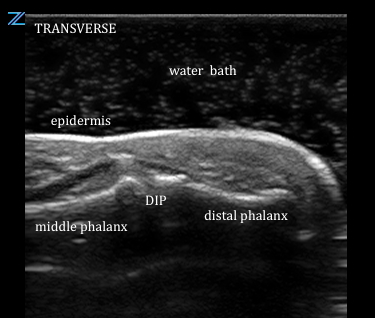
US Probe: Ultrasound Water Bath for Distal Extremity Evaluation
Point-of-care ultrasound is becoming an increasingly more common part of the emergency department evaluation. In this post, we explore the benefits of using water in place of ultrasound gel to evaluate distal extremity injuries.
US Probe: Ultrasound Water Bath for Distal Extremity Evaluation Read More »