Authors: Kendra Jackson, MD (Pediatric Emergency Medicine Fellow, Atrium Health’s Carolinas Medical Center); Christine Murphy, MD (Emergency Medicine Attending, Medical Toxicologist, Atrium Health’s Carolinas Medical Center) // Reviewed by: Anthony Spadaro, MD (@TSpadaro91, Medical Toxicology Fellow, Rutgers New Jersey Medical School, Newark, NJ); James Dazhe Cao, MD (@JamesCaoMD, Associate Professor of EM, Medical Toxicology, UT Southwestern Medical Center, Dallas, TX); Alex Koyfman, MD (@EMHighAK); Brit Long, MD (@long_brit)

Case:
A 22-year-old male with a history of depression presents with altered mental status. Per paramedics, the patient was lying in an empty bathtub with a suicide note. On arrival, the patient was confused and responding to internal stimuli. Vitals include a temperature of 98.5°F, BP 129/94, HR 116, RR 28, and oxygen saturation of 96% on room air. On exam, the patient was agitated and trying to eat his EKG leads. His exam is also notable for 4+ patellar reflexes, ocular clonus, and tremor. The patient attempts to walk but stumbles due to spontaneous clonus at the ankles bilaterally. The only home medication reported is duloxetine.
Questions:
- What is the metabolic pathway of serotonin?
- What is serotonin toxicity, and how does it present clinically?
- What are the pitfalls of the Hunter criteria?
- What are some common medications or recreational drugs associated with serotonin toxicity?
Background:
- Serotonin (5-HT) is a neurotransmitter made in presynaptic neurons and found in the central nervous system (CNS), gastrointestinal tract, and platelets.1
- Serotonin biosynthesis (Fig. 1):1,2
- Tryptophan is an amino acid that is hydrolyzed and decarboxylated by two different enzymes to create serotonin.
- Serotonin is loaded into vesicles in the presynaptic nerve and transported to the synapse.
- Serotonin travels across the synaptic gap and binds receptors on post-synaptic neurons to activate cell signaling pathways.
- Serotonin breakdown (Fig. 1):1
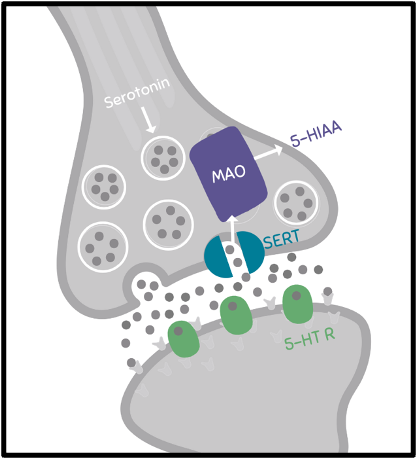
Figure 1. Serotonin release and reuptake from the synapse. 5-HT R – serotonin receptor; SERT – serotonin transporter protein; 5-HIAA – 5-hydroxyindoleacetic acid; MAO – monoamine oxidase. Image created by K Jackson, adapted from Chiew, et al.3
- “Serotonin toxicity” or “serotonin syndrome” are terms often used interchangeably to describe moderate to severe serotonin toxicity with “serotonin toxicity” being the preferred term.3
- Serotonin toxicity is a spectrum of disease that transpires when there is too much intra-synaptic CNS serotonin. This usually occurs through a combination of the following:3
- Increased production of pre-synaptic serotonin
- Increased release from pre-synaptic serotonin stores
- Decreased 5-HT clearance due to either serotonin reuptake inhibition or inhibition of monoamine oxidase
- When intra-synaptic 5-HT levels increase, there is increased agonist activity at the 5-HT1A or 5-HT2A receptors, the primary receptors associated with the clinical effects that define serotonin toxicity.
- Serotonin toxicity from a single serotonin agonist alone is unlikely.5
Clinical Presentation:
- Patients taking therapeutic doses of medications that increase intrasynaptic serotonin concentrations can experience side effects such as nausea, diarrhea, and tremor.
