Author: Jenna Otter, MD (Emergency Medicine resident at Temple University Hospital) // Edited by: Cynthia Santos, MD (Senior Medical Toxicology Fellow, Emory University School of Medicine), Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UT Southwestern Medical Center / Parkland Memorial Hospital) and Brit Long, MD (@long_brit)
Case:
A 45 yo M with PMH of substance abuse and psychiatric disease is brought in by police for AMS. He is agitated and profusely sweating. You struggle to place the restraints on him, as he won’t let you bring his arms to the side of the bed. An attending calls for Ativan for sedation. He is able to be placed on a monitor and you notice HR 136, BP 210/105. He has mydriatic pupils with erratic nystagmus. The patient continues to struggle against soft restraints, but calms momentarily for an oral temperature, which is 103.2 F. You look in his chart for his medication history and attempt to contact a relative to obtain more history.
Pearl:
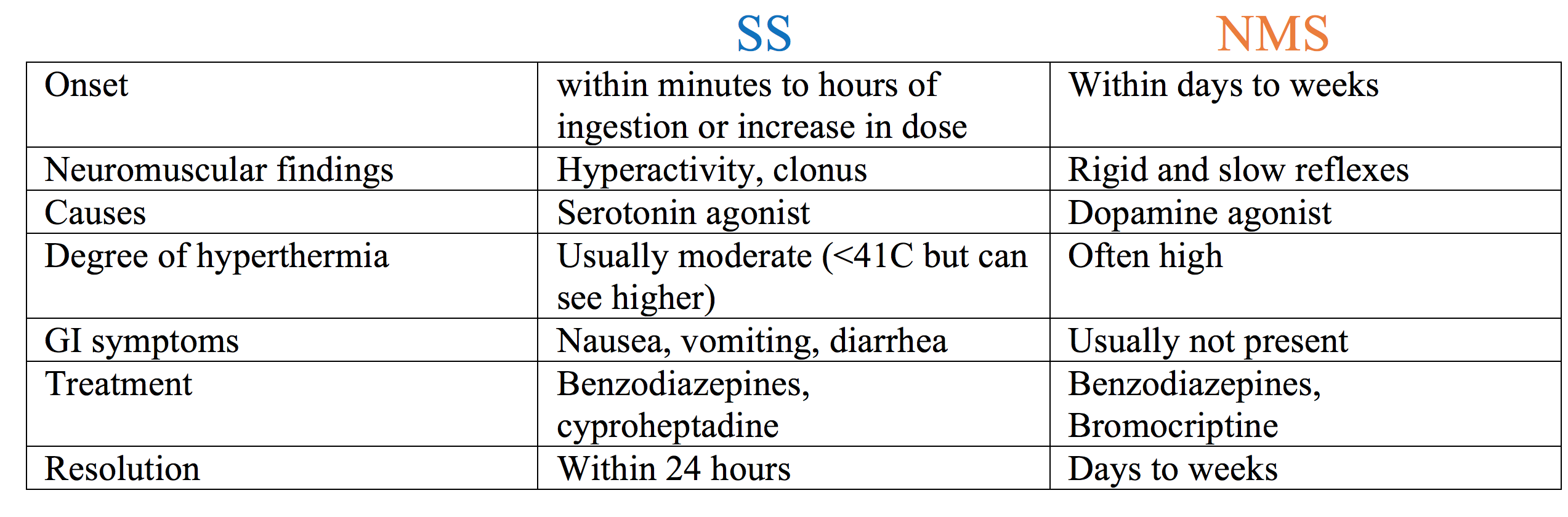
In a patient who presents with agitation and a concern for a toxicological hyperthermic syndrome, care should be given in determining medications used, as they could precipitate Serotonin Syndrome (SS) or contribute to development of the Neuroleptic Malignant Syndrome (NMS). When trying to differentiate between the two conditions think “FAST” with Serotonin Syndrome and “SLOW” with Neuroleptic Malignant Syndrome.
Serotonin Syndrome:
THINK: FAST
FAST onset
FAST movements (agitation, akathisia, HYPERreflexia)
FAST resolution
Neuroleptic Malignant Syndrome:
THINK: SLOW
SLOW onset
SLOW movements and HYPOreflexia
SLOW resolution

Serotonin Syndrome (SS)
- Some references1 break down serotonin syndrome into mild, moderate and severe based on degree of hyperthermia and physical exam features.
- Consider serotonin syndrome as a spectrum in order to recognize mild serotonin syndrome features in patients who may receive medications in the emergency department that could potentiate moderate to severe serotonin syndrome.

