Spontaneous Coronary Artery Dissection
By Krystle Shafer MD, William Fields MD, and Mark Gonzales DO, MPH
(Chief Residents, Dept of Emergency Medicine, WellSpan York Hospital in York, PA)
Edited by Alex Koyfman MD (@EMHighAK) and Stephen Alerhand MD (@SAlerhand)
Case 1:
A 26 year-old M presents to the ED with a chief complaint of chest pain that started acutely at 3 am. His pain is constant and located in the center of his chest. Nothing makes his pain better or worse, and it is not positional. He woke up vomiting this morning while also feeling short of breath. He has no PMH, takes no medications, and has no significant family or social history. Vital signs: HR 111, BP 166/106, RR 18, oral temp 98.0F, oxygen saturation is 100%. On exam he is pale and diaphoretic, leaning forward and clutching his chest. Lungs are clear to auscultation bilaterally, heart has a regular rate and rhythm without murmurs/rubs/gallops. EKG reveals diffuse ST elevation. Bedside echocardiogram reveals normal ejection fraction, but there are concerns for wall motion abnormalities at the apex. Pertinent labs revealed a WBC count of 19.5, troponin 3.05, lactic acid 3.9, BNP 66. Eventual cardiac catheterization revealed spontaneous LAD dissection, which was subsequently stented.
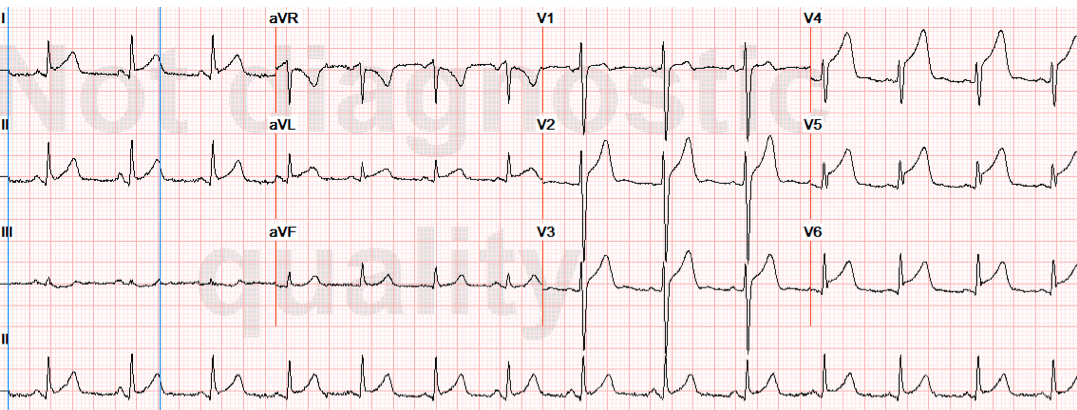
Case 1 EKG: diffuse ST elevation
Case 2:
A 38 year-old F presents to the ED with a chief complaint of chest pain that started approximately 12 hours prior to arrival. The pain is intermittent but progressively worsening. It is a constant, mid-sternal, 10/10 sharp pain present for the past 30 minutes. She has no exacerbating or relieving factors, and her pain is non-radiating. She had nausea and vomiting throughout the day as well as dyspnea and diaphoresis. PMH includes atrial fibrillation and hypertrophic cardiomyopathy. Vital signs: HR 87, BP 156/114, RR 24, oral temp 97.3F, oxygen saturation is 100%. On exam she is pale, diaphoretic, and writhing in distress. Lungs are clear to auscultation bilaterally, heart has an irregularly irregular rhythm and is without murmurs. There is no peripheral edema. EKG reveals ST elevation in the anterolateral leads. Pertinent labs revealed WBC count of 22.1, troponin 0.13, and BNP 924. She immediately went to the catheterization lab, which revealed a spontaneous LAD dissection. This was unable to be stented and required an emergent CABG.
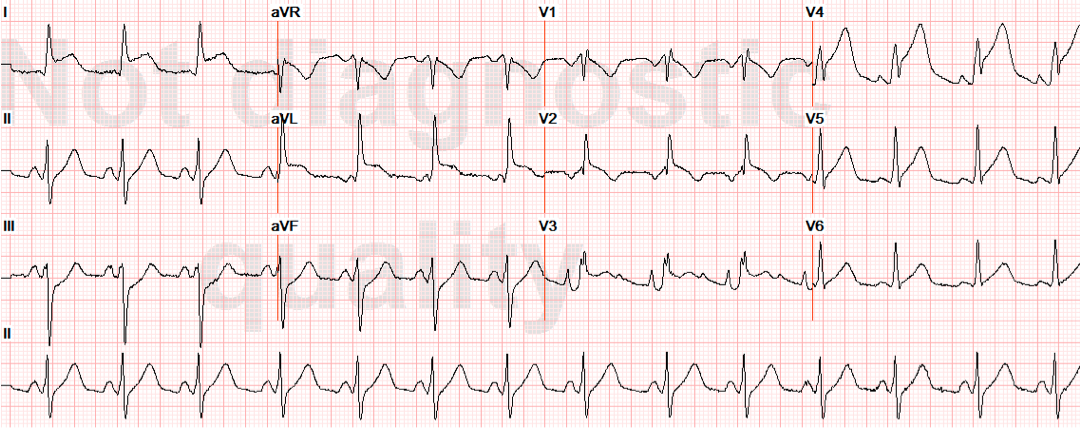
Case 2 EKG: anterolateral ST elevation
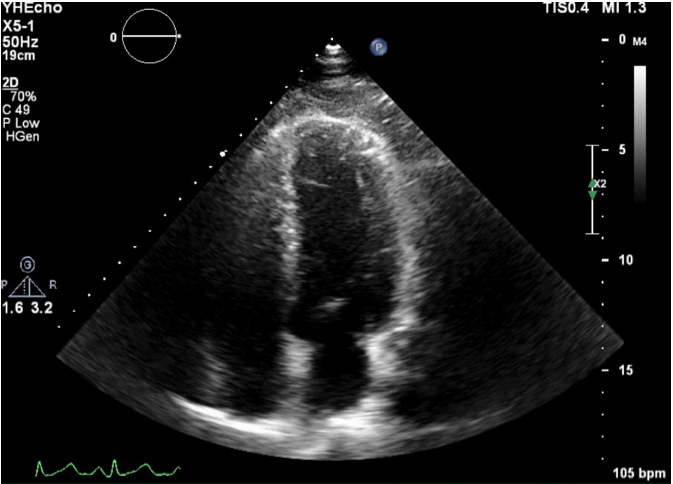
Case 2 Echo: akinetic apical wall
Background
Chest pain is a common complaint among patients presenting to the Emergency Department (ED). In patients <50 years old, chest pain is more likely to be benign. However, spontaneous coronary artery dissection (SCAD) is an uncommon diagnosis that uniquely targets the younger population and is potentially fatal if misdiagnosed. In 1996, only 100 cases in the world had been identified1. Of these reported cases, 75% were diagnosed at autopsy and the rest were diagnosed with coronary angiography2. The majority of these cases were found in women —approximately 75% — and of these cases, 32% of the patients were pregnant, post-partum, or taking oral contraceptives, suggesting that hormonal factors potentially have an effect1.
