Authors: Alexander M Mozeika, PharmD (MS3, Rutgers New Jersey Medical School), Cynthia Santos, MD (Assistant Professor Emergency Medicine, Medical Toxicology, Rutgers New Jersey Medical School) // Reviewed by: Alex Koyfman, MD (@EMHighAK) and Brit Long, MD (@long_brit)

Case:
A 14-year-old female with a history of asthma on an unknown oral medication presents with vomiting and diarrhea. She was admitted and subsequently developed seizures in the setting of hyperglycemia and hypokalemia. Further work-up revealed a combined respiratory alkalosis and metabolic acidosis. She endorses that she has “been forgetful” and took double her dose for the last two days.
Questions:
- What are the pharmacokinetic factors of elimination?
- How are these factors altered in the setting of toxicology (i.e. toxicokinetics)?
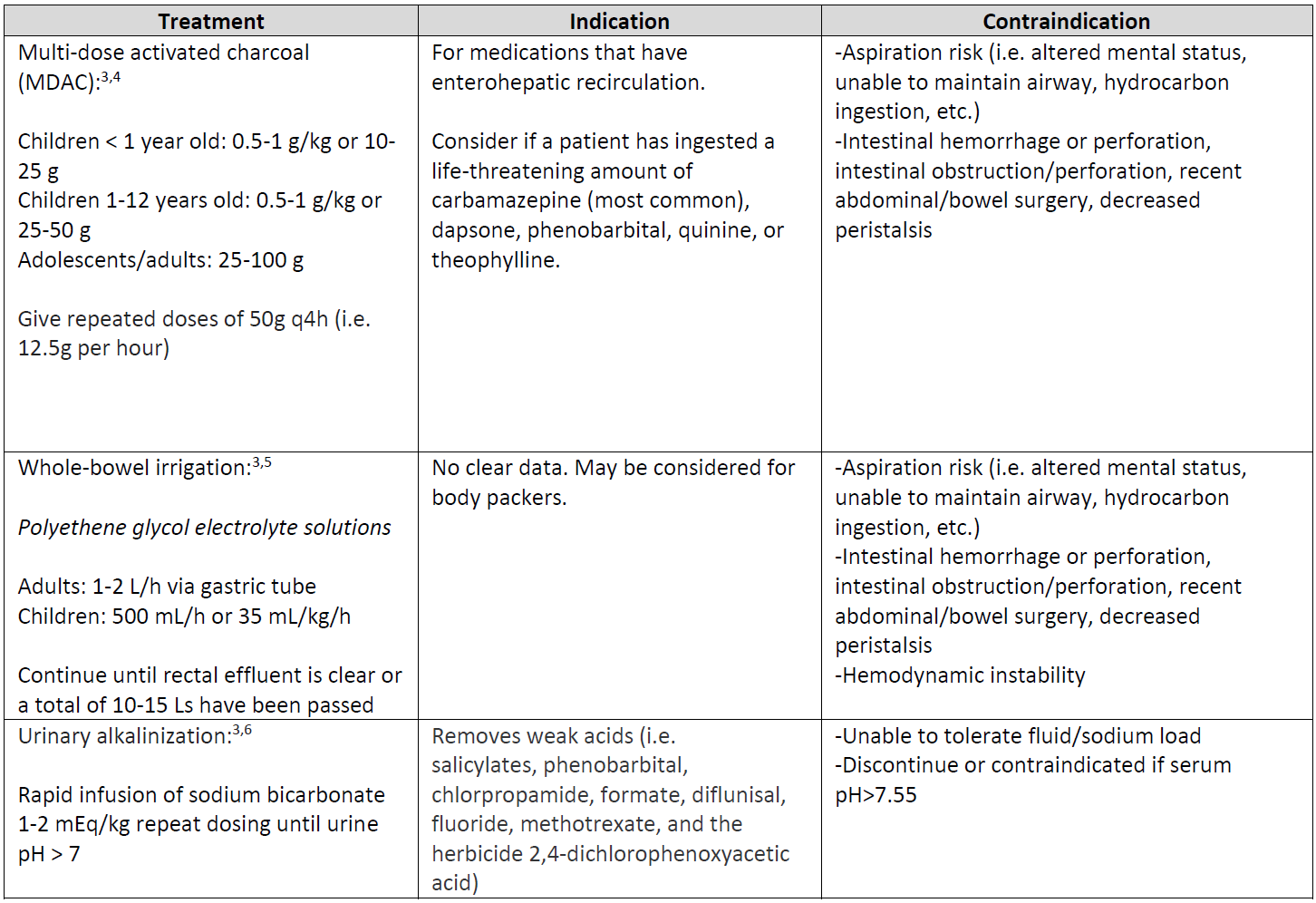
- What are treatment options for gastric decontamination?
