeding rate at 24hours and one week, ED length of stay, and patient satisfaction.
Inclusion: patients were eligible for inclusion if they had an acute anterior nosebleed and taking antiplatelet drugs.
Exclusion: Patients were excluded if the cause of their epistaxis was traumatic, on anticoagulation, had inherited bleeding disorders, inherited platelet disorders, and INR >1.5, shock, a visible bleeding vessel, a history of renal disease, and lack of consent.
Results: A total of 384 patients were assessed for eligibility, but 260 patients were excluded leaving only 124 patients available for analysis. 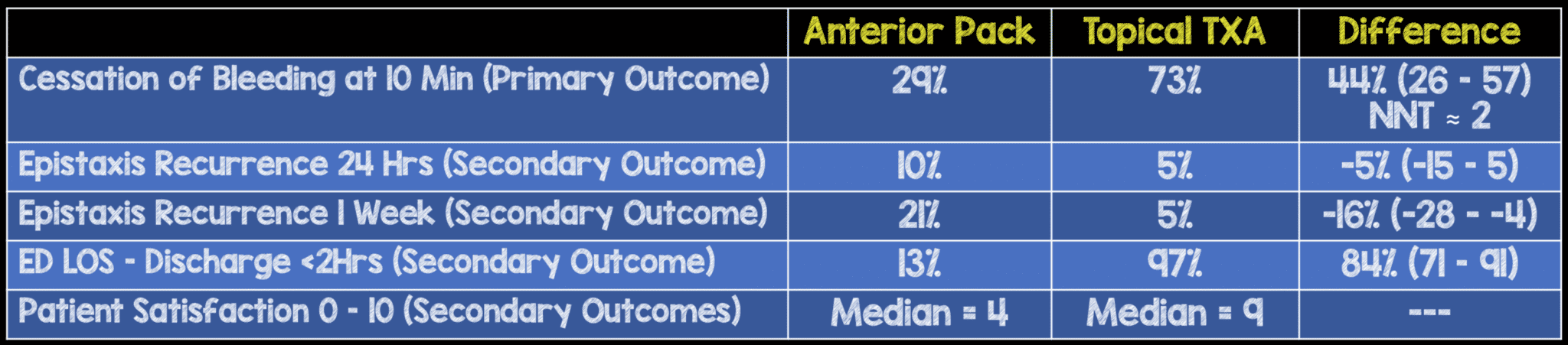
Strengths: Outcome assessors were blinded to treatment allocation
Limitations: Patients with posterior epistaxis were not included in this trial, so no comments can be made about the use of TXA in these patients based on this study.
Discussion: In patients with anterior epistaxis, I generally have them blow out the clots from their nose, put two sprays of afrin into the affected nostril, place a TXA soaked pledget (500mg in 5mL), and then use a nose clip or direct compression for 10 – 15 minutes. All of these interventions are simple and inexpensive.
Author Conclusion:“In our study population, epistaxis treatment with topical application of TXA resulted in faster bleeding cessation, less re-bleeding at 1-week, shorter ED LOS, and higher patient satisfaction as compared with anterior nasal packing.”
Clinical Take Home Point: Based on this trial, the use of topical TXA appears to be superior to anterior nasal packing for cessation of bleeding at 10 minutes (primary outcome), ED length of stay, and patient satisfaction.