A more recent retrospective study revealed 87 patients diagnosed at the Mayo Clinic from 1979-20113. 82% of these patients were female and the mean age was 42.6, with 18% of the female patients being postpartum. STEMI was apparent in 49% of patients, NSTEMI in 44%, and the rest had unstable angina. Fibromuscular dysplasia was found to be a potential causative factor as well. The LAD was involved in 71% of cases and multi-vessel disease was apparent in 23%. The pathophysiologic etiology of this disease is unclear, but some autopsies have demonstrated an eosinophilic penetration of the tunica adventitia, and it is postulated that this subsequently causes damage to the collagen, elastin, and smooth muscle wall2. SCAD may also be a source for sudden cardiac death in athletes or those suffering blunt, shear-force trauma and may be under-reported in this regard4. A high index of suspicion is essential in these cases. This article focuses on the key identifying factors about this disease to help prevent the ED physician from missing this diagnosis.
Physical Exam
SCAD patients will raise your “sick” feelers that all ED physicians develop. They will look like the textbook heart attack patient except they are generally a young age for MI. Patients will be diaphoretic, pale, and typically experience significant chest pain. It is not typical for patients to experience new dysrhythmias in the setting of coronary dissection. Severe cardiac ischemia due to the dissecting artery can potentially result in acute CHF.
Imaging/Labs
- EKG will traditionally reveal ST elevation in the leads of the dissecting artery.
- Troponin will be elevated after 4-6 hours from symptom onset due to ischemia.
- Lactic acid can be elevated as well but depends on the degree of heart dysfunction and organ ischemia.
- Bedside US will commonly reveal wall motion abnormalities related to the dissecting vessel.
- Diagnosis is made definitively with cardiac catheterization, intravascular ultrasound, optical coherence tomography, or at autopsy.
Management
Treatment options for SCAD patients include medical management, stenting, or bypass surgery. There are no guidelines or standard treatment at this time, and the prognosis of these patients who survive is unknown. However, the case reports overall seem to demonstrate that the one year post-event survival rate is quite high. One study found a 17% recurrence rate (all of which were female) as well as a long-term survival rate that was comparative to patients with acute coronary syndrome (ACS)3.
Summary
Spontaneous coronary artery dissection is a rare diagnosis with high potential for mortality or significant morbidity. SCAD should be considered in the differential diagnosis of acute chest pain patients, with heightened clinical suspicion in young female patients under age 50 who present like ACS. Peripartum status, fibromuscular dysplasia, and shear stress from blunt trauma are also potential causative factors that should increase clinical suspicion. SCAD will mimic ACS with ST elevations on EKG, troponin increase, and wall motion abnormalities on bedside echo. These patients are diagnosed in the catheterization lab and typically managed with either a stent or bypass surgery.
References / Further Reading
- Zampieri et al. Follow up after spontaneous coronary artery dissection: a report of five case series; 1996: 75, 206-209
- Spontaneous Coronary Artery Dissection, Aneurysms, and Pseudoaneurysms: A Review. Echocardiography. 2004: 21(2), 175-182.
- Tweet, et al. Clinical Features, Management, and Prognosis of Spontaneous Coronary Artery Dissection. Circulation. 2012;126:667-670.
- Van Mieghan, et al. Traumatic Coronary Artery Dissection: Potential Cause of Sudden Death in Soccer. Circulation. 2013;127:280-282.
- Vanzetto, et al. Prevalence, therapeutic management and medium-term prognosis of spontaneous coronary artery dissection: results from a database of 11,605 patients. European Journal of Cardio-thoracic Surgery. 2008: 35 (3), 205-254.
- Vrints, Christian. Spontaneous coronary artery dissection. Heart. 2010;96:801-808.
- http://www.ncbi.nlm.nih.gov/pubmed/23158608
- http://www.ncbi.nlm.nih.gov/pubmed/22917653
- http://www.ncbi.nlm.nih.gov/pubmed/22560269
- http://www.ncbi.nlm.nih.gov/pubmed/20605390
- http://www.ncbi.nlm.nih.gov/pubmed/22224163