Background:1,2
- Elimination is a multi-organ process to rid the body of xenobiotics and their metabolites.
- Most of elimination occurs by the kidneys and liver.
- Clearance is the volume of blood that an organ can clear substance from per unit time.
- The summation of organ-specific clearances equals the total body clearance.
- Half-life is the amount of time it takes for plasma concentrations of a xenobiotic to reduce by half.
- It may be constant (first-order kinetics) or vary by concentration (zero-order kinetics).
- Elimination kinetics can be classified by zero-order, first-order, or Michaelis-Menten kinetics.
Elimination Kinetics:1,2
- See “TOXCards: General Principles of Toxicokinetics” for more information.
- Zero-order kinetics:
- Fixed amount of xenobiotic is eliminated per unit time.
- Examples: ethanol, phenytoin, salicylates, omeprazole, fluoxetine, cisplatin

- First-order kinetics:
- Fixed proportion of xenobiotic is eliminated per unit time.
- A large majority (~95%) substances exhibit first-order kinetics.

- Michaelis-Menten kinetics:
- A non-linear kinetic state with both zero- and first-order kinetics.
- Kinetics are dependent on concentration:
- Low concentrations ([C] <<< km) = first-order kinetics
- High concentrations ([C] >>> km) = zero-order kinetics

Case (continued):
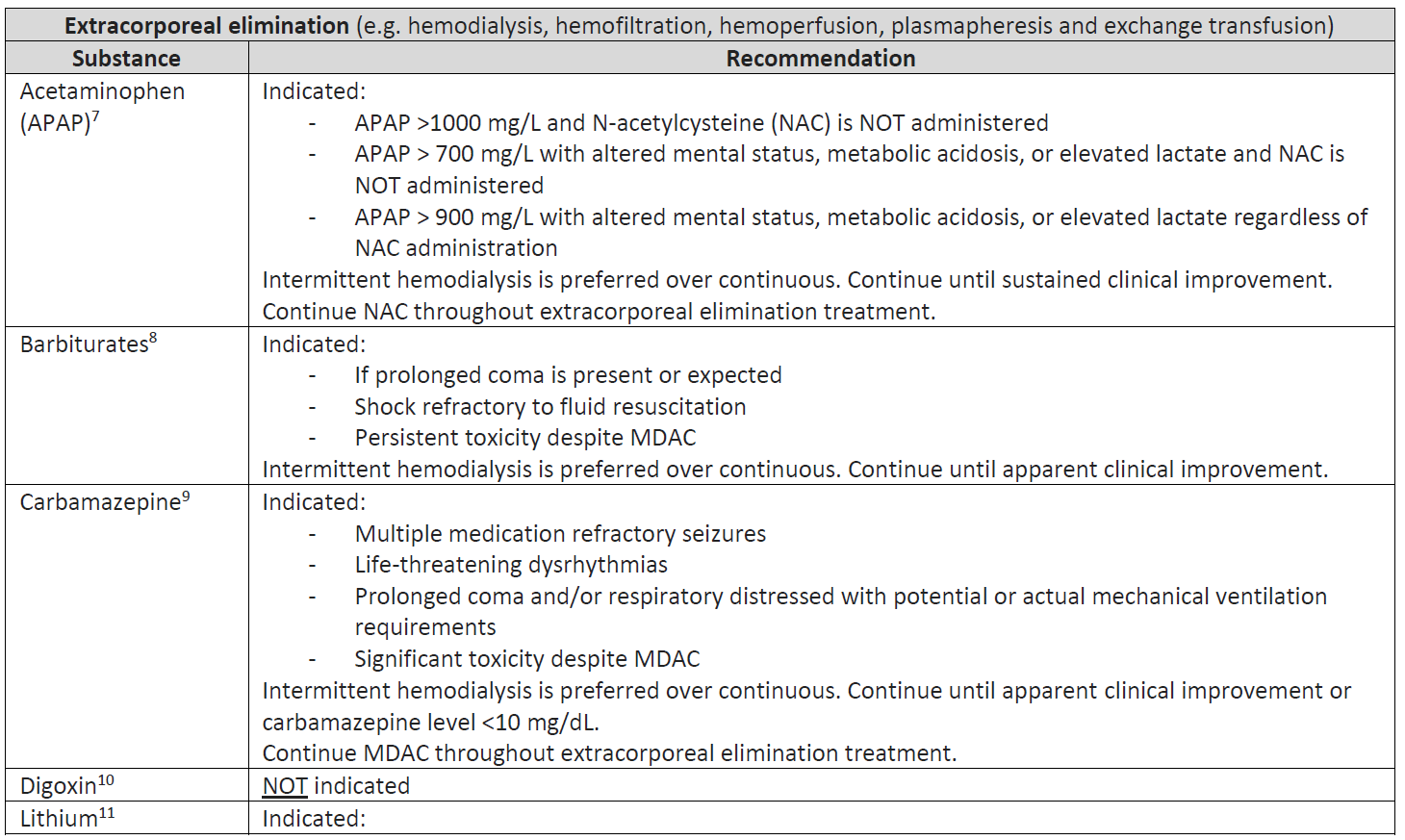
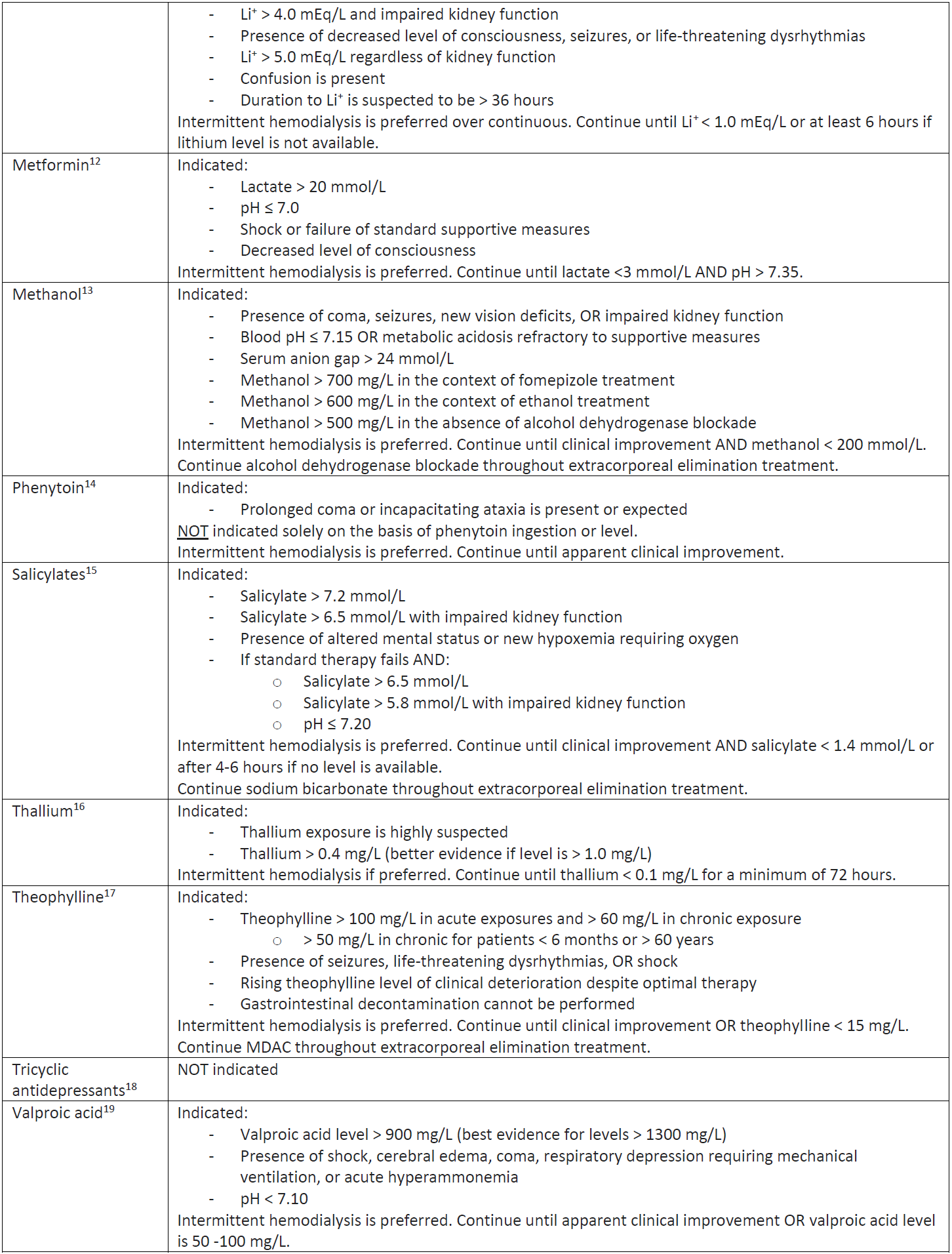
The patient’s parents arrive to the emergency department and endorse that she is on theophylline for chronic asthma control. Her labs resulted a theophylline level of 83 mg/dL. Multi-dose activated charcoal and intermittent hemodialysis are initiated to enhance the elimination of theophylline.
Enhance Elimination Treatments:
Main Point:
- Elimination is a multi-organ process in order to eliminate xenobiotics from the body.
- The elimination kinetics enable us to predict how the plasma concentrations change with respect to ingestion quantity and time.