Post-Tonsillectomy Bleeding
Meta-Analysis 2012 [11]:
What They Did:
- Systematic review and meta-analysis to evaluate the role of TXA in tonsillectomy
Outcomes:
- Total blood loss (intra-operative and post-operative)
- Number of patients with post-operative hemorrhage
- Severity and duration of hemorrhage
- Number of patients requiring further interventions (either medical or surgical)
Inclusion:
- Studies using TXA for tonsillectomy during the pre-operative, peri-operative, and post-operative time period
- Observational or randomized controlled trial design
Exclusion:
- Studies without a control or placebo group
- Patients <2 years old
- Patients with hemorrhagic disorders
- Patients with adenotonsillectomy due to difficulty in assessing additional blood loss during adenoidectomy specifically
Results:
- 7 studies with 2,444 patients
- 3 RCTs
- 4 Case control trials
- 2 studies (180 patients) evaluated mean volume of blood loss
- TXA decreased mean volume blood loss by 32.72mL when compared to control group
- 95% CI -42.66 to -22.78
- P <0.00001
- 5 studies (1,670 patients) evaluated number of patients with post-tonsillectomy hemorrhage
- TXA did not reduce the risk of post-tonsillectomy bleeding
- RR 0.51
- 95% CI 0.25 – 1.07
- P = 0.08
- 1 study with 40 patients evaluated duration of hemorrhage after tonsillectomy
- Mean duration of bleeding was significantly less with TXA when compared to control by 3.6hrs
- 4 studies reported adverse effects, and none were found in patients treated with TXA
Strengths:
- 1stsystematic review and meta-analysis on the use of TXA in tonsillectomy patients
- Included studies with appropriate control and study groups
- Data extracted and collected by two independent reviewers to ensure inter-rater agreement in data
- Completed methodological quality assessment of all trials
Limitations:
- Most studies conducted and published from 1970 – 1980
- Included studies without lack of blinding
- Application of TXA varied in dosage, mode of delivery, and timing of administration making it difficult to identify one optimal dosing option in patients with post-tonsillectomy bleeding
- None of these studies applied TXA in the post-operative period (All studies investigated the prophylactic effects of TXA in tonsillectomy patients, rather than therapeutic effects)
- Significant heterogeneity of studies due to differing inclusion and exclusion criteria, therefore different populations of patients included in each trial
Discussion:
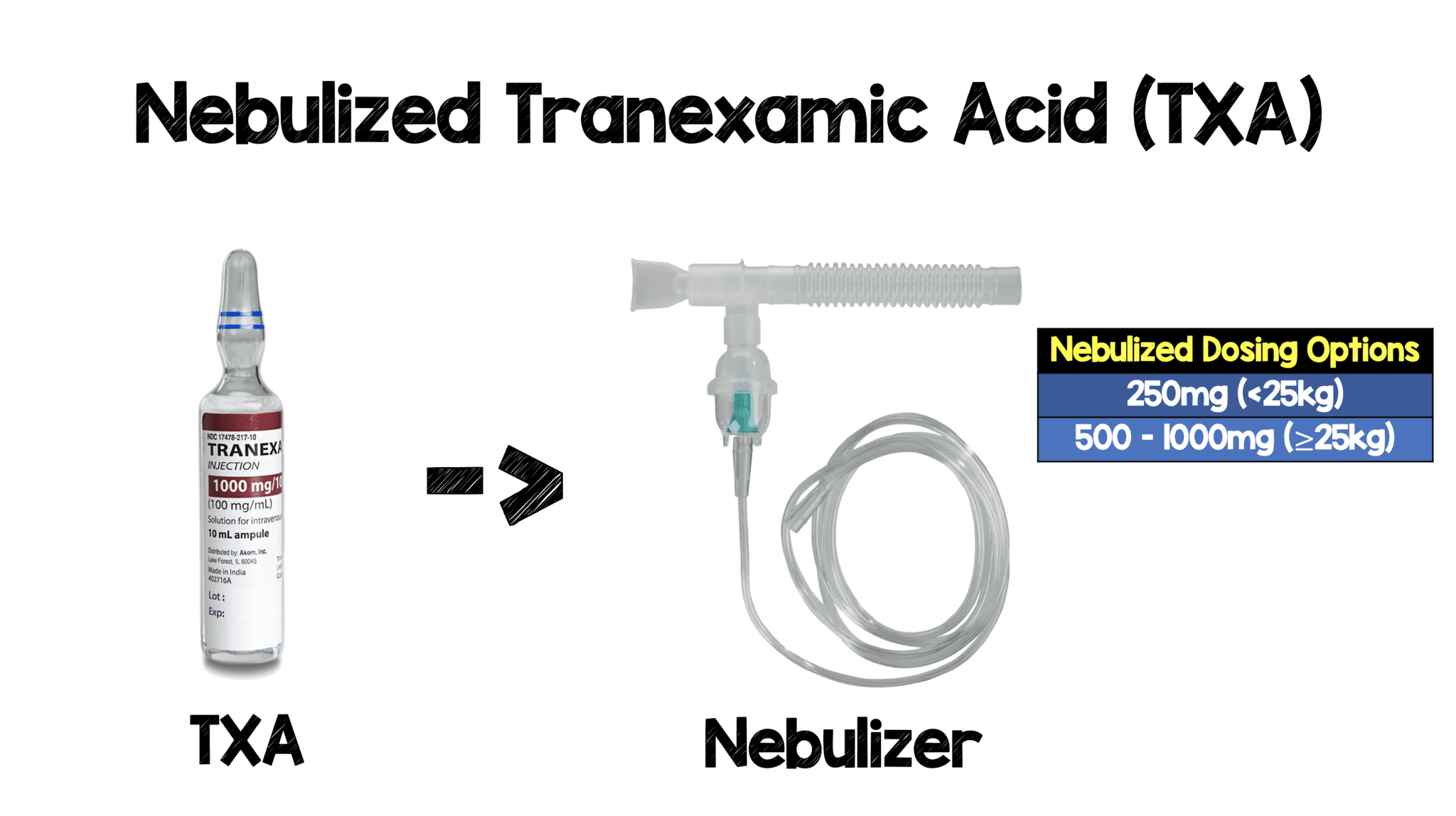