- Symptoms of serotonin toxicity range from mild to severe clinical effects (Fig. 2).3
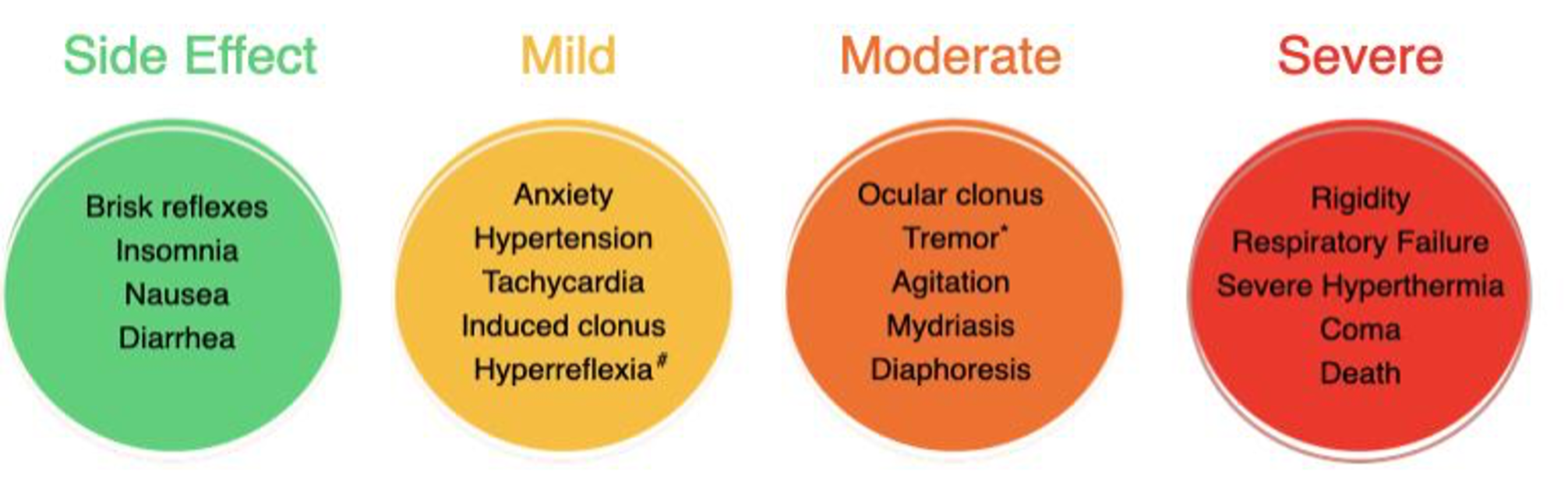
Figure 2. Symptoms noted in the spectrum of serotonin toxicity. #Hyperreflexia is usually worse in the lower extremities than upper extremities. *Tremor is a known side effect of selective serotonin reuptake inhibitors (SSRIs) but also appears as a criteria for diagnosing serotonin toxicity. Image created by K Jackson, adapted from Foong, et al.2 and Chiew, et al.3
Diagnosis:
- The diagnosis of serotonin toxicity is clinical and may be aided by clinical decision rules.
- Two primary decision rules are available to assist providers, the Sternbach’s criteria and the Hunter Serotonin criteria. Sternbach’s criteria were developed based primarily on therapeutic drug-drug interactions.3 The Hunter criteria supplanted Sternbach’s criteria for diagnosing serotonin toxicity in the early 2000’s.4

Adapted from Dunkley, et al. 4
- The Hunter criteria use decision rules with clinical features more specific to serotonin toxicity and are considered more specific and sensitive than Sternbach’s criteria.4

Adapted from Dunkley, et al. 4
- Originally developed by a retrospective review of single-agent SSRI overdoses, these criteria were validated in a second retrospective review of patients who overdosed on any serotonergic drug.3,4 However, they have not been validated for symptoms resulting from therapeutic use.
