
Authors: Ryan Sumpter, MD (Uniformed Services University, Bethesda, MD), Rachel Bridwell, MD (@rebridwell, EM Resident Physician, San Antonio, TX) // Reviewed by: Brit Long, MD(@long_brit, EM Attending Physician, San Antonio, TX); Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UTSW / Parkland Memorial Hospital)
Welcome to EM@3AM, an emDOCs series designed to foster your working knowledge by providing an expedited review of clinical basics. We’ll keep it short, while you keep that EM brain sharp.
A 45-year-old male presents to the ED for worsening, severe oral pain and acute bleeding of his gums. He says he thinks his breath smells worse than normal. He has HIV and is non-compliant on HAART.
Exam reveals BP 127/90, HR 110, RR 16, T 101.7 F temporal, SaO2 98% on room air. He is uncomfortable appearing, not wanting to move his mouth or speak, but maintaining his airway.
You note halitosis, gingival bleeding, increased mobility of the front lower teeth, ulcerated “punched out” lesions along the interdental papillae, and anterior cervical lymphadenopathy. Social history is notable for IVDU.
What’s the next step in your evaluation and treatment?
Answer: Acute Necrotizing Ulcerative Gingivitis (ANUG)1-12
Epidemiology:
- Historically known as Vincent’s Angina or Trench Mouth.
- Trench mouth originating from the higher reported incidence of ANUG among young soldiers in the trenches on the western front during WWI.
- Combination of poor oral hygiene, intense psychological stress, and malnutrition all are contributing factors.1
- Relatively rare clinical entity in more developed countries.
- Scarce data regarding incidence of disease in general population; however, limited data suggest increased rates of approximately 30 cases per 1000 person years in immunocompromised groups.2
- Immunocompromised (cancer, HIV, etc.) at higher risk.
- Most important predisposing factor is HIV.3
- Increased risk with decreasing CD4 counts.4
- Data suggest decreased function in neutrophil chemotaxis and phagocytosis may be important in pathogenesis of ANUG.5,6
- Populations include patients with Leukocyte Adhesion Deficiency, Chronic Granulomatous Disease, Localized Juvenile Periodontitis, and AIDS.
- Most important predisposing factor is HIV.3
- Risk factors include:3,7
- Poor oral hygiene/nutrition/sleep, increased stress
- EtOH and tobacco use
- Increased rates in Caucasians and individuals age less than 21.
- Observational studies have suggested seasonal variation in patients presenting with ANUG most commonly in summer.
- 4% of ANUG patients presenting during the summer, 27.7% in the fall, and 8.4% during both winter and spring.7
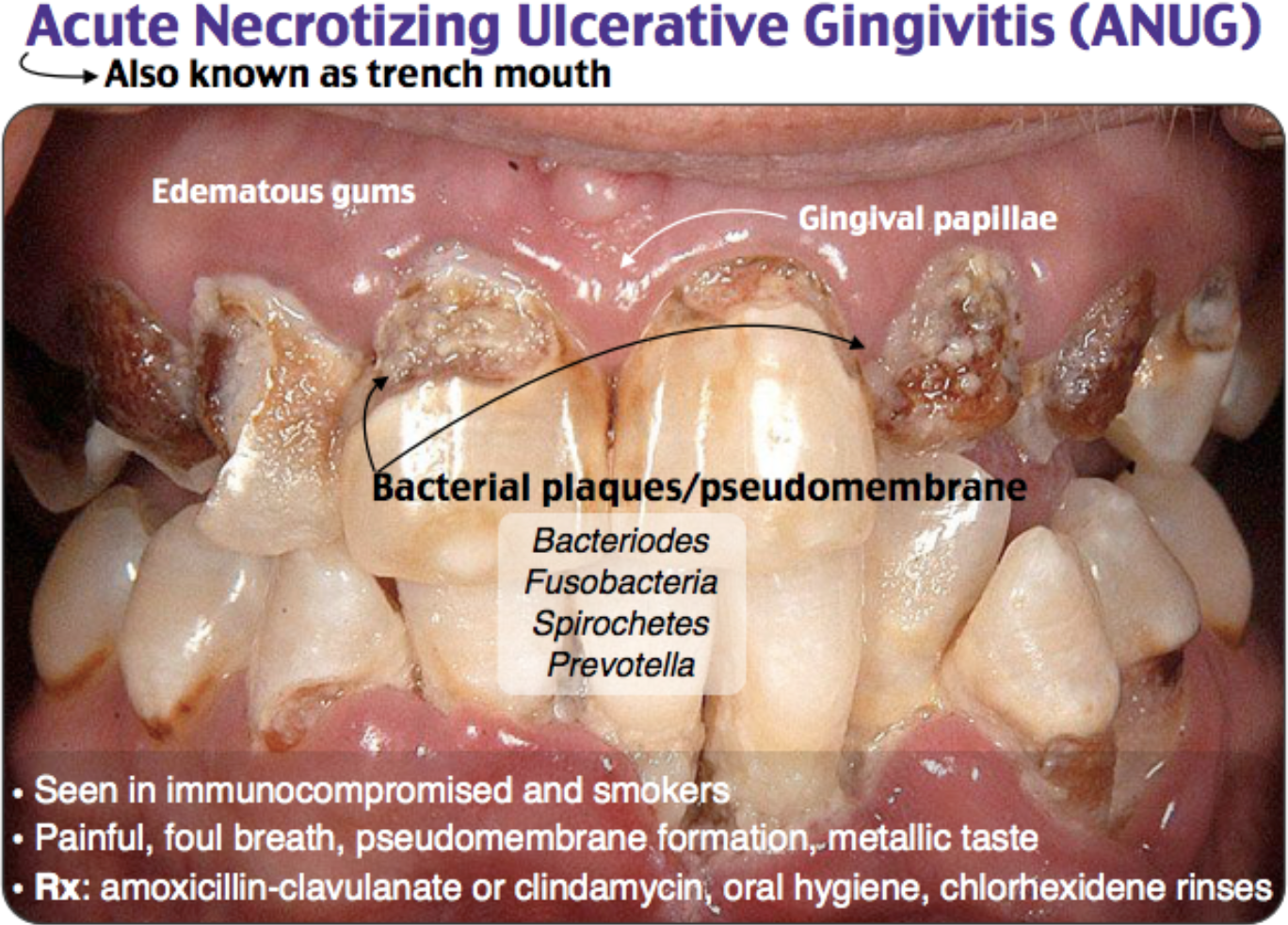
- Often polymicrobial, but most common causative organisms: Prevotella, Fusobacterium species, Tannerella forsythia, Treponema denticoli, oral spirochetes.8
Clinical Presentation:
- Diagnostic triad of pain, ulcerated or “punched out” interdental papillae, and gingival bleeding.9
- Other features include acute onset of fetid breath, blunting of interdental papilla, teeth mobility, malaise, and submandibular and submental lymphadenopathy.
- Ulcerative necrotic slough of the gingiva
- Removing film causes bleeding and exposure of ulcerated and erythematous tissue.

Evaluation:10
- Assess ABCs and VS abnormalities.
- Rarely, can present with fever, tachycardia, and trismus requiring resuscitation and possible airway management.10
- Close oropharyngeal and neck examination to assess for halitosis, blunting of interdental papilla, teeth mobility, malaise, and submandibular and submental lymphadenopathy.10
- Laboratory Evaluation: May consider basic labs such as CBC with differential and CMP, but as with imaging, very limited data or guidelines suggesting routine labs for uncomplicated patients presenting with ANUG.
- Imaging: Consider CT maxillofacial with contrast if concerned for abscess or periosteal spread.11
- Differential:
- Acute lymphoblastic leukemia: presents with features typical of an immunocompromised state: fever, bleeding/bruising, lymphadenopathy, more common in younger populations.
- Odontogenic infections: Acute alveolar osteitis, Ludwig’s angina, periapical abscess, periodontal abscess.8
- Scurvy
- Gingival hyperplasia: causes include Phenytoin, Cyclosporine, Nifedipine, Amlodipine, Leukemia
Treatment:
- Trismus, excessive sloughing of gingiva, or oropharyngeal edema may prompt early airway management with adjuncts and ENT/anesthesia for assistance in an anatomically difficult airway.
- Antibiotics:12
- Antimicrobial rinses, 0.12% chlorhexidine gluconate BID for 2 weeks.
- Amoxicillin/Clavulanate 875 mg PO two times daily AND Metronidazole 500mg PO three times daily x 7 days
- Clindamycin 300mg PO three times daily
- Doxycycline 100mg PO BID x 10 days
- If allergic to penicillin, use Ciprofloxacin 500mg twice daily AND metronidazole 500mg PO three times daily
- Other considerations: intense gingivostomatitis may require IV antibiotics due to PO intolerance.
- Appropriate regimens include Ampicillin-sulbactam 1.5 to 3g IV q6hrs or Clindamycin 600mg IV q8hrs.
- Macrolides have good gingival penetration.11
- Considerations for immunocompromised patients:
- Nystatin oral rinse four times daily x 14 days or Fluconazole 200mg PO daily x 14 days
- Invasion into surrounding bone as necrotizing stomatitis:
- Complication of invasion of infection in to surrounding bone of maxilla or mandible may require urgent OMFS and/or ENT consultation for management.11
- Debridement:
- Recommended for all ANUG patients along with systemic antibiotic treatment and antimicrobial rinses.8
- Will require significant pain control for debridement
- Immunocompromised state: Consider testing for HIV, syphilis, HSV.4
- Appropriate regimens include Ampicillin-sulbactam 1.5 to 3g IV q6hrs or Clindamycin 600mg IV q8hrs.