- Specifically evaluating the post-operative tonsillectomy patients, the routes of administration and dosages varied, and only one study evaluated topical application (4% TXA Topical Solution Applied for 4min). In my practice I am nebulizing 500mg of TXA (based off hemoptysis data)
- Reviewing the literature, a single pediatric case report was found extrapolating nebulized tranexamic acid from diffuse alveolar hemorrhage studies. The dosing is 250mg for children <25kg, 500mg for children >25kg [12]
Author Conclusion: “TXA led to a significant reduction of tonsillectomy blood loss volume but had no impact on the rate of patients with post-tonsillectomy haemorrhage.”
Clinical Take Home Point: In patients with minor post-tonsillectomy bleeding consider using nebulized TXA to reduce or stop bleeding. Exsanguinating patients not enrolled in these studies, although fairly uncommon, therefore difficult to draw conclusions in this patient population.
Hemoptysis
Case Report of Inhaled Tranexamic Acid 2018 [13]
What They Did:
- This was a case report of a patient with massive hemoptysis treated with nebulized TXA in the ED. Also, in this paper the evidence for nebulized TXA in hemoptysis is discussed. Unfortunately, by evidence we mean case reports and case series. The main outcome of concern is cessation of hemoptysis. Patients with massive hemoptysis (defined as >200cc over a 24hr period) were included in this discussion
Results:
- There are 14 individual cases of hemoptysis discussed in this paper.
- The typical dosing for hemoptysis ranged from 250mg – 500mg of nebulized TXA 2 – 4x/day up to 1000mg of nebulized TXA x1
- The time to resolution of hemoptysis also was a range from a few minutes to <72hrs
- <30min: 7 Cases
- 1 – 6hrs: 2 Cases
- 7 – 24hrs: 2 Cases
- 25 – 72hrs: 3 Cases

- Adverse outcomes: 1 patient had bronchospasm, which was successfully treated with bronchodilators
Author Conclusion: “In massive hemoptysis, rapidly available nebulized TXA may be considered a therapeutic option, serving either as primary therapy or as a bridge until other definitive therapies can be arranged.”
Clinical Take Home Point: Nebulized TXA at a dose of 250mg – 1000mg either as a straight drug or diluted in 20cc of NS, could potentially be a bridge to stop or slow down hemoptysis until definitive therapy can be carried out. Again, just as with post-tonsillectomy bleeding, patients with airway compromise or massive bleeding were not included in this analysis. In these patients, intubation with bronchoscopy will be definitive therapy.