- Some toxicologists question the clinical validity of the Hunter criteria due to the non-specific symptoms and a lack of an appropriate clinical scenario where either a new serotonergic medication or drug is introduced, the dose of an existing medication is increased, or there is an overdose of medication.3
- Example: A patient who has been clinically stable for years on 20 mg of fluoxetine presents with fever, hypertonia, and clonus. The patient’s cerebral spinal fluid (CSF) polymerase chain reaction (PCR) is positive for herpes simplex virus (HSV).
- Though some might consider the clinical effects as related to serotonin toxicity, it is more likely attributed to HSV encephalitis.
- This emphasizes that in addition to the Hunter criteria, providers should think critically about the overall condition of the patient and the neurochemistry of medications possibly involved.3
- Example: A patient who has been clinically stable for years on 20 mg of fluoxetine presents with fever, hypertonia, and clonus. The patient’s cerebral spinal fluid (CSF) polymerase chain reaction (PCR) is positive for herpes simplex virus (HSV).

- To be diagnosed with serotonin toxicity, a patient needs to have a combination of the right symptoms AND be exposed to medications whose mechanism could lead to an increase in serotonin in the CNS.
- The right symptoms
- Does the patient have symptoms consistent with serotonin toxicity as defined by the Hunter Criteria?
- The right mechanism