- However, they can be significantly altered in the setting of toxicological ingestions.
- Substances with zero-order kinetics can show large fluctuations in concentration with small increments in dose.
References/Further Reading:
- Howland MA. Pharmacokinetic and Toxicokinetic Principles. In: Hoffman RS, Howland MA, Lewin NA, Nelson LS, Goldfrank LR, eds. Goldfrank’s Toxicologic Emergencies, 10e. New York, NY: McGraw-Hill Education; 2015.
- Ducharme MP. Drug Elimination, Clearance, and Renal Clearance. In: Shargel L, Yu ABC, eds. Applied Biopharmaceutics & Pharmacokinetics, 7e. New York, NY: McGraw-Hill Education; 2016.
- Goldfarb DS, Ghannoum M. Principles and Techniques Applied to Enhance Elimination. In: Hoffman RS, Howland MA, Lewin NA, Nelson LS, Goldfrank LR, eds. Goldfrank’s Toxicologic Emergencies, 10e. New York, NY: McGraw-Hill Education; 2015.
- American Academy of Clinical Toxicology EAoPC, Toxicologists C. Position statement and practice guidelines on the use of multi-dose activated charcoal in the treatment of acute poisoning. Journal of Toxicology: Clinical Toxicology. 1999;37(6):731-751.
- Thanacoody R, Caravati EM, Troutman B, et al. Position paper update: whole bowel irrigation for gastrointestinal decontamination of overdose patients. Clinical Toxicology. 2015;53(1):5-12.
- Proudfoot A, Krenzelok E, Vale J. Position paper on urine alkalinization. Journal of Toxicology: Clinical Toxicology. 2004;42(1):1-26.
- Gosselin S, Juurlink D, Kielstein J, et al. Extracorporeal treatment for acetaminophen poisoning: recommendations from the EXTRIP workgroup. Clinical toxicology. 2014;52(8):856-867.
- Mactier R, Laliberté M, Mardini J, et al. Extracorporeal treatment for barbiturate poisoning: recommendations from the EXTRIP Workgroup. American Journal of Kidney Diseases. 2014;64(3):347-358.
- Ghannoum M, Yates C, Galvao TF, et al. Extracorporeal treatment for carbamazepine poisoning: systematic review and recommendations from the EXTRIP workgroup. Clinical Toxicology. 2014;52(10):993-1004.
- Mowry JB, Burdmann EA, Anseeuw K, et al. Extracorporeal treatment for digoxin poisoning: systematic review and recommendations from the EXTRIP Workgroup. Clinical Toxicology. 2016;54(2):103-114.
- Decker BS, Goldfarb DS, Dargan PI, et al. Extracorporeal treatment for lithium poisoning: systematic review and recommendations from the EXTRIP Workgroup. Clinical Journal of the American Society of Nephrology. 2015;10(5):875-887.
- Calello DP, Liu KD, Wiegand TJ, et al. Extracorporeal treatment for metformin poisoning: systematic review and recommendations from the Extracorporeal Treatments in Poisoning Workgroup. Critical care medicine. 2015;43(8):1716-1730.
- Roberts DM, Yates C, Megarbane B, et al. Recommendations for the role of extracorporeal treatments in the management of acute methanol poisoning: a systematic review and consensus statement. Critical care medicine. 2015;43(2):461-472.
- Anseeuw K, Mowry JB, Burdmann EA, et al. Extracorporeal treatment in phenytoin poisoning: Systematic review and recommendations from the EXTRIP (extracorporeal treatments in poisoning) workgroup. American Journal of Kidney Diseases. 2016;67(2):187-197.
- Juurlink DN, Gosselin S, Kielstein JT, et al. Extracorporeal treatment for salicylate poisoning: systematic review and recommendations from the EXTRIP workgroup. Annals of Emergency Medicine. 2015;66(2):165-181.
- Ghannoum M, Nolin TD, Goldfarb DS, et al. Extracorporeal treatment for thallium poisoning: recommendations from the EXTRIP Workgroup. Clinical Journal of the American Society of Nephrology. 2012;7(10):1682-1690.
- Ghannoum M, Wiegand TJ, Liu KD, et al. Extracorporeal treatment for theophylline poisoning: systematic review and recommendations from the EXTRIP workgroup. Clinical Toxicology. 2015;53(4):215-229.
- Yates C, Galvao T, Sowinski KM, et al. Extracorporeal treatment for tricyclic antidepressant poisoning: recommendations from the EXTRIP Workgroup. Paper presented at: Seminars in dialysis2014.
- Ghannoum M, Laliberté M, Nolin TD, et al. Extracorporeal treatment for valproic acid poisoning: systematic review and recommendations from the EXTRIP workgroup. Clinical Toxicology. 2015;53(5):454-465.