Inhaled TXA RCT 2018 [14]:
What They Did:
- Prospective, double-blind, placebo-controlled randomized controlled trial assessing the effectiveness of nebulized TXA (500mg/5mL TID) vs placebo (5mL of 0.9% normal saline) for treatment of non-massive hemoptysis
Outcomes:
- Primary:
- Rate of complete resolution of hemoptysis during first 5 days from admission
- Difference in daily volume of expectorated blood
- Secondary:
- Rate of interventional bronchoscopy
- Rate of angiographic embolization
- Rate of surgery
- Mean hospital LOS
- Safety Outcome:
- Rate of side effects
- Follow Up Outcomes (30d and 1 year)
- Mortality
- Recurrence rate of hemoptysis
Inclusion:
- Adult patients (≥18 years of age) admitted with hemoptysis over previous 24 hours
Exclusion:
- Massive hemoptysis (Expectorated blood >200mL/24hr)
- Hemodynamic instability
- Respiratory instability
- Pregnancy
- Renal failure (Cr Level > 3mg/dL or need for RRT)
- Hepatic failure (Bilirubin >2mg/dL or AST > 3x upper limit of normal)
- Coagulopathy (INR > 2)
- Known hypersensitivity to TXA
- Treatment with TXA prior to screening
Results:
- 47 patients randomized
- 25 patients received nebulized TXA
- 22 patients received nebulized normal saline
- 36% (9pts) and 41% (9pts) had lung malignancy in the TXA group and placebo group respectively
- >50% of patients were treated with anticoagulants or antiplatelet medications as outpatients
- Resolution of hemoptysis within 5 days of admission
- TXA: 96%
- Placebo: 50%
- ARR = 46%
- NNT = 2
- P<0.0005
- Quantity of expectorated blood was significantly reduced by day 2 of admission (≈50cc/24hr vs 15cc/24hrs)
- Mean Hospital Length of Stay
- TXA: 5.7 +/- 2.5d
- Placebo 7.8 +/- 4.6d
- P = 0.046
- Requiring Invasive Procedures (i.e. Bronchoscopy or Angiographic Embolization) to Control Bleeding:
- TXA: 0%
- Placebo 18.2%
- P = 0.041
- No surgical procedures were required in either group
- No side effects in either group including bronchospasm
- Long-Term Follow Up:
- Mortality at 30d:
- TXA: 0%
- Placebo: 10%
- P = 0.21
- Recurrent Hemoptysis at 30d:
- TXA: 8%
- Placebo 27.3%
- P = 0.12
- Mortality at 30d:
Strengths:
- 1st prospective RCT to assess the effectiveness of nebulized tranexamic acid in patients with hemoptysis
- Both treatment and placebo were prepared in pharmacy and provided to pulmonary department in identical unmarked vials, to allow blinding of the treating team and patients
- Patients collected expectorated blood in measuring cups daily during the trial to measure the amount of bleeding, instead of subjectively quantifying the amount of bleeding
- Patients were balanced in baseline clinical characteristics and causes of hemoptysis
Limitations:
- Hemodynamic and respiratory instability not clearly defined
- Massive hemoptysis (>200cc/hr) were excluded
- Small number of patients does not allow specific assessment of nebulized TXA in different subpopulations of hemoptysis (i.e.anticoagulant therapy)
Discussion:
- Study required 60 patients to have statistical significance and fell short of this with 47 patients randomized. This was due to an internal analysis showing perceived superiority of inhaled TXA to placebo after successful recruitment of 47 patients
- The main advantage of inhaled TXA vs systemic TXA in hemoptysis, is a more rapid onset of action at the site of bleeding
- There is also a Cochrane review from 2016 [15], however it only included 2 RCTs (one from 2002 and one from 1994). The 2002 trial evaluated oral TXA and the 1994 trial evaluated IV TXA. The pooled results did show a reduction in bleeding time in patients receiving TXA vs placebo, but with significant heterogeneity
Author Conclusion: “TA inhalations can be used safely and effectively to control bleeding in patients with nonmassive hemoptysis.”