- Has the patient been exposed to a drug or drugs with a mechanism that increases intrasynaptic serotonin by either increasing release of 5-HT into the synapse or decreasing metabolism of 5-HT?
- Does it increase serotonin in the CNS specifically?
- Some medications are erroneously associated with serotonin toxicity merely because they have “serotonergic” activity, meaning they work on a serotonin receptor.
- It is important to keep in mind that it is increased serotonin in the synapse that drives serotonin toxicity.
- A combination of the specific drug mechanism and context of exposure can lead to a varying risk of developing serotonin toxicity.
- While activity at 5-HT1A and 5-HT2A receptors is associated with features of serotonin toxicity, serotonin agonism alone, without increased intrasynaptic serotonin, would not be expected to cause serotonin toxicity.
- Of note, the 5-HT2A receptors play a significant role in hyperthermia and neuromuscular features of serotonin toxicity3
- Additionally, not all serotonin receptor agonists are associated with true serotonin toxicity.2
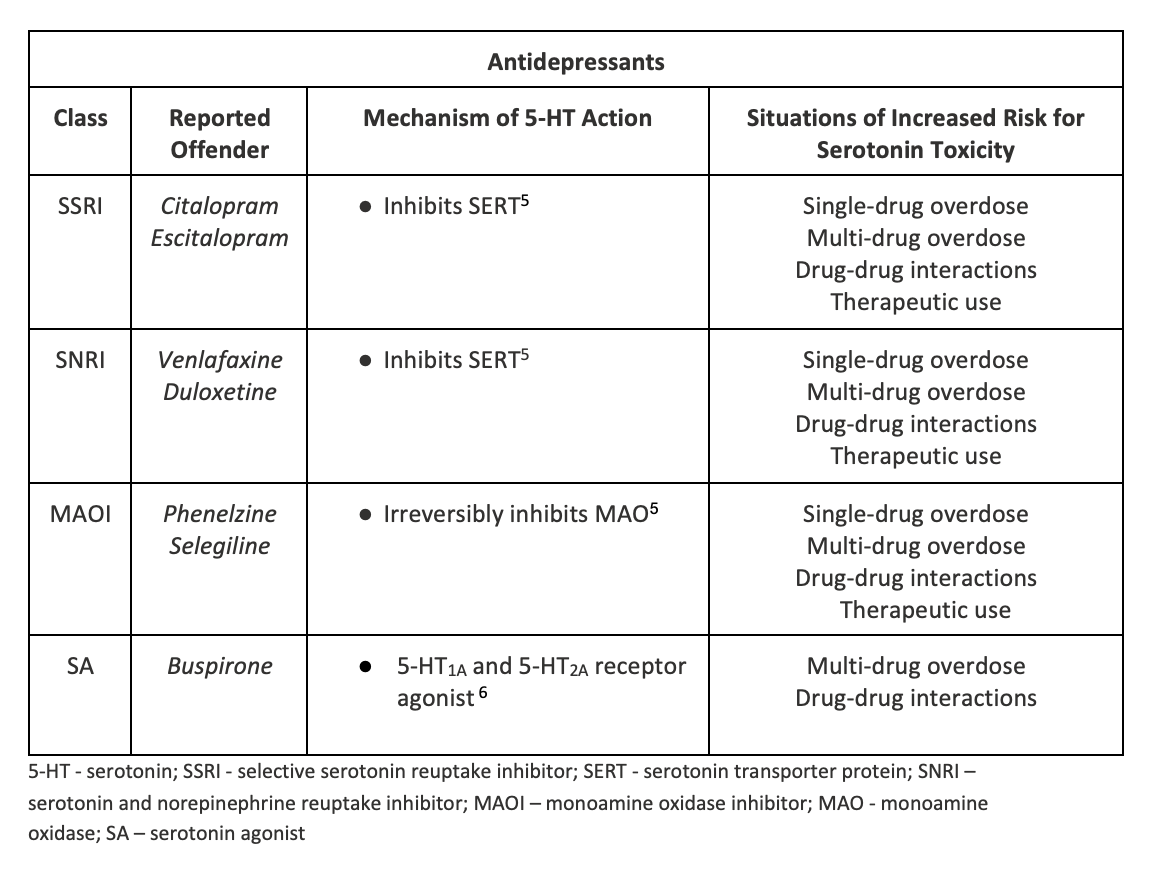
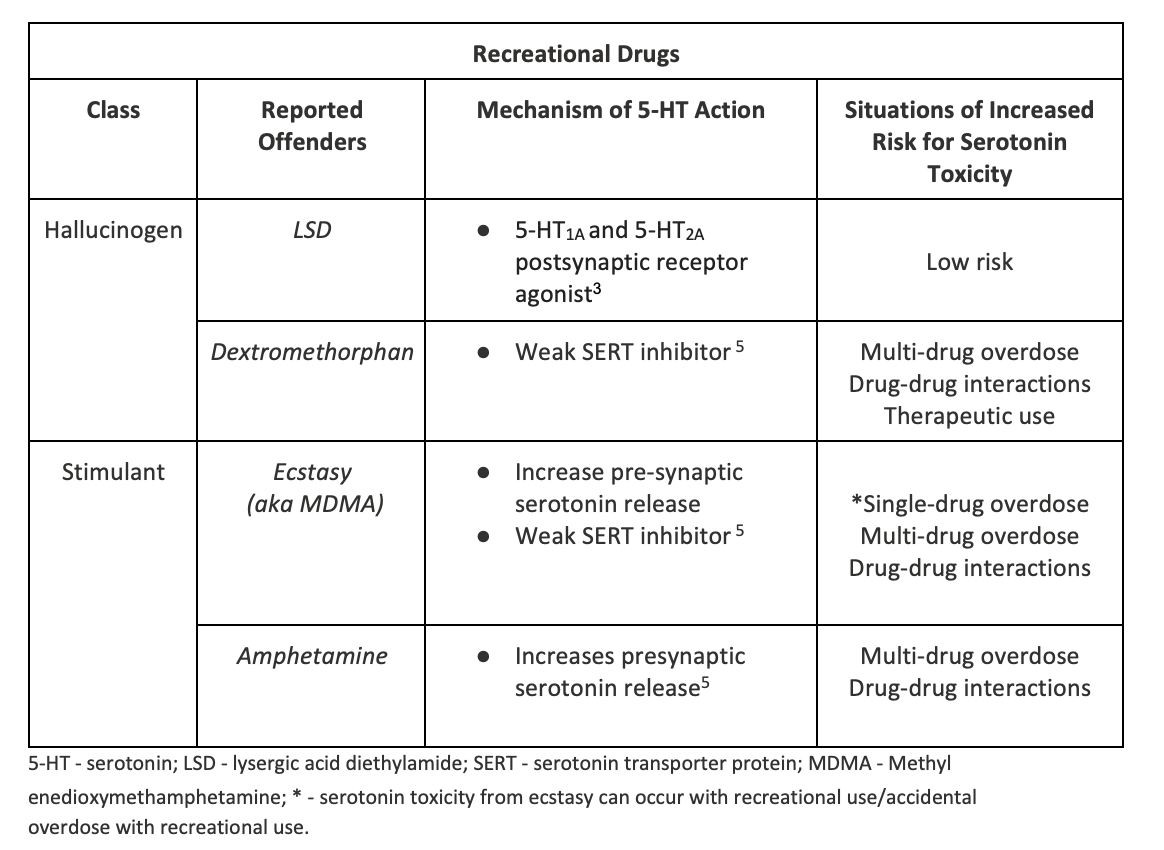
- Situational risk for developing serotonin toxicity:
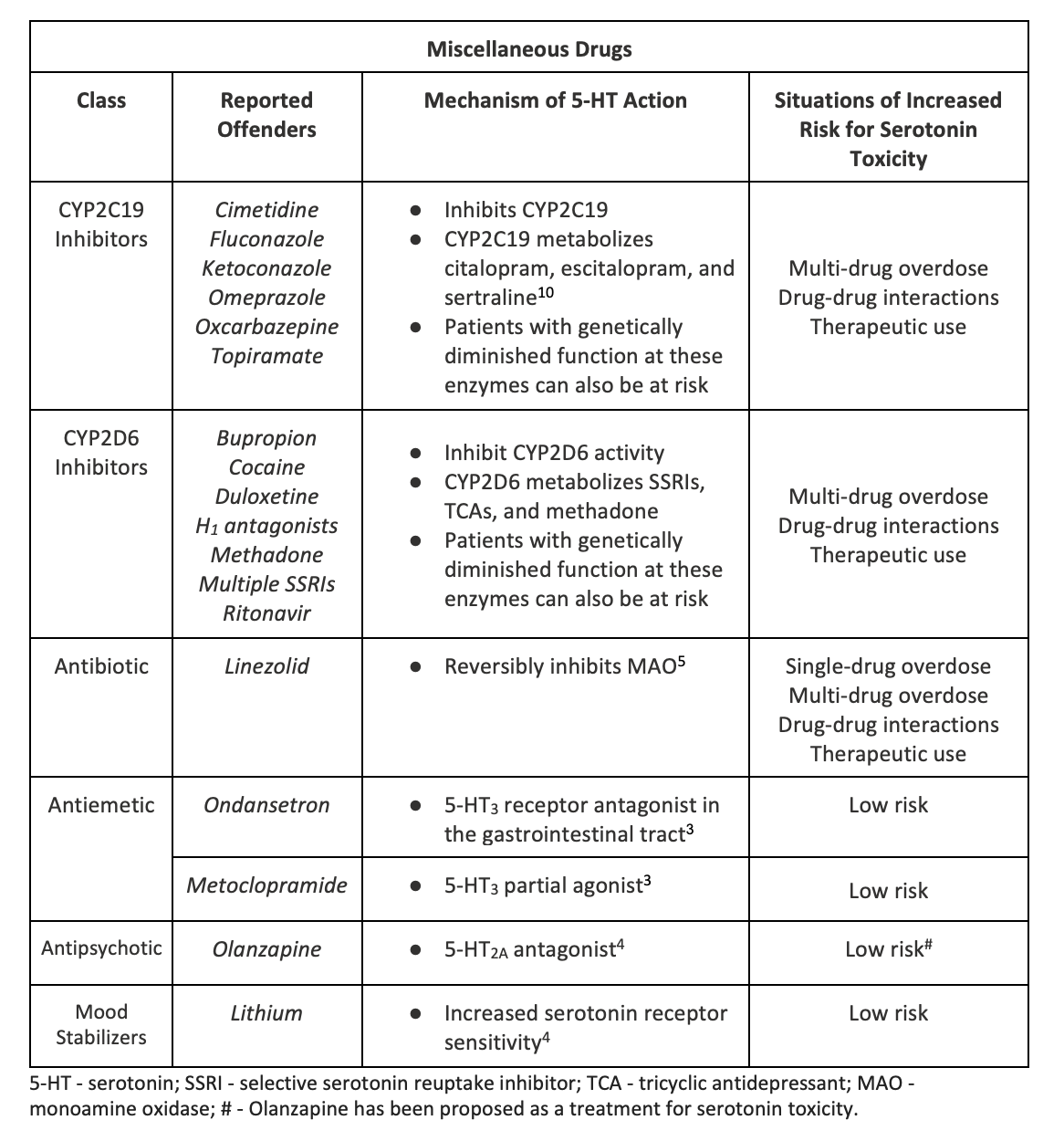
- Several scenarios where drugs with the “right mechanism” taken alone or in combination with other serotonergic drugs can increase the risk for developing serotonin toxicity (see tables below; of note, these tables are not all-inclusive)
- Single-drug overdose: A drug that increases intra-synaptic serotonin when taken alone in an overdose