Disposition:
- Milder cases can be discharged with antibiotics, close outpatient follow up with a dentist, antibiotics, and chlorhexidine.3
- For severe infections, consult ENT or OMFS for possible dental debridement and admission.1
Pearls:
- ANUG occurs primarily in immunocompromised patients.
- Primarily a clinical diagnosis, hallmark sign is ulcerated interdental papillae with an ulcerative necrotic sloughing of the gingiva.
- Treatment focuses on infection control with best antibiotic regimen along with reducing contributing risk factors and consulting OMFS or dental professional for debridement if necessary.


A 20-year-old man with human immunodeficiency virus presents with severe oral pain and gingival bleeding. Oral examination is shown above. There is no facial edema, erythema, or fever. What is the next best step in management?
A) Admission for intravenous clindamycin
B) Discharge home with cephalexin
C) Discharge home with chlorhexidine, penicillin, and dental referral
D) Discharge home with nystatin
Answer: C
Acute necrotizing ulcerative gingivitis (ANUG) is a periodontal infection where bacteria invade normal oral tissue. It is characterized by painful, edematous interdental papillae. While the interdental papillae are normally pointed, in ANUG there is blunting and ulceration. There may also be a pseudomembrane covering the gingiva which, if removed, reveals bleeding, ulcerated tissue. It is most frequently noted around the anterior incisors and posterior molars. Patients may also have fetid breath, lymphadenopathy, malaise, and fever. Risk factors for developing ANUG include a compromised immune system (e.g. HIV), poor oral care, stress, smoking, and malnutrition. Treatment consists of analgesics, systemic antibiotics (e.g. clindamycin or penicillin), and chlorhexidine rinses. Dental referral is also essential as these patients require thorough debridement and close follow up.
Admission for intravenous clindamycin (A) is not indicated as patients typically respond well to outpatient management. Discharge home with cephalexin (B) does not provide complete treatment as the patient should also have close dental follow up. Discharge home with nystatin (D) is indicated in cases of oral thrush.
Further Reading:
Recommended FOAM:
References:
- Malek R, Gharibi A, Khlil N, Kissa J. Necrotizing ulcerative gingivitis. Contemp Clin Dent. 2017;8(3):496. doi:10.4103/ccd.ccd_1181_16
- Melnick S, Roseman J, Engel D, Cogen R. Epidemiology of Acute Necrotizing Ulcerative Gingivitis. Epidemiol Rev. 1988;10(1):191-211. doi:10.1093/oxfordjournals.epirev.a036022
- Johnson B, Engel D. Acute necrotizing ulcerative gingivitis. A review of diagnosis, etiology and treatment. J Periodontol. 1986;57(3):141-150.
- Kato H, Imamura A. Unexpected acute necrotizing ulcerative gingivitis in a well-controlled hiv-infected case. Intern Med. 2017;56(16):2223-2227. doi:10.2169/internalmedicine.8409-16
- Cogen RB, Stevens AW, Cohen-Cole S, Kirk K, Freeman A. Leukocyte Function in the Etiology of Acute Necrotizing Ulcerative Gingivitis. J Periodontol. 1983;54(7):402-407. doi:10.1902/jop.1983.54.7.402
- Van Dyke TE, Hoop GA. Neutrophil function and oral disease. Crit Rev Oral Biol Med. 1990;1(2):117-133. doi:10.1177/10454411900010020201
- Arendorf TM, Bredekamp B, Cloete CA, Joshipura K. Seasonal variation of acute necrotising ulcerative gingivitis in South Africans. Oral Dis. 2001;7(3):150-154. http://www.ncbi.nlm.nih.gov/pubmed/11495190. Accessed April 9, 2020.
- Pihlstrom BL, Ammons WF. Treatment of gingivitis and periodontitis. Research, Science and Therapy Committee of the American Academy of Periodontology. J Periodontol. 1997;68(12):1246-1253. http://www.ncbi.nlm.nih.gov/pubmed/9444602. Accessed April 9, 2020.
- Tintinalli JE, Stapczynski JS, Ma OJ, Yealy DM, Meckler GD, Cline D. Tintinalli’s Emergency Medicine : A Comprehensive Study Guide.
- Atout RN, Todescan S. Managing patients with necrotizing ulcerative gingivitis. J Can Dent Assoc. 2013;79:46.
- Maccarrone F, Alicandri-Ciufelli M. Plaut-Vincent’s Ulcerative Gingivitis and Tonsillitis. Otolaryngol – Head Neck Surg (United States). 2019;161(6):1056-1057. doi:10.1177/0194599819868171
- Walker C, Karpinia K. Rationale for Use of Antibiotics in Periodontics. J Periodontol. 2002;73(10):1188-1196. doi:10.1902/jop.2002.73.10.1188





1 thought on “EM@3AM: Acute Necrotizing Ulcerative Gingivitis”
Pingback: ePulse: Highlights of the week 18 – 23 April 2020 – V E N T R I C L E