Clinical Take Home Point: Although this was a small study, the advantages of inhaled TXA vs placebo in patients with non-massive hemoptysis (<200mL/24hrs) included faster resolution of hemoptysis, shorter hospital LOS, fewer invasive procedures, and although not statistically significant, a trend toward improved 30d mortality.
How Do You Nebulize TXA?
TXA Clinical Bottom Line

References:
- Morrison JJ et al. Military Application of Tranexamic Acid in Trauma Emergency Resuscitation (MATTERs) Study. Arch Surg 2012. PMID: 22006852
- Shakur H et al. Effects of Tranexamic Acid on Death, Vascular Occlusive Events, and Blood Transfusion in Trauma Patients with Significant Haemorrhage. Lancet 2010. PMID: 20554319
- Zehtabchi S et al. Tranexamic Acid for Traumatic Brain Injury: A Systematic Review and Meta-Analysis. Am J Emerg Med 2014. PMID: 25447601
- Sprigg N et al. Tranexamic Acid for Hyperacute Primary IntraCerebral Haemorrhage (TICH-2): An International Randomised, Placebo-Controlled, Phase 3 Superiority Trial. Lancet 2018. PMID: 29778325
- WOMAN Trial Collaborators. Effect of Early Tranexamic Acid Administration on Mortality, Hysterectomy, and Other Morbidities in Women with Post-Partum Haemorrhage (WOMAN): An International, Randomised, Double-Blind, Placebo-Controlled Trial. Lancet 2017. PMID: 28456509
- Gayet-Ageron A et al. Effect of Treatment delay on the Effectiveness and Safety of Antifibrinolytics in Acute Severe Haemorrhage: A Meta-Analysis of Individual Patient-Level Data From 40138 Bleeding Patients. Lancet 2017. PMID: 29126600
- Bennett C et al. Tranexamic Acid for Upper Gastrointestinal Bleeding (Review). Cochrane Database Syst Rev 2014. PMID: 25414987
- Zahed R et al. Topical Tranexamic Acid Compared With Anterior Nasal Packing or Treatment of Epistaxis in Patients Taking Antiplatelet Drugs: Randomized Controlled Trial. Acad Emerg Med 2017. PMID: 29125679
- Joseph J et al. Tranexamic Acid for Patients with Nasal Haemorrhage (epistaxis) (Review). Cochrane Database Syst Rev 2018. PMID: 30596479
- Chan CC et al. Systematic Review and Meta-Analysis of the Use of Tranexamic Acid in Tonsillectomy. Eur Arch Otorhinolaryngol 2013. PMID: 22996082
- Prutsky G et al. Antifibrinolytic Therapy to Reduce Haemoptysis from any Cause (Review). Cochrane Database Syst Rev 2012. PMID: 22513965
- Schwarz W et al. Nebulized Tranexamic Acid Use for Pediatric Secondary Post-Tonsillectomy Hemorrhage. Ann Emerg Med 2019. PMID: 30292524
- Komura S et al. Hemoptysis? Try Inhaled Tranexamic Acid. JEM 2018. PMID: 29502864
- Wand O et al. Inhaled Tranexamic Acid for Hemoptysis Treatment: A Randomized Controlled Trial. Chest 2018. PMID: 30321510
- Prutsky G et al. Antifibrinolytic Therapy to Reduce Haemoptysis from any Cause (Review). Cochrane Database Syst Rev 2016. PMID: 22513965
For More Thoughts on This Topic Checkout:
- emDOCs: TXA MATTERS!
- PharmERToxGuy: Nebulized Tranexamic Acid (TXA) for Acute Treatment of Stable Hemoptysis
- REBEL EM: It’s Time for Tranexamic Acid (TXA) in Massive Hemorrhage
Support the Show by Paying & Claiming 0.75hrs of CME/CEH by Clicking on the Logo Below

Post Peer Reviewed By: Anand Swaminathan, MD (Twitter: @EMSwami)