- Multi-drug overdose: A drug that increases intra-synaptic serotonin taken in overdose with other serotonergic drugs that also increase intra-synaptic serotonin
- Drug-drug interactions: A drug that increases intra-synaptic serotonin taken therapeutically in combination with other serotonergic drugs that also increase intra-synaptic serotonin (directly or indirectly)
- Therapeutic use: A drug taken therapeutically that increases intra-synaptic serotonin concentrations in the CNS in the setting of a recent dose increase
- Low risk: there are some low-risk drugs that have 5-HT receptor effects that do not increase pre- or intra-synaptic 5-HT concentrations. These are drugs that would not be expected to cause or contribute to serotonin toxicity when taken in combination with other drugs that increase intra-synaptic serotonin levels.
- Ondansetron, for example, acts as a 5-HT3 receptor antagonist in the gastrointestinal tract, so would not meet criteria for the right mechanism.3
- Similarly, olanzapine is another drug many providers believe can cause serotonin toxicity. Olanzapine is a 5-HT2A antagonist. In fact, olanzapine has been successfully used as a treatment in mice suffering from serotonin toxicity and has been proposed as a treatment for human serotonin toxicity.2,4-6

Management:
- Stop the offending drugs.4
- Avoid the use of new serotonergic agents, especially high or moderate-risk agents.
- Keep the patient calm, preferentially using benzodiazepines for agitation.
- Alternatively, can consider a combination of benzodiazepines and dexmedetomidine, if appropriate, to assist with sedation.
- Symptomatic care of hyperthermia:11
- Aggressively cool patients, increase sedation, and consider intubation and paralysis in more severe cases
- Cyproheptadine has been used as an adjunct treatment for mild to moderate serotonin toxicity.11 This only comes as an oral medication and there is some debate as to its effectiveness.
- Consider consulting a regional poison control center or medical toxicologist to discuss the diagnosis and management of serotonin syndrome.
- For a more detailed discussion on treatment, please refer to EM@3AM: Serotonin Syndrome
Case Follow-up:
The patient is admitted to the intensive care unit. On hospital day 2, he required several as needed doses of intravenous midazolam. He was intubated for airway protection and sedated with propofol. The patient’s family arrived from out of town and searched his home. In the bathtub, there were two empty bottles of dextromethorphan containing cough syrup and an empty bottle of duloxetine. On hospital day 3, the patient’s hyperreflexia and tachycardia resolved, his sedation was weaned, and he was extubated.
Clinical Pearls:
- Serotonin toxicity is a spectrum of disease.
- Once other medical diagnoses have been excluded, a patient with the right symptoms and exposure to a drug with the right mechanism can be diagnosed with serotonin toxicity.
- Decision rules like the Hunter Serotonin Toxicity Criteria can be applied to aid in diagnosis.
- Stop the suspected offending agent(s) and avoid other drugs that increase intra-synaptic serotonin.