Diagnosis: the Hunter Serotonin Toxicity Criteria: only 84% sensitive and 97% specific.2
Known ingestion of a serotonergic drug plus one of the following:
- Spontaneous myoclonus
- Inducible clonus PLUS agitation or diaphoresis
- Ocular clonus PLUS agitation or diaphoresis
- Tremor PLUS hyperreflexia
- Hypertonia PLUS temperature above 38C PLUS ocular clonus or inducible clonus
Pearl: Increased muscle tone is more pronounced in the lower extremities in serotonin syndrome.
SS can be caused by drugs that increase serotonin release or decrease serotonin uptake.

Neuroleptic Malignant Syndrome (NMS)
- Idiosyncratic –
- Unlike serotonin syndrome which worsens in a dose-related fashion, NMS can happen at any time, is not necessarily precipitated by acute overdose, and can happen when a patient is therapeutic on the medication.
Causes:
- From decreased dopamine due to dopamine antagonism or cessation of dopamine agonism: neuroleptics, antiemetics, and the cessation of L-dopa in Parkinson’s patients
Diagnosis:
Simplified:
- Taking a dopamine antagonist (neuroleptic), or recent cessation of dopamine agonist medication
AND
- Fever with muscle rigidity
Case recap:
You find out that the patient lives in a halfway house and chronically receives weekly IM injections of haloperidol decanoate. The past week he hasn’t been participating in any of the group activities. He was last seen by a co-resident 6 days ago who reported that the patient seemed to have the flu and was lying in bed with a fever. He was picked up by security today after he was found lying outside of his home wearing no clothes. You diagnose him with NMS and actively cool the patient, start IV hydration, and continue to treat him with benzodiazepines. During his hospital stay there was some discussion about using bromocriptine or dantrolene but he ended up improving with just benzodiazepines alone.
References/Further Reading:
- Boyer E and Shannon M. The Serotonin Syndrome. N Engl J Med. 2005; 352:1112-1120. DOI: 10.1056/NEJMra041867.
- Dunkley EJ, Isbister GK, Sibbritt D, Dawson AH, Whyte IM. The Hunter Serotonin Toxicity Criteria: simple and accurate diagnostic decision rules for serotonin toxicity. QJM. 2003; 96(9):635-42.
- LoVecchio F and Mattison E. Chapter 178: Atypical and Serotonergic Antidepressants. In: Tintinalli J, ed. Tintinalli’s Emergency Medicine. 8th McGraw Hill; 2016: 1219-1224.
- Levine M and LoVecchio F. Chapter 180: Antipsychotics. In: Tintinalli J, ed. Tintinalli’s Emergency Medicine. 8th McGraw Hill; 2016: 1231-1232.
- Gurrera RJ, Caroff SN, Cohen A, et al. An International Consensus Study of Neuroleptic Malignant Syndrome Diagnostic Criteria Using the Delphi Method. The Journal of Clinical Psychiatry, Volume 72, Pages 1222-8, 2011.





2 thoughts on “TOXCARD: Differentiating Serotonin Syndrome and Neuroleptic Malignant Syndrome”
Pingback: emDOCs.net – Emergency Medicine EducationCommon Psychiatric Medications: Pearls & Pitfalls for the ED - emDOCs.net - Emergency Medicine Education
Pingback: Nursing FOAMed Review #2 (Aug 9th - Aug 20th) - Code Blue LLC