- Mainstays are symptomatic and supportive care for agitation and hyperthermia.5
References:
- Boyer EW, Shannon M. The serotonin syndrome. N Engl J Med. 2005 Mar 17;352(11):1112-20. doi: 10.1056/NEJMra041867. Erratum in: N Engl J Med. 2007 Jun 7;356(23):2437. Erratum in: N Engl J Med. 2009 Oct 22;361(17):1714. PMID: 15784664.
- Chiew AL, Buckley NA. The serotonin toxidrome: shortfalls of current diagnostic criteria for related syndromes. Clin Toxicol (Phila). 2022 Feb;60(2):143-158. doi: 10.1080/15563650.2021.1993242. Epub 2021 Nov 22. PMID: 34806513.
- Curry SC, O’Connor AD, Graeme KA, Min Kang AA. Neurotransmitters and Neuromodulators. In: Nelson LS, Howland M, Lewin NA, Smith SW, Goldfrank LR, Hoffman RS. eds. Goldfrank’s Toxicologic Emergencies, 11e. McGraw Hill; 2019. Accessed August 20, 2022. https://accessemergencymedicine.mhmedical.com/content.aspx?bookid=2569§ionid=210258698
- Dunkley EJ, Isbister GK, Sibbritt D, Dawson AH, Whyte IM. The Hunter Serotonin Toxicity Criteria: simple and accurate diagnostic decision rules for serotonin toxicity. QJM. 2003 Sep;96(9):635-42. doi: 10.1093/qjmed/hcg109. PMID: 12925718.
- Foong AL, Grindrod KA, Patel T, Kellar J. Demystifying serotonin syndrome (or serotonin toxicity). Can Fam Physician. 2018 Oct;64(10):720-727. PMID: 30315014; PMCID: PMC6184959.
- Francescangeli J, Karamchandani K, Powell M, Bonavia A. The Serotonin Syndrome: From Molecular Mechanisms to Clinical Practice. Int J Mol Sci. 2019 May 9;20(9):2288. doi: 10.3390/ijms20092288. PMID: 31075831; PMCID: PMC6539562.
- Baldo BA, Rose MA. The anaesthetist, opioid analgesic drugs, and serotonin toxicity: a mechanistic and clinical review. Br J Anaesth. 2020 Jan;124(1):44-62. doi: 10.1016/j.bja.2019.08.010. Epub 2019 Oct 22. PMID: 31653394.
- Rickli A, Liakoni E, Hoener MC, Liechti ME. Opioid-induced inhibition of the human 5-HT and noradrenaline transporters in vitro: link to clinical reports of serotonin syndrome. Br J Pharmacol. 2018 Feb;175(3):532-543. doi: 10.1111/bph.14105. Epub 2018 Jan 6. PMID: 29210063; PMCID: PMC5773950.
- Tao R, Auerbach SB. GABAergic and glutamatergic afferents in the dorsal raphe nucleus mediate morphine-induced increases in serotonin efflux in the rat central nervous system. J Pharmacol Exp Ther. 2002 Nov;303(2):704-10. doi: 10.1124/jpet.102.038133. PMID: 12388654.
- Ricardo-Silgado ML, Singh S, Cifuentes L, Decker PA, Gonzalez-Izundegui D, Moyer AM, Hurtado MD, Camilleri M, Bielinski SJ, Acosta A. Association between CYP metabolizer phenotypes and selective serotonin reuptake inhibitors induced weight gain: a retrospective cohort study. BMC Med. 2022 Jul 26;20(1):261. doi: 10.1186/s12916-022-02433-x. PMID: 35879764; PMCID: PMC9317126.
- Stork CM. Serotonin Reuptake Inhibitors and Atypical Antidepressants. In: Hoffman RS, Howland M, Lewin NA, Nelson LS, Goldfrank LR. eds. Goldfrank’s Toxicologic Emergencies, 10e. McGraw Hill; 2015. Accessed August 20, 2022. https://accessemergencymedicine.mhmedical.com/content.aspx?bookid=1163§ionid=65097